Page 2 of 14
SU9.1 | Selection and Interpretation of Surgical Investigations — SDL Guide (Part 2)
Interpreting the Investigative Data in a Surgical Patient
Selecting the test is only half the skill; the harder half is interpreting the result without being misled. The governing rule is that a result updates the pretest probability — it does not replace clinical judgement. Read every result against three questions. First, what was the pretest probability? A positive test in a low-risk patient is far more likely to be a false positive than the same result in a high-risk patient, so a surprising positive in an unlikely setting deserves confirmation, not immediate action. Second, is this a single value or a trend? Many surgical results — tumour markers, inflammatory markers, haemoglobin, renal function — are far more informative as a trend over time than as one snapshot; a single mildly abnormal number is often noise within the normal-range definition, whereas a rising or falling sequence signals real change. Third, does it fit the clinical picture? When a result contradicts a confident clinical assessment, suspect a false positive or false negative, sampling or labelling error, or the wrong test for the question, and either repeat it, confirm it by a different modality, or correlate it with histology. Specific traps to remember: a negative highly-sensitive test is reassuring (SnNOut), but a negative insensitive test does not exclude disease; a positive highly-specific test is convincing (SpPIn), but an isolated positive low-specificity test (such as many tumour markers) is not a diagnosis. Tissue — cytology or, definitively, histopathology — is what ultimately establishes a cancer diagnosis, not a marker or an image alone.
From Pretest Probability to Surgical Management
Applying It: A Worked Surgical Case
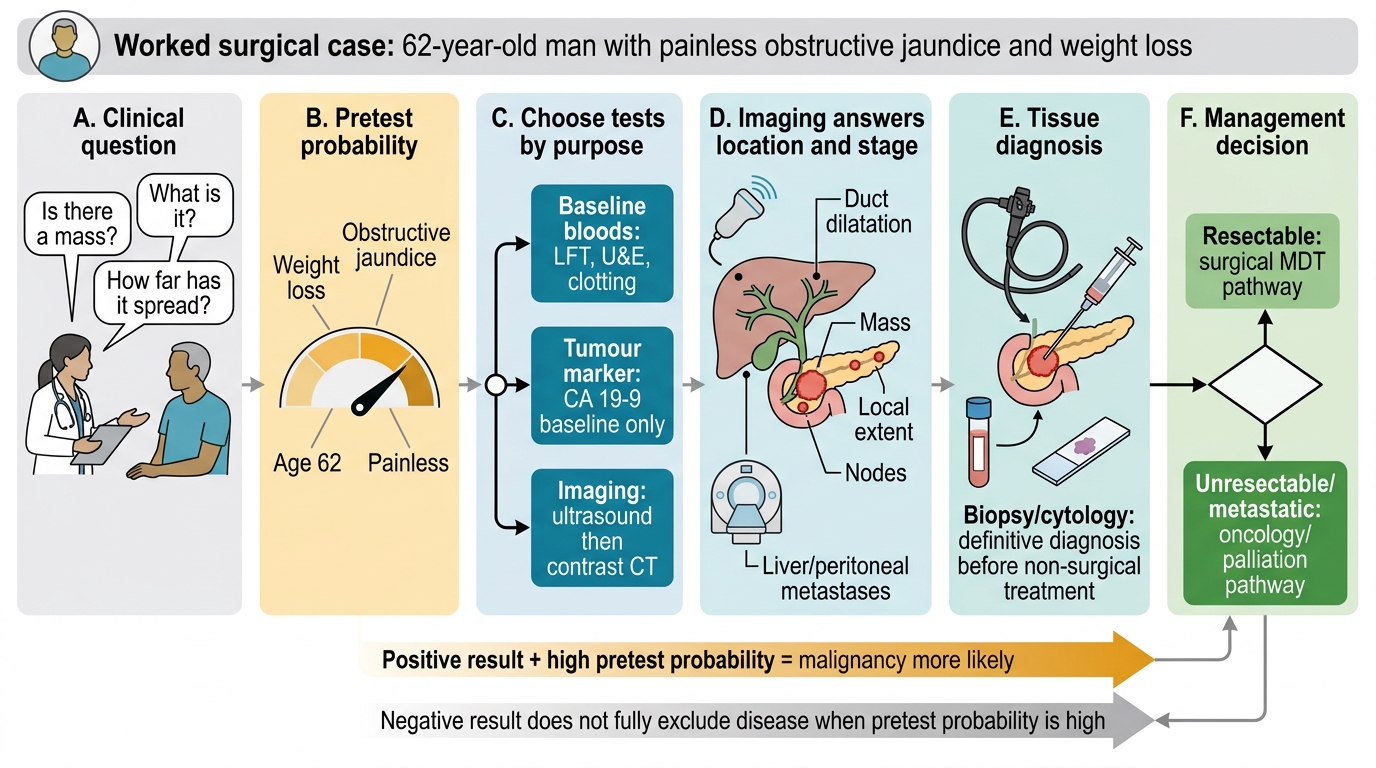
Now apply the whole skill to a case, the way you would on a ward round. A 62-year-old man presents with painless obstructive jaundice and weight loss. Step 1 — the clinical question. History and examination raise a high pretest probability of a pancreatic or peri-ampullary malignancy, so the questions are: is there a mass, what is it, and how far has it spread? Step 2 — select by modality and purpose. Start with biochemical baseline tests — liver function (an obstructive pattern), renal function and clotting — and recognise that a raised CA 19-9 here supports the picture and gives a baseline to monitor later, but is not itself diagnostic and would be meaningless as a screening test in a well person. Choose imaging to answer 'where and how big': ultrasound first (cheap, no radiation, confirms duct dilatation), then a contrast-enhanced CT of the abdomen for the diagnostic detail and, critically, for staging the local extent, nodal status and any liver or peritoneal metastases. Step 3 — tissue. Because management hinges on it, obtain a pathological diagnosis (for example, image- or endoscopy-guided biopsy/cytology) before non-surgical treatment; a tissue diagnosis is the definitive answer that no marker or scan can replace. Step 4 — interpret in context. Read the CT for resectability, correlate the CA 19-9 trend rather than the single value, and confirm that the results fit the clinical story; if the CT were unexpectedly normal in the face of a convincing clinical picture, suspect a false negative and pursue further imaging or tissue rather than reassurance. The investigation pathway has then done its job: it has answered the diagnostic and staging questions needed to decide whether, and how, to operate. Walking a case through these steps — question, pretest probability, modality, tissue, contextual interpretation — is exactly the supervised practice this competency requires.
Check Your Understanding
Consolidate the skill as a repeatable algorithm you can run on any surgical patient. Begin by stating the clinical question and your pretest probability from history and examination — never order a test that cannot change management. Choose the test by performance and modality: use sensitivity and specificity to decide whether you are trying to rule a disease out (a sensitive test, SnNOut) or rule it in (a specific test, SpPIn), and pick the right category — biochemical, microbiological, pathological or imaging — for the question, separating diagnostic from staging from baseline purposes. Remember that predictive values follow pretest probability, which is why tumour markers are for monitoring and not for screening the general population. Then interpret the result in context: weigh it against the pretest probability, prefer a trend over a single value, suspect a false result when it contradicts a confident clinical picture, and reach for tissue (cytology or definitive histopathology) when a diagnosis must be certain. Self-test on four links: can you define sensitivity, specificity, PPV and NPV and say which moves with prevalence; can you match a clinical question to the right modality and purpose; can you state why a tumour marker is not a screening test; and can you describe how you would interpret a surprising positive in a low-risk patient? The questions below check exactly these.
SELF-CHECK
You strongly suspect appendicitis clinically (high pretest probability) but want a test whose NEGATIVE result would most reliably let you safely send the patient home. What property should that test have, and why?
A. High specificity, because a positive result then rules the disease in (SpPIn)
B. High sensitivity, because a negative result then rules the disease out (SnNOut)
C. A high tumour-marker level, because markers exclude inflammation
D. Low pretest probability, because that guarantees a true negative
Reveal Answer
Answer: B. High sensitivity, because a negative result then rules the disease out (SnNOut)
To safely exclude a disease you need a SENSITIVE test: high sensitivity means few false negatives, so a negative result confidently rules the disease out (SnNOut). High specificity is for ruling a disease IN on a positive result (SpPIn). Tumour markers have no role in appendicitis, and pretest probability is set by the clinical picture, not chosen to guarantee an answer.