Page 5 of 15
SU11.3 | Airway Maintenance Skill — SDL Guide (Part 2)
Recognising a Patent versus an Obstructed Airway
Performing a manoeuvre is only half the skill; the other half is reading whether the airway is actually open, because an intervention that has not worked must be recognised and corrected at once. The bedside method is look, listen and feel, and you must be able to interpret each. A patent airway shows quiet, unobstructed breathing with visible, symmetrical chest rise, audible normal breath sounds at the mouth, and felt airflow; when you are ventilating, the chest rises with each breath. An obstructed airway declares itself by the absence of these signs and by added noises that localise the problem: snoring suggests soft-tissue (tongue) obstruction relievable by basic manoeuvres; gurgling suggests fluid (secretions, blood, vomit) needing suction; stridor suggests laryngeal-level narrowing (laryngospasm, oedema, foreign body); and complete obstruction is ominously silent — paradoxical 'see-saw' chest and abdominal movement with no air entry and no sound at all, the most dangerous pattern of all. The interpretation drives the next action: a snore means lift the jaw or insert an oral airway; a gurgle means suction; a silent see-saw means urgent escalation. Where the patient has been intubated, the gold-standard confirmation that the endotracheal tube is correctly placed in the trachea (and not the oesophagus) is capnography — a sustained end-tidal carbon-dioxide waveform — supported by seeing symmetrical chest rise and hearing equal bilateral breath sounds. Continuous reassessment after every step is the discipline that turns a manoeuvre into a maintained airway.
Provided image
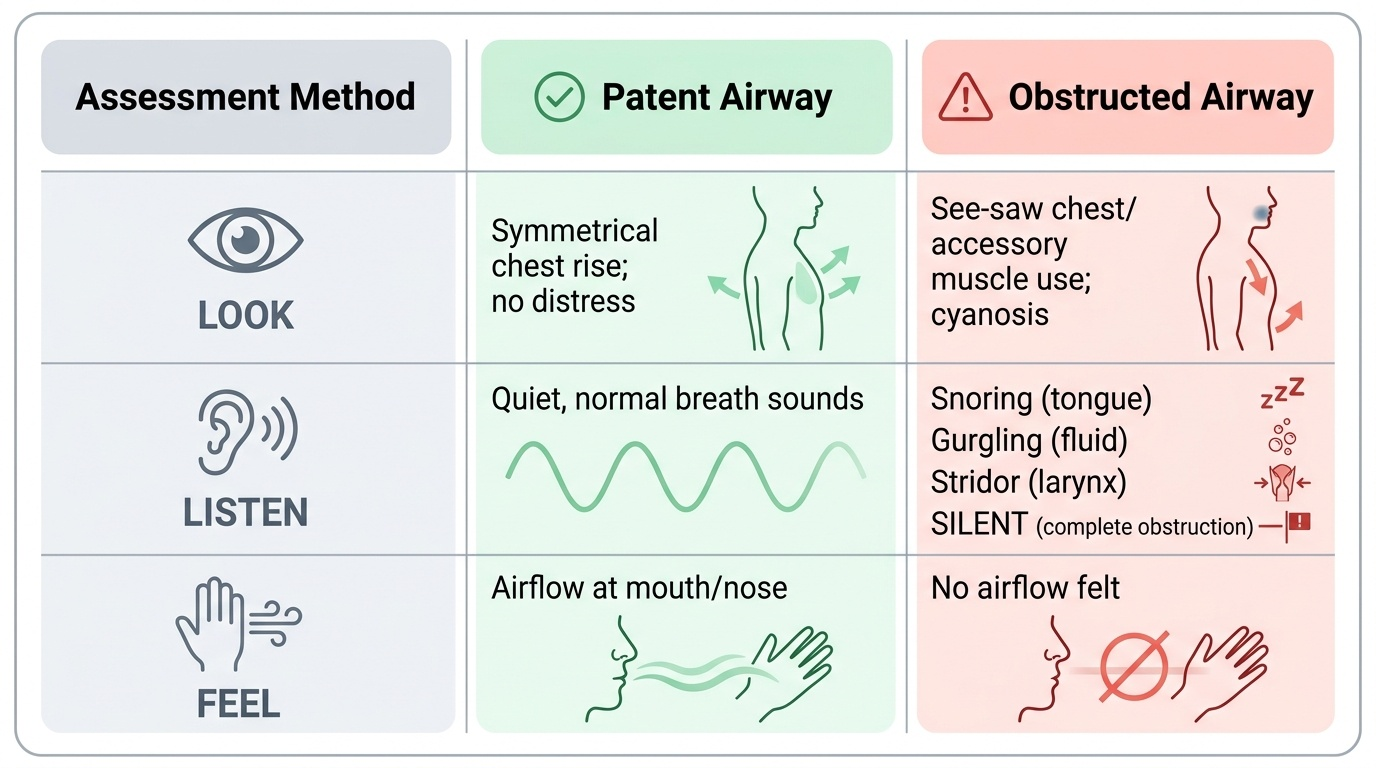
| Sign | Patent airway | Obstructed airway |
|---|---|---|
| Look | Symmetrical chest rise; no distress | See-saw chest/abdomen; accessory muscle use; cyanosis |
| Listen | Quiet normal breath sounds | Snoring (tongue), gurgling (fluid), stridor (larynx), or SILENT (complete) |
| Feel | Airflow at mouth/nose | No airflow felt |
Practising Airway Maintenance on the Mannequin
Because this is a competency to be demonstrated, the knowledge above must be turned into smooth hand skills, and the place to do that safely is the simulation mannequin. Practise the whole sequence repeatedly under supervision until each step is automatic and flows into the next. Begin every run the same way: ensure safety, then assess with look-listen-feel. Open the airway with a head-tilt/chin-lift, switching deliberately to a jaw thrust in the scenario where neck injury is flagged, and verify that the chest now moves and the obstructed noise clears. Size and insert an oropharyngeal airway correctly — measuring from the angle of the mouth to the angle of the jaw, inserting it upside-down and rotating it into place over the tongue (or inserting it the right way up with a tongue depressor in the manikin) — and confirm it has improved, not worsened, the airway. Deliver bag-mask ventilation: select the right mask size, achieve a leak-free seal (practise both the one-hand 'EC' grip and the two-person technique), attach oxygen, and watch for visible chest rise with each squeeze, ventilating at a controlled rate without over-inflation. Rehearse suctioning a simulated obstruction and recognising when to escalate. Where the mannequin and supervision allow, practise inserting a laryngeal mask airway, understanding that it secures ventilation but not aspiration, and observe or simulate the steps of endotracheal intubation with capnographic confirmation. Throughout, reassess after every step and verbalise what you are doing and why. Deliberate, repeated, supervised practice is what builds the reliable, unhurried competence that a real airway emergency demands.
CLINICAL PEARL
Complete airway obstruction is SILENT — there is no snore, no stridor, no breath sound, just paradoxical see-saw movement of the chest and abdomen and a falling saturation. Noise means air is still moving past a partial obstruction; the truly frightening airway makes no sound at all. Never be reassured by silence. And remember the device hierarchy on aspiration protection: an oropharyngeal airway, a nasopharyngeal airway, a bag-mask and even a laryngeal mask airway all keep a patient ventilated but do NOT protect against aspiration — only a cuffed endotracheal tube does that.
Check Your Understanding
Consolidate the skill by mentally walking the airway ladder from collapse to a maintained airway. Start by recognising the problem with look, listen and feel, interpreting the added noises — snoring means the tongue, gurgling means fluid, stridor means the larynx, and an ominous silence with see-saw movement means complete obstruction. Open the airway with a head-tilt/chin-lift, or a jaw thrust when cervical-spine injury is suspected, pulling the tongue off the pharyngeal wall. Support it with an adjunct — an oropharyngeal (Guedel) airway sized angle-of-mouth to angle-of-jaw for the patient with no gag reflex, or a nasopharyngeal airway for the semi-conscious patient (avoided in base-of-skull fracture). Ventilate inadequate breathing with bag-mask and oxygen, watching for chest rise. Escalate to a laryngeal mask airway (ventilates but does not protect against aspiration) or a cuffed endotracheal tube (the definitive airway that does protect against aspiration, confirmed by capnography). Self-test on four links: can you name the commonest cause of obstruction in the unconscious patient and the manoeuvre that relieves it; can you size and state the indication for an oropharyngeal versus a nasopharyngeal airway; can you list the airway devices in order and say which one protects against aspiration; and can you interpret look-listen-feel to tell a patent from an obstructed airway? The questions here check exactly these.
SELF-CHECK
A team has just ventilated a patient with a laryngeal mask airway (LMA) and is maintaining good oxygen saturations. Which statement about the LMA is correct?
A. The LMA is a definitive airway that protects against aspiration
B. The LMA is a supraglottic device that ventilates the patient but does NOT protect against aspiration
C. The LMA must be inserted through the vocal cords under laryngoscopy
D. The LMA is only used in patients with an intact gag reflex
Reveal Answer
Answer: B. The LMA is a supraglottic device that ventilates the patient but does NOT protect against aspiration
The laryngeal mask airway is a SUPRAGLOTTIC device that sits over the glottis and allows ventilation without laryngoscopy, but it does NOT protect against aspiration — only a cuffed endotracheal tube (passed through the cords) is a definitive aspiration-protecting airway. The LMA is used in the unconscious patient, not one with an intact gag reflex.