Page 8 of 15
SU11.4-5 | Daycare Surgery and Pain Management — SDL Guide (Part 2)
Principles of Post-operative Pain Management
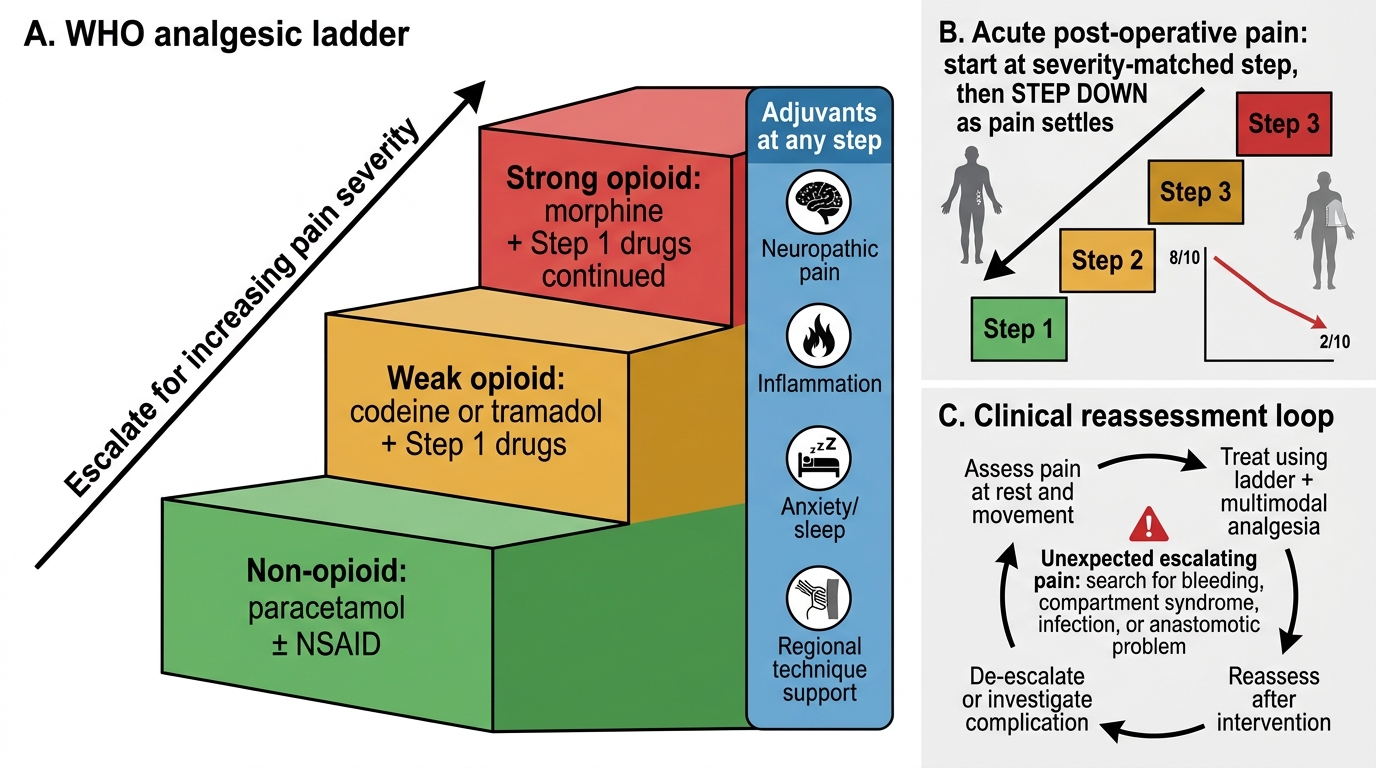
Post-operative pain should be anticipated and prevented, not merely treated once it is severe, and three principles guide its management. The first is the WHO analgesic ladder, originally devised for cancer pain, which grades drugs by potency: step 1 is a non-opioid (paracetamol and, where not contraindicated, an NSAID); step 2 adds a weak opioid such as codeine or tramadol; and step 3 uses a strong opioid such as morphine. For chronic and cancer pain the ladder is climbed upwards as pain worsens, but for acute post-operative pain the ladder is applied in reverse — you start at the step that matches the (predictably severe) early pain and step down as the pain settles over the following days. The second principle is multimodal analgesia: combining drugs from different classes and routes that act by different mechanisms — paracetamol plus an NSAID plus an opioid plus a local-anaesthetic infiltration or regional block — so their effects are additive, each is needed in a smaller dose, and the total opioid requirement (and so opioid side-effects such as sedation, nausea and respiratory depression) is reduced. This opioid-sparing effect is exactly what allows comfortable early discharge in day surgery. The third principle is pre-emptive analgesia: giving analgesia before the painful stimulus — for example infiltrating the wound with local anaesthetic before incision, or giving paracetamol and an NSAID before the operation — on the rationale that blunting the initial nociceptive barrage reduces both early pain and central sensitisation. Used together, these principles deliver better pain relief with fewer side-effects than any single strong drug given reactively.
WHO Three-Step Analgesic Ladder
- Step 1 — non-opioid: paracetamol ± NSAID.
- Step 2 — weak opioid: codeine or tramadol, added to step 1.
- Step 3 — strong opioid: morphine, with step-1 drugs continued.
- Acute post-op: start at the step matching severity and step DOWN as pain settles.
Assessing Pain and Tailoring the Plan; Managing Chronic Pain
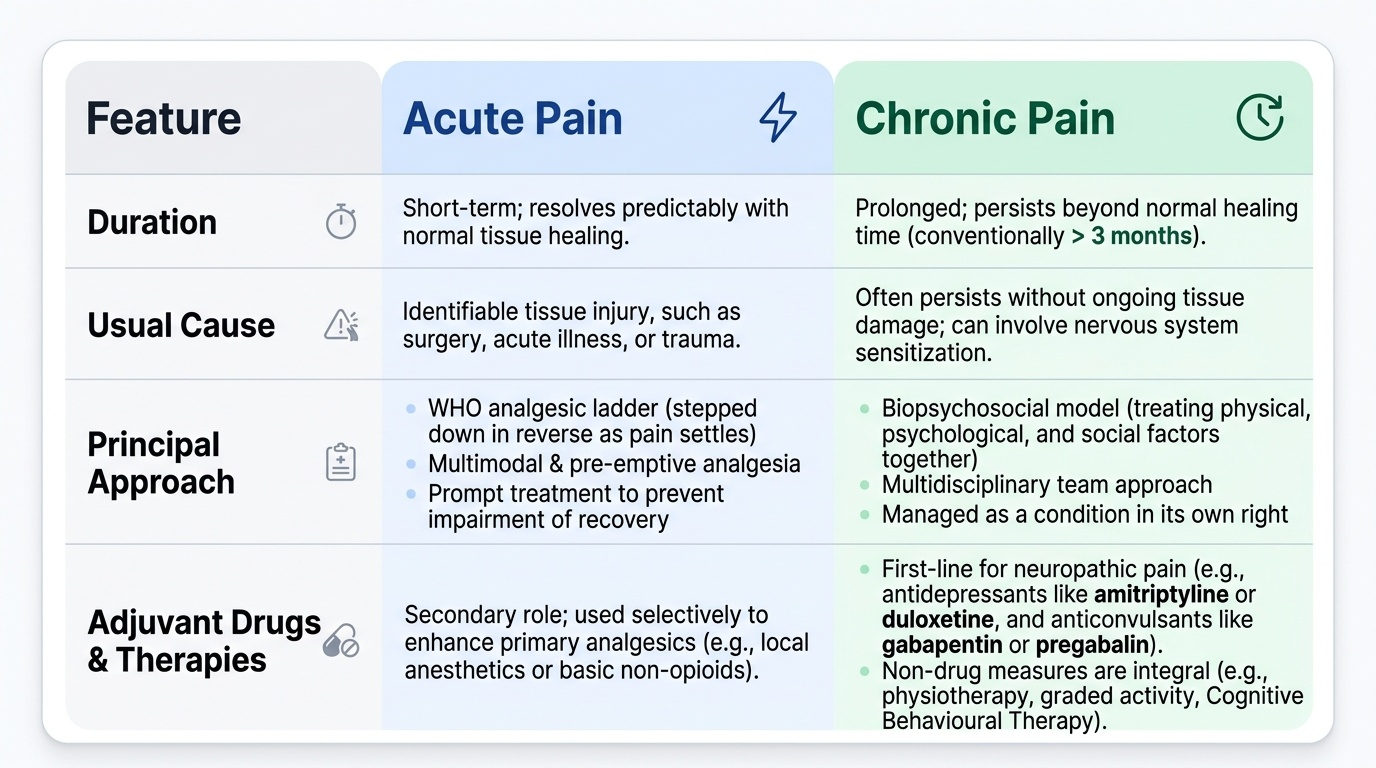
An analgesic plan is only as good as the assessment that drives it, so pain must be measured and reassessed, and the plan adjusted to the response. Pain is assessed with a simple validated tool — a numerical rating or visual analogue scale, or a faces scale in children — at rest and on movement (since pain on coughing or mobilising is what impairs recovery), and reassessed after each intervention. The findings are then interpreted: pain controlled at rest but severe on movement calls for a stronger or multimodal regimen and regional techniques; pain that escalates unexpectedly must prompt a search for a complication (bleeding, compartment syndrome, infection, an anastomotic problem) rather than simply more analgesia — escalating pain is a clinical sign, not just a prescribing problem. As acute pain settles, the plan is de-escalated down the ladder. Chronic pain is a different entity: pain that persists beyond the time of normal tissue healing, conventionally taken as more than about three months, and often without ongoing tissue damage. It does not respond well to the acute model and is managed on the biopsychosocial model — addressing physical, psychological and social contributors together through a multidisciplinary team. Its pharmacology is multimodal and frequently relies on adjuvant analgesics: antidepressants (such as amitriptyline or duloxetine) and anticonvulsants (such as gabapentin or pregabalin) are first-line for neuropathic pain, where conventional analgesics alone are often inadequate. Non-drug measures — physiotherapy, graded activity, psychological therapies such as cognitive behavioural therapy, and interventional techniques — are integral rather than optional. The key interpretive shift is that chronic pain is managed as a condition in its own right, not as an acute pain that has simply lasted too long.
Provided image
| Feature | Acute pain | Chronic pain |
|---|---|---|
| Duration | Short, resolves with healing | Beyond normal healing (>~3 months) |
| Usual cause | Tissue injury (surgery, trauma) | Often persists without ongoing tissue damage |
| Principal approach | WHO ladder (in reverse), multimodal, pre-emptive | Biopsychosocial, multidisciplinary |
| Adjuvant drugs | Sometimes | Central — antidepressants, anticonvulsants for neuropathic pain |
Applying Daycare and Analgesia Principles to a Case
Bring the principles together by working a representative case from selection to comfortable discharge, the way you would on a real list. Consider a fit 40-year-old man with a reducible inguinal hernia, no significant comorbidity, who lives with his wife five minutes from the hospital. Selection: he is ASA I (patient factor), the operation is short with a low risk of major bleeding and pain controllable orally (procedure factor), and he has a responsible escort, a safe home and a telephone (social factors) — he is a good day-case candidate. Preoperative preparation: he is pre-assessed, optimised, consented, and given fasting and medication instructions. Anaesthesia and pre-emptive analgesia: a plan is made for a short-acting general or regional anaesthetic, and pre-emptive, multimodal analgesia is started — for example paracetamol and an NSAID before surgery and local-anaesthetic infiltration of the wound before or at incision — so that he wakes comfortable and needs little opioid. Post-operative analgesia: he continues regular paracetamol and an NSAID (a multimodal, opioid-sparing base), with a weak opioid available for breakthrough pain, applying the ladder in reverse and de-escalating as the pain settles. Discharge: he is allowed home only when he meets the discharge criteria — stable vital signs, alert and mobile, pain and nausea controlled on oral medication, tolerating fluids, passed urine, no undue bleeding, escort present — and he leaves with written instructions, take-home analgesia and a contact number. Had he instead been an unstable ASA III patient, or had no escort, the safe decision would have been an inpatient pathway. This worked example is the template you will apply, with the specifics changed, to every day-case patient.
CLINICAL PEARL
Unexpectedly escalating post-operative pain, or pain that needs far more analgesia than the operation should cause, is a CLINICAL SIGN of a complication — reaching for bleeding, compartment syndrome, infection or an anastomotic leak — not simply a cue to prescribe more opioid. Assess the patient before you escalate the drugs. And remember the direction of the WHO ladder: for chronic/cancer pain you climb UP as pain worsens, but for acute post-operative pain you start at the step matching the early severe pain and step DOWN as it settles — the same ladder, used in opposite directions.