Page 7 of 15
SU11.4-5 | Daycare Surgery and Pain Management — SDL Guide
Learning Objectives
- Enumerate the indications and principles of daycare (ambulatory) general surgery, including patient, procedure and social selection criteria and discharge criteria (SU11.4).
- Describe the principles of post-operative pain relief — the WHO analgesic ladder, multimodal and pre-emptive analgesia (SU11.5).
- Describe the principles of managing chronic pain, including the biopsychosocial model and the role of adjuvant drugs (SU11.5).
INSTRUCTIONS
A great deal of modern surgery sends the patient home the same day, and almost all surgery causes pain that must be controlled humanely and effectively. This module covers two everyday surgical disciplines: daycare (ambulatory) surgery — who it suits, how the pathway is run, and when the patient is safe to discharge — and the management of pain, both the acute pain that follows an operation and the chronic pain that can persist long after. You will learn the selection and discharge criteria that make day-case surgery safe, and the principles of analgesia — the WHO ladder, multimodal and pre-emptive analgesia for acute pain, and the biopsychosocial, multidisciplinary approach to chronic pain — that make recovery comfortable.
References
- Bailey & Love's Short Practice of Surgery, Day-case Surgery and Postoperative Care (textbook)
- SRB's Manual of Surgery, Day Care Surgery and Pain Management (textbook)
- Sabiston Textbook of Surgery, Ambulatory Surgery and Acute Postoperative Pain (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A young woman arrives at 7 a.m. for an inguinal hernia repair, walks into theatre after a chat with the surgeon and anaesthetist, has her operation, eats lunch, and is driven home by her husband before the afternoon is out — comfortable, with a clear instruction sheet and a phone number to call. The same operation a generation ago would have meant several nights in a hospital bed. What changed was not the operation but the system around it: careful selection of the right patient and procedure, anaesthesia chosen for a quick clear-headed recovery, and — crucially — pain that was anticipated and controlled before it ever became severe. Daycare surgery and good pain control are two sides of the same modern principle: do the operation well, keep the patient comfortable, and let them recover at home where they would rather be.
WHY THIS MATTERS
Daycare surgery and effective pain management are central to contemporary surgical practice and to the experience of nearly every surgical patient you will look after. A large and growing share of elective operations are now done as day cases, which frees beds, reduces hospital-acquired infection, lowers cost and is preferred by most patients — but only when the patient, the procedure and the home circumstances are correctly selected and clear discharge criteria are met, or it becomes unsafe. Pain control matters for every patient: poorly treated acute pain is not merely unkind, it impairs breathing and mobilisation, delays recovery, and can contribute to the development of chronic pain. As a clinician you will select patients for day surgery, judge when they are fit to go home, and prescribe and review analgesia daily; doing both well is humane, improves outcomes and is directly examined. These are core, practical competencies, not optional refinements.
RECALL
Recall the knowledge this skill builds on. From the preoperative-assessment learning in this cluster, recall the ASA physical status classification and the structured preoperative assessment, because patient selection for daycare surgery rests on exactly this risk evaluation. Recall too, from the same learning, the principles of regional and local anaesthesia — spinal and epidural blocks, peripheral nerve blocks, and local infiltration — since these techniques are key components both of day-case anaesthesia and of multimodal pain relief. From pharmacology, recall the actions and adverse effects of the main analgesic classes — paracetamol, the non-steroidal anti-inflammatory drugs (NSAIDs) and the opioids — and the adjuvant drugs used for neuropathic pain. This pharmacological and anaesthetic background is what makes the analgesic principles in this module rational, and the assessment background is what makes daycare selection safe.
Why Daycare Surgery and Good Pain Control Matter
The clinical relevance of these two topics is broad because they touch almost every surgical patient. Daycare surgery — also called ambulatory or day-case surgery — means the patient is admitted, operated on and discharged on the same calendar day, without an overnight stay. It is indicated for the large category of minor and intermediate operations that are short, carry a low risk of major bleeding or other serious early complications, and whose recovery can safely continue at home. Done in the right patients it brings real benefits: efficient use of scarce inpatient beds, a lower risk of hospital-acquired infection and venous thromboembolism, reduced cost, shorter waiting lists, and a recovery in the patient's own home, which most patients prefer. Pain management is the necessary partner of all surgery, day-case or inpatient, because every operation produces tissue injury and pain. Controlling that pain is not only humane; uncontrolled acute pain has real physiological harms — it splints breathing and predisposes to chest complications, discourages early mobilisation and so raises the risk of venous thromboembolism, drives a stress response, and, if poorly managed, can sensitise the nervous system and contribute to the development of chronic pain. The two topics meet directly in day surgery, where effective, opioid-sparing analgesia is precisely what allows a patient to be comfortable enough to go home the same day. The rest of this module sets out the selection and discharge principles that make daycare safe, and the analgesic principles that make recovery comfortable.
Principles and Selection Criteria for Daycare Surgery
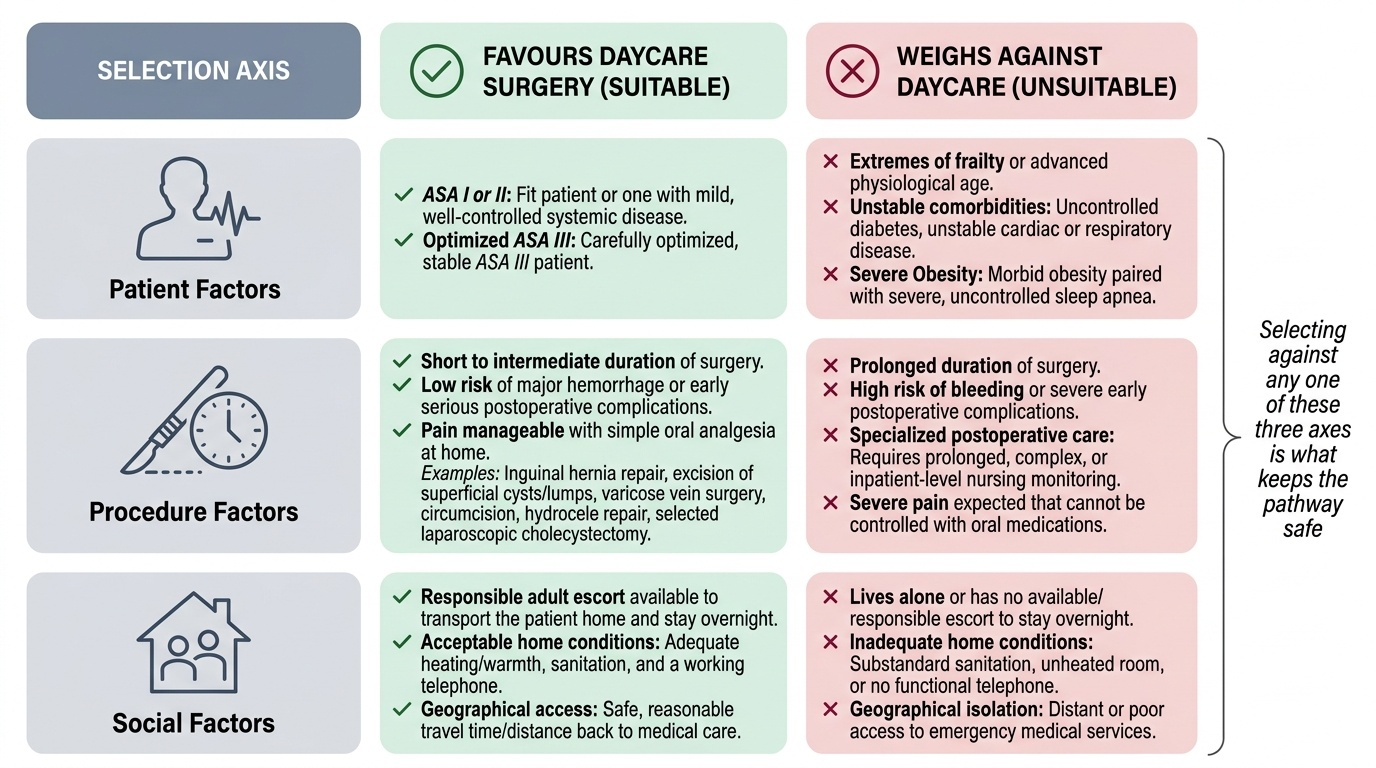
The safety of daycare surgery rests entirely on selection, so the governing principle is to admit only patients in whom same-day discharge can be predicted to be safe and comfortable, judged across three groups of factors. Patient factors: the patient should generally be ASA I or II (a fit patient or one with mild, well-controlled systemic disease), although a carefully optimised, stable ASA III patient may be suitable; extremes of frailty, unstable or poorly controlled comorbidity (uncontrolled diabetes, unstable cardiac or respiratory disease) and morbid obesity with sleep apnoea weigh against day surgery. Procedure factors: the operation should be of short to intermediate duration, carry a low risk of major haemorrhage or other serious early postoperative complications, not require prolonged specialised postoperative care, and have pain that is controllable with oral analgesia at home — typical examples include inguinal hernia repair, excision of superficial lumps and cysts, varicose vein surgery, circumcision, hydrocele repair, and laparoscopic cholecystectomy in selected patients. Social factors: the patient must have a responsible adult escort to take them home and stay overnight, acceptable home conditions (warmth, sanitation, a telephone), and reasonable access back to medical care should a problem arise. Suitable anaesthesia — short-acting agents, regional or local techniques that allow a clear-headed, pain-controlled recovery — and good preoperative optimisation complete the picture. Selecting against any one of these three axes is what keeps the pathway safe; a perfect candidate on patient and procedure grounds is still unsuitable if they would go home alone to an unheated room with no telephone.
Provided image
| Axis | Favours daycare | Weighs against |
|---|---|---|
| Patient | ASA I–II (or stable, optimised III) | Unstable/uncontrolled comorbidity; significant sleep apnoea |
| Procedure | Short/intermediate, low bleeding risk, oral-analgesia pain (hernia, lumps, varicose veins, hydrocele) | Long, high-bleeding-risk, needs specialised postoperative care |
| Social | Responsible escort, safe home, telephone, access to care | Lives alone with no escort; unsafe home; no access to help |
SELF-CHECK
Which of the following best fits the principles of patient selection for daycare (day-case) surgery?
A. Any patient, regardless of comorbidity, provided the operation is finished by midday
B. An ASA I–II patient (or a stable, optimised ASA III) having a short, low-bleeding-risk procedure, with a responsible escort and a safe home
C. Only ASA IV patients, because they benefit most from avoiding hospital
D. A patient living alone with no telephone, provided they feel well
Reveal Answer
Answer: B. An ASA I–II patient (or a stable, optimised ASA III) having a short, low-bleeding-risk procedure, with a responsible escort and a safe home
Daycare selection balances PATIENT factors (ASA I–II, or stable optimised III), PROCEDURE factors (short, low risk of major bleeding/complications, pain controllable with oral analgesia), and SOCIAL factors (responsible escort, safe home, telephone, access to care). A patient living alone with no telephone fails the social criteria even if otherwise fit; ASA IV and 'any patient' ignore the safety basis of selection.
Running a Daycare List: Pathway and Discharge Criteria
Once a patient is correctly selected, the day-case pathway runs as a streamlined version of the standard surgical pathway, and the discipline lies in its preparation and its discharge. Preoperatively, the patient is assessed and optimised in advance (often in a dedicated pre-assessment clinic), given clear instructions including fasting and which regular medications to take, and consented — so that on the day there are no surprises that would cancel or delay the case. On admission, identity, consent, site and fasting are reconfirmed (the same safe-surgery discipline as any operation). Intraoperatively, anaesthesia is chosen for a rapid, clear-headed recovery — short-acting general anaesthetic agents, or regional and local techniques — and multimodal, opioid-sparing analgesia is started, including local-anaesthetic infiltration or a regional block where appropriate, so the patient wakes comfortable. In recovery, the patient is observed until they meet explicit discharge criteria before being allowed home. Discharge is permitted only when: vital signs are stable and have been so for an adequate period; the patient is alert and orientated, able to walk (at their normal baseline) and not unduly dizzy; pain and nausea are controlled on oral medication; the patient can tolerate oral fluids and has passed urine where required (e.g. after pelvic or regional anaesthesia); there is no undue bleeding from the wound; a responsible adult escort is present to take them home and stay; and the patient is given written instructions, take-home analgesia, and a contact number for problems. Discharging against any one of these criteria is what turns a safe day case into an unsafe one — the criteria are a checklist, not a guideline to be eyeballed.
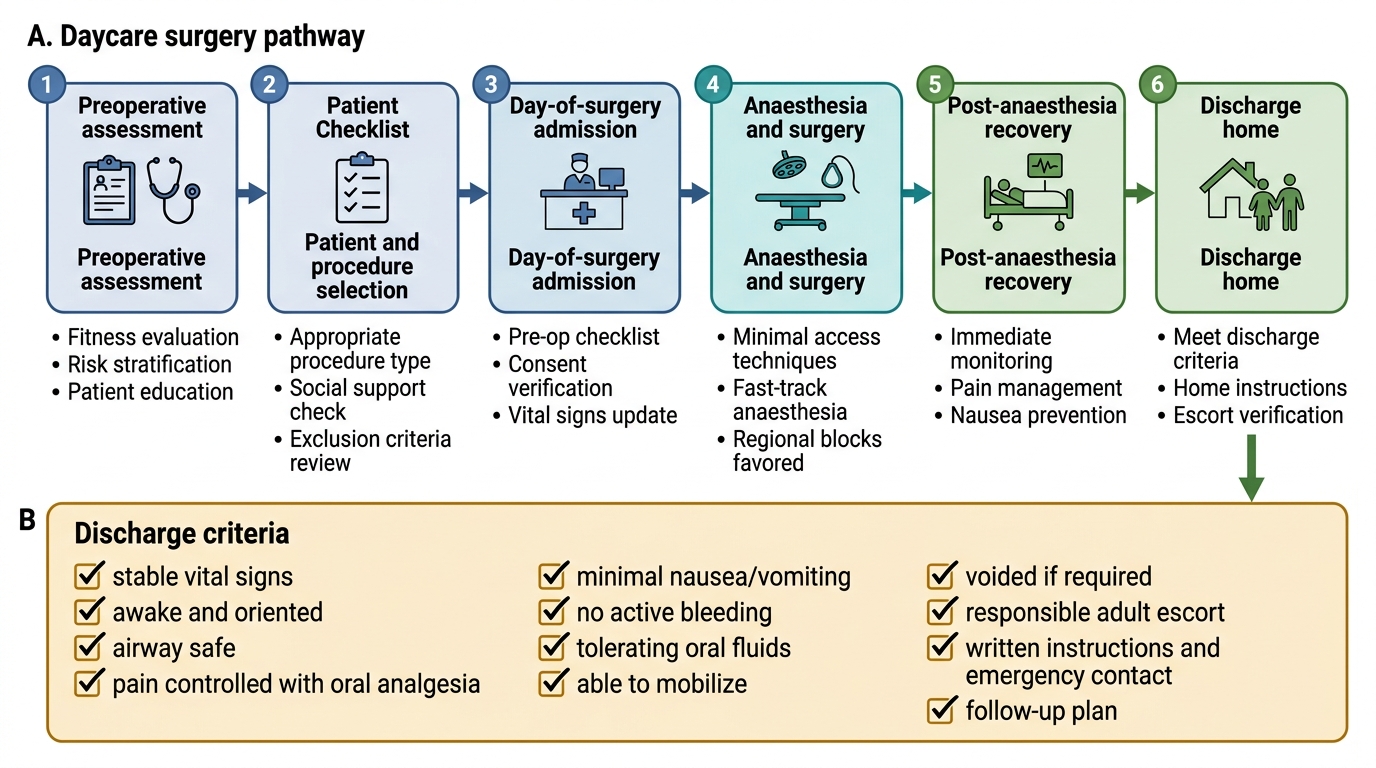
Daycare Surgery Pathway and Discharge Criteria