Page 4 of 15
SU11.3 | Airway Maintenance Skill — SDL Guide
Learning Objectives
- Recognise upper-airway obstruction and explain the anatomy and principles of maintaining a patent airway (SU11.3).
- Demonstrate the graded sequence of airway maintenance — basic manoeuvres, airway adjuncts, bag-mask ventilation, and the principles of supraglottic and definitive airways — on a mannequin or equivalent (SU11.3).
- Interpret the signs that distinguish a patent from an obstructed airway and judge whether an intervention has succeeded (SU11.3).
INSTRUCTIONS
An obstructed airway will kill a patient in minutes, faster than almost any other surgical emergency, and the rescue is a set of hand skills and simple devices that anyone on the team must be able to deploy at once. This module teaches airway maintenance as a graded ladder — recognising obstruction, opening the airway with basic manoeuvres, supporting it with simple adjuncts, ventilating with a bag and mask, and understanding the supraglottic and definitive airways that follow. Because this is a skill, you will rehearse the whole sequence on a mannequin until it is smooth and automatic; the aim is not to memorise a list but to build the muscle memory that keeps a patient alive while help arrives.
References
- Bailey & Love's Short Practice of Surgery, Anaesthesia and the Surgical Patient (textbook)
- SRB's Manual of Surgery, Anaesthesia and Airway Management (textbook)
- Sabiston Textbook of Surgery, Anesthesiology and Airway Management (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A patient slumps unconscious in the recovery bay. Within seconds his breathing turns to a coarse snore, his chest heaves but no air moves, and the oximeter trace begins to fall. Nothing exotic has happened: lying on his back and unconscious, his tongue has simply fallen against the back of his throat and sealed the airway. The cure costs no drug and no machine — a hand under the chin, a lift of the jaw, and the snore stops, the chest fills, the saturation climbs. This is the single most important manual skill in all of medicine, because an airway lost is a life lost in minutes, and an airway opened is a life saved with two hands. Everything else in resuscitation waits behind it.
WHY THIS MATTERS
Airway maintenance is the first priority in every collapsed, anaesthetised, injured or critically ill patient — the 'A' of the ABC approach — because no amount of breathing support or circulation matters if air cannot reach the lungs. As a surgeon you will meet airway emergencies in theatre and recovery, on the ward, in the emergency department and at the bedside of any patient who loses consciousness; you must be able to recognise obstruction instantly and act with your hands and with simple devices before specialist help arrives. The skill is also examined directly and demonstrated on a mannequin precisely because it must be reliable under pressure: there is no time to look it up. Mastering the graded ladder now — open, support, ventilate — and rehearsing it until it is automatic is what will let you keep a patient oxygenated in the few critical minutes that decide the outcome.
RECALL
Recall the knowledge this skill depends on. From the preoperative-assessment learning in this cluster, recall the Mallampati classification and the other predictors of a difficult airway, since anticipating difficulty is part of safe airway management. From anatomy, recall the structure of the upper airway — the oropharynx, the larynx with its vocal cords, the epiglottis, and the trachea below — and the way the tongue and soft tissues can fall back to obstruct it. Recall too, from the same preoperative learning, that loss of consciousness and general anaesthesia abolish the protective airway reflexes (the gag and cough) and the muscle tone that normally keeps the airway open, which is exactly why an unconscious patient so readily obstructs. This anatomical and physiological background is what makes the manoeuvres in this module rational rather than rote.
Why Airway Maintenance Is the First Priority
The clinical indication for airway maintenance is any patient who cannot maintain their own patent airway — the unconscious, the anaesthetised, the injured, the obtunded — and it takes absolute priority because the airway is the first and most time-critical link in the chain of oxygen delivery. The logic is stark and quantitative: the brain tolerates only a few minutes of complete airway obstruction before irreversible hypoxic injury and death, far less time than is available for almost any other emergency intervention. This is why airway is the 'A' in the ABC sequence of resuscitation and is addressed before breathing and circulation: there is no point ventilating or supporting the circulation if air cannot pass into the lungs in the first place. The commonest cause of obstruction in an unconscious supine patient is also the simplest to relieve — the loss of muscle tone lets the tongue fall back against the posterior pharyngeal wall — and the commonest fatal error is failing to recognise and relieve it in time. Airway maintenance is therefore approached as a graded ladder: recognise obstruction, open the airway with basic manoeuvres, support it with simple adjuncts, ventilate with a bag and mask if breathing is inadequate, and escalate to supraglottic or definitive airways as skill and equipment allow. The early rungs need no equipment and can be performed by anyone, which is precisely why every clinician must own them.
Airway Anatomy and the Principles of a Patent Airway
Effective airway maintenance rests on a clear mental picture of the airway and of what obstructs it, so begin with the anatomy. Air passes from the mouth and nose into the pharynx, past the epiglottis and through the larynx — where the vocal cords guard the entrance to the lower airway — and then down the trachea to the lungs. In a conscious person, muscle tone and protective reflexes keep this passage open and protect it from soiling. The governing principle of airway maintenance is therefore simple: keep this passage open and unobstructed, and protect it from aspiration when reflexes are lost. Obstruction in the unconscious patient is most often soft-tissue obstruction — the relaxed tongue and pharyngeal soft tissues falling backwards against the posterior pharyngeal wall when the patient lies supine — which is why lifting the tongue and jaw forward relieves it. Other causes include foreign material (blood, vomit, secretions, or a foreign body), laryngeal problems (laryngospasm, oedema), and swelling from trauma or burns. Every technique in the ladder works on one of these principles: the basic manoeuvres (head-tilt/chin-lift and jaw thrust) pull the tongue and soft tissues forward off the pharyngeal wall; the adjuncts (oropharyngeal and nasopharyngeal airways) hold a channel open behind the tongue; bag-mask ventilation delivers oxygen past a maintained airway; and the supraglottic and definitive airways create a more secure conduit, with the cuffed endotracheal tube additionally protecting against aspiration. Understanding which problem each tool solves is what lets you choose correctly under pressure.
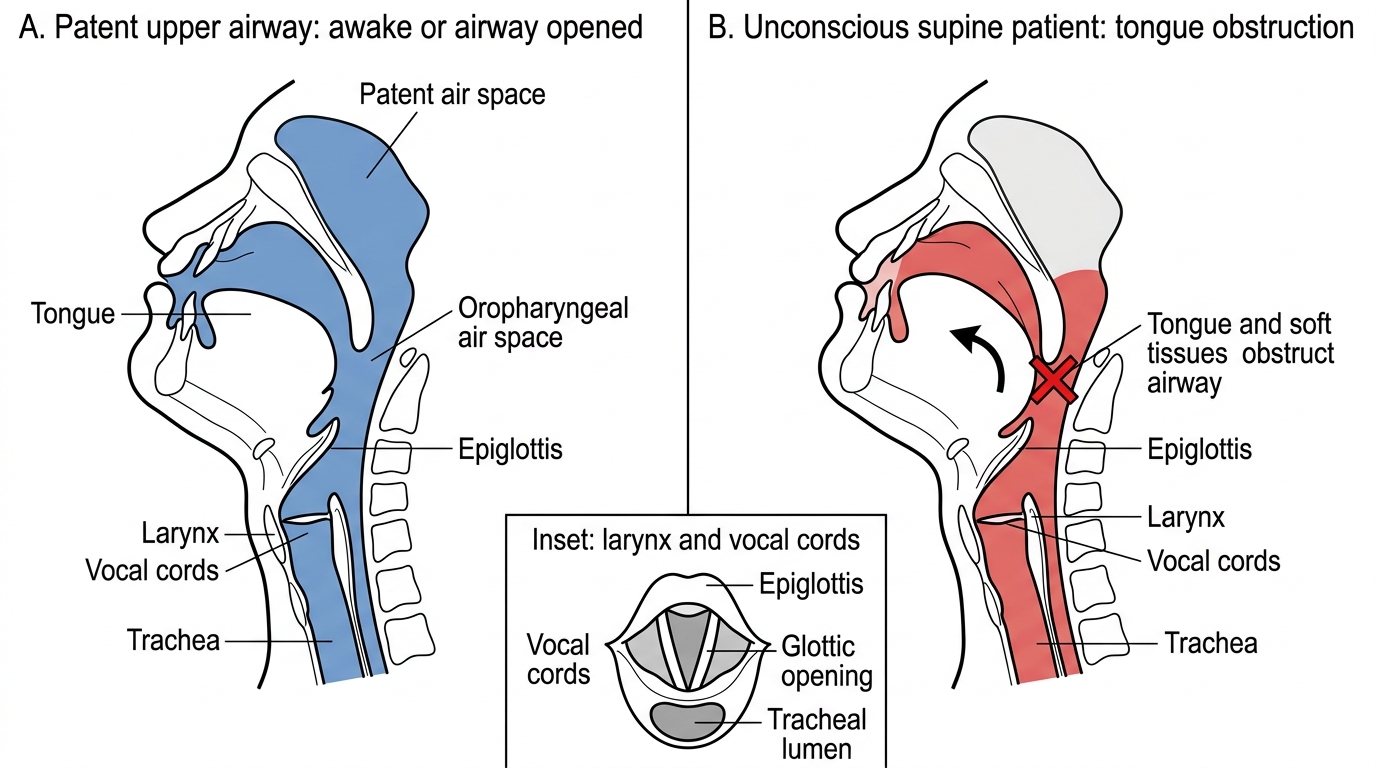
Tongue Obstruction of the Upper Airway in the Unconscious Supine Patient
SELF-CHECK
In an unconscious patient lying supine, what is the single most common cause of upper-airway obstruction?
A. Laryngospasm
B. The tongue and soft tissues falling back against the posterior pharyngeal wall
C. A foreign body lodged in the trachea
D. Swelling of the vocal cords
Reveal Answer
Answer: B. The tongue and soft tissues falling back against the posterior pharyngeal wall
Loss of muscle tone in the unconscious supine patient lets the TONGUE and pharyngeal soft tissues fall back against the posterior pharyngeal wall — the commonest cause of obstruction, and the reason basic manoeuvres (chin-lift, jaw thrust) that pull the tongue forward are so effective. The other causes occur but are far less common.
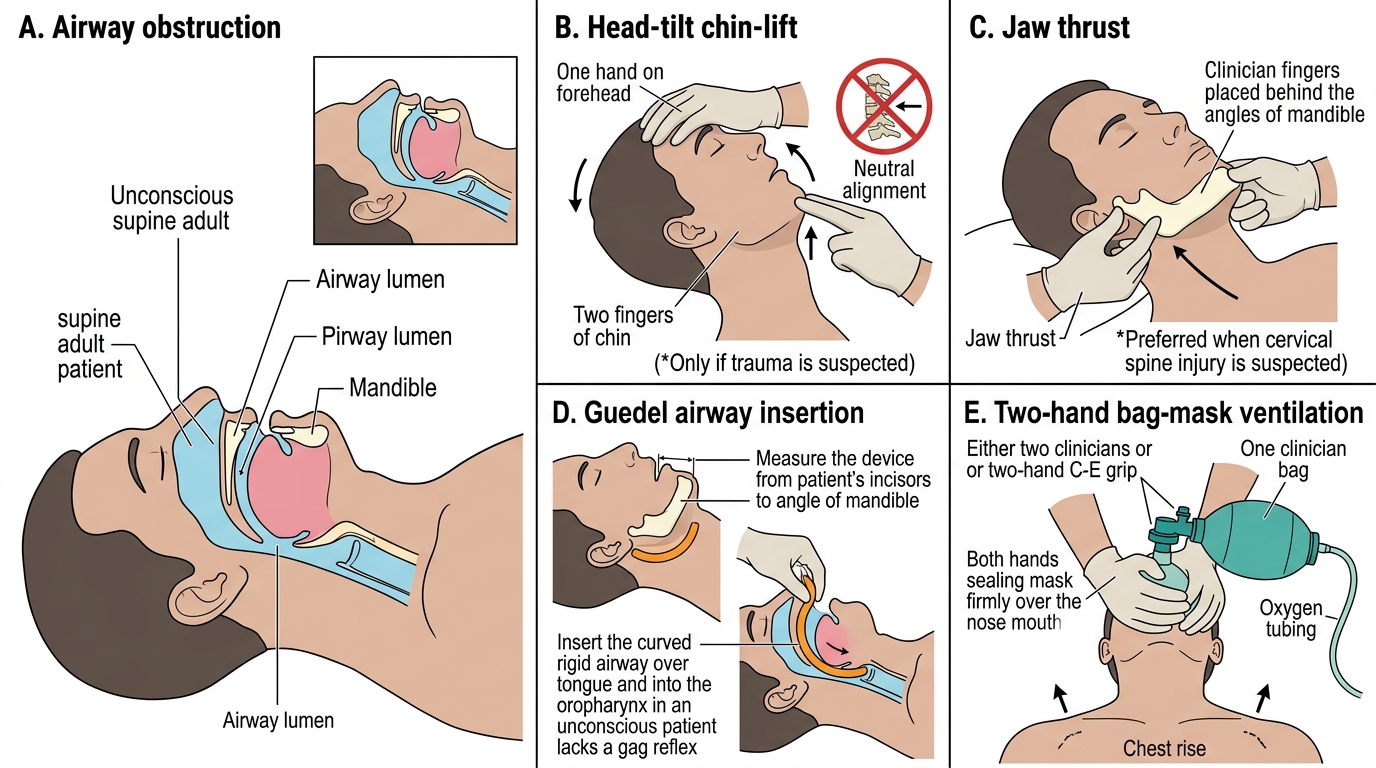
The Airway Maintenance Technique, Step by Step
Airway maintenance is performed as a graded sequence, escalating only as far as the situation and your skill require, and each step builds on the last. First, recognise the problem: approach the patient, ensure your own safety, and assess the airway by look, listen and feel — look for chest and abdominal movement and for cyanosis, listen at the mouth for breath sounds or the noises of obstruction (snoring, gurgling, stridor), and feel for airflow. Second, open the airway with basic manoeuvres. The head-tilt/chin-lift — tilting the head back with one hand on the forehead while lifting the chin with the fingertips of the other — lifts the tongue off the pharyngeal wall and is the default in a patient with no suspected neck injury. Where cervical-spine injury is suspected (trauma), use the jaw thrust instead, lifting the angles of the mandible forward without moving the neck, and clear the mouth of any visible foreign material or secretions (suction if available). Third, support the airway with an adjunct. An oropharyngeal (Guedel) airway, sized from the angle of the mouth to the angle of the jaw, holds a channel open behind the tongue and is used in the deeply unconscious patient who has no gag reflex (it will provoke gagging or vomiting in a patient who is too awake). A nasopharyngeal airway is better tolerated by a semi-conscious patient but is avoided where a base-of-skull fracture is suspected. Fourth, ventilate if breathing is inadequate using bag-mask (bag-valve-mask) ventilation with high-flow oxygen, ideally a two-person, two-hand technique sealing the mask to the face while a maintained airway lets the breaths inflate the chest. Fifth, escalate to a more secure airway as skill and equipment allow: a supraglottic airway — the laryngeal mask airway (LMA) — is inserted blindly to sit over the glottis and allows ventilation without laryngoscopy, but it does not protect against aspiration; the definitive airway is the cuffed endotracheal tube (ETT), passed through the vocal cords under laryngoscopy, which both secures ventilation and protects the lungs from aspiration. Throughout, give oxygen and reassess after every step.
Provided image
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Basic Airway Manoeuvres and Adjuncts
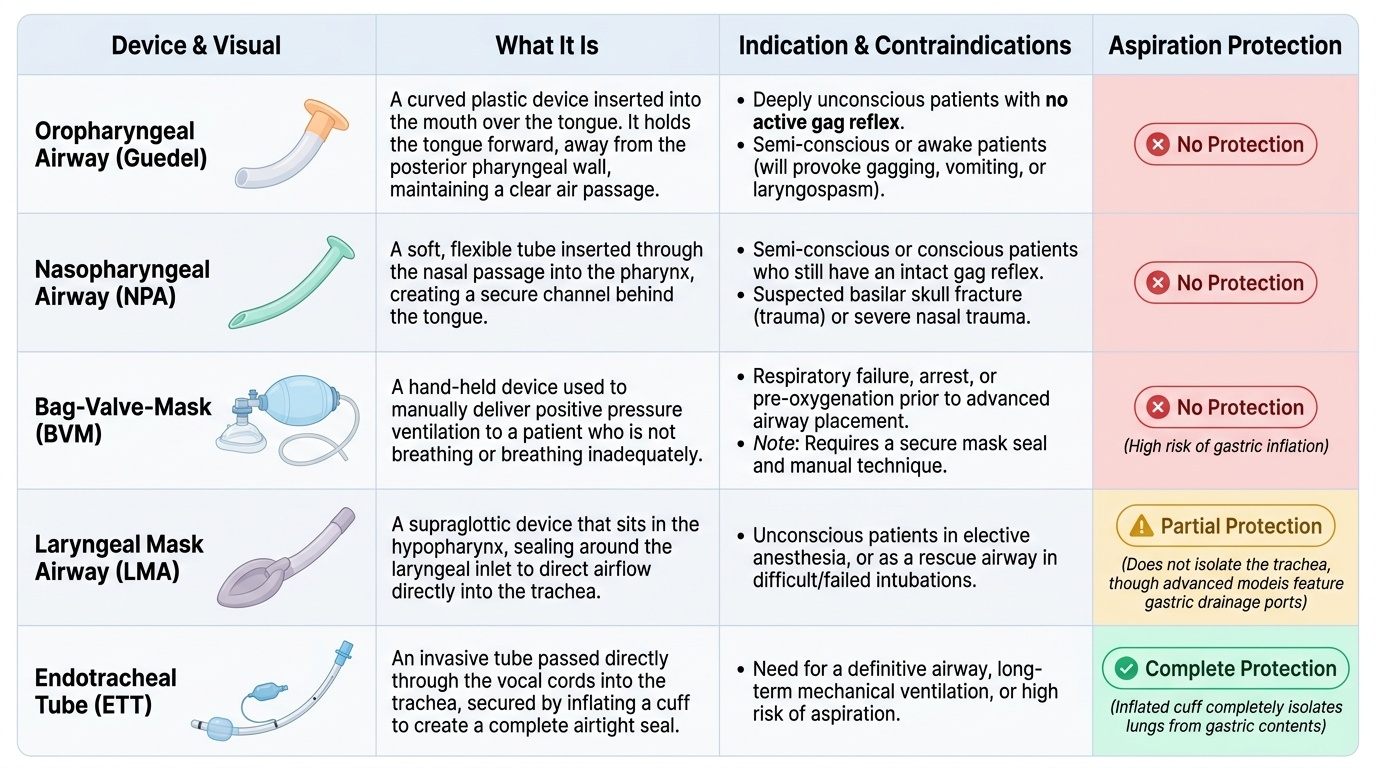
| Device | What it is | Indication | Protects against aspiration? |
|---|---|---|---|
| Oropharyngeal (Guedel) airway | Rigid adjunct behind the tongue | Deeply unconscious, no gag reflex | No |
| Nasopharyngeal airway | Soft tube via the nostril | Semi-conscious; avoid in base-of-skull fracture | No |
| Bag-valve-mask | Self-inflating bag + mask | Inadequate breathing — rescue ventilation | No |
| Laryngeal mask airway (LMA) | Supraglottic device over the glottis | Ventilation without laryngoscopy | No |
| Endotracheal tube (ETT) | Cuffed tube through the cords | Definitive airway; aspiration risk | Yes |