Page 1 of 15
SU11.{1-2,6} | Preoperative Assessment and Safe Anaesthesia Principles — SDL Guide
Learning Objectives
- Describe the principles of preoperative assessment, including history, examination, ASA physical status grading, fasting guidance and risk optimisation (SU11.1).
- Enumerate the principles of general, regional and local anaesthesia, including their definitions, sites of action and main risks (SU11.2).
- Describe the principles of safe general surgery, including the WHO Surgical Safety Checklist and team-based error prevention (SU11.6).
INSTRUCTIONS
Most perioperative harm is anticipated, not random — it follows from a patient hazard missed before the operation, an anaesthetic chosen without weighing its risks, or a routine safety check skipped under time pressure. This module teaches the three disciplines that prevent that harm: a structured preoperative assessment that finds and optimises risk before the patient ever reaches the table; a working understanding of general, regional and local anaesthesia so you can take part intelligently in choosing and conducting the plan; and the principles of safe general surgery, anchored by the WHO Surgical Safety Checklist. These are everyday surgical competencies you will use on every operating list.
References
- Bailey & Love's Short Practice of Surgery, Preoperative Preparation and Anaesthesia (textbook)
- SRB's Manual of Surgery, Preoperative Preparation, Anaesthesia and Patient Safety (textbook)
- Sabiston Textbook of Surgery, Principles of Preoperative and Operative Surgery (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 62-year-old man is listed for an elective hernia repair. On the morning of surgery the team is busy; his chart is signed and he is wheeled in. Only after induction does someone notice he never stopped his clopidogrel, his blood sugar is uncontrolled, and the consent form names the wrong side. None of these is rare; none is unforeseeable; each could have been caught the day before by a few minutes of structured assessment, and the last by a ten-second time-out before the knife touched skin. Surgery is unforgiving of assumptions. The safest surgeons are not the fastest or the boldest — they are the ones who ask, every single time, the same disciplined questions before the operation begins, and who never skip the check that catches the rare catastrophe.
WHY THIS MATTERS
Preoperative assessment, anaesthetic choice and safe-surgery discipline are the framework that keeps elective and emergency surgery safe, and you will use all three on every patient you take to theatre. A good assessment finds the comorbidity that changes the plan, optimises the patient so the operation is survivable, sets realistic expectations and secures valid consent. Understanding the principles of general, regional and local anaesthesia lets you communicate sensibly with the anaesthetist, position and prepare the patient correctly, and recognise the complications that follow each technique. The WHO Surgical Safety Checklist — a one-page, low-cost intervention — measurably reduces deaths and complications by catching exactly the errors the hook describes. These are core, examinable surgical skills and a prerequisite to operating safely: no patient should be anaesthetised before they are properly assessed, and no incision made before the team has confirmed who, what and where.
RECALL
Recall the knowledge this skill builds on. From the airway-maintenance learning in this cluster, recall airway assessment — the Mallampati classification of the oropharyngeal view and the predictors of a difficult airway — because airway risk is central to anaesthetic planning. From pharmacology, recall that local anaesthetics act by blocking voltage-gated sodium channels in nerve membranes, and that they have ceiling doses above which systemic toxicity occurs. From the asepsis and safe-surgery learning, recall that surgical safety is a team behaviour, not an individual one. Finally, recall basic cardiorespiratory physiology — how anaesthesia and surgery stress the heart, lungs and circulation — since the whole purpose of preoperative assessment is to find the patient whose physiological reserve cannot absorb that stress, and to optimise them before, not during, the operation.
Why Preoperative Assessment and Anaesthetic Choice Decide Safety
The clinical indication for a structured preoperative assessment is every patient scheduled for surgery and anaesthesia, whether elective or emergency, because the assessment is the principal opportunity to identify, quantify and reduce perioperative risk before any harm is committed. Surgery and anaesthesia impose a coordinated physiological stress — on the airway and lungs, the heart and circulation, fluid and metabolic balance, and the patient's drugs and comorbidities — and the patient who tolerates that stress safely is, very often, simply the patient who was properly assessed and optimised beforehand. The assessment serves four linked purposes: it detects comorbidity and risk factors; it quantifies risk in a shared language (the ASA physical status grade); it optimises modifiable problems (controlling blood sugar, blood pressure or anaemia; managing antiplatelet and anticoagulant drugs; treating active infection) so the patient is in the best achievable state; and it prepares the patient through fasting, informed consent and a clear anaesthetic plan. Choosing the anaesthetic technique — general, regional or local — is part of this same risk calculus, matching the method to the patient and the operation. Layered on top of all of it is the discipline of safe general surgery: the systematic team checks, communication and verification, embodied in the WHO Surgical Safety Checklist, that catch the errors an individual will inevitably sometimes make. Assessment finds the hazard, the anaesthetic plan manages it, and the safety checklist guards against the slip — together they make a planned operation a safe one.
Principles and Framework of Preoperative Assessment
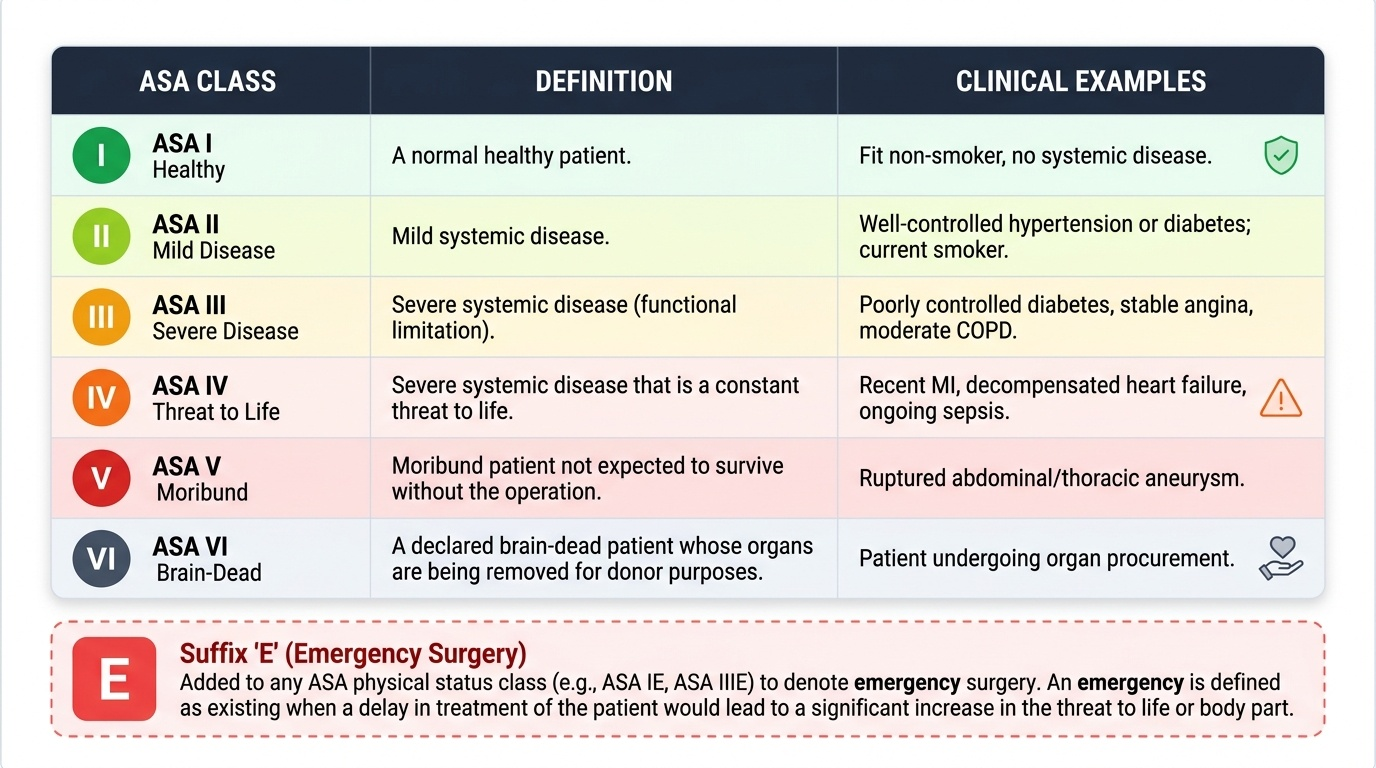
Preoperative assessment follows a disciplined framework so that nothing important is left to chance, and the same structure applies whether the patient is fit or frail. It begins with a focused history: the presenting surgical problem; significant comorbidities (cardiac, respiratory, renal, hepatic, diabetes, bleeding disorders); current medications — especially antiplatelet and anticoagulant drugs, antihypertensives, steroids, insulin and oral hypoglycaemics; allergies; previous anaesthetic history and any family history of anaesthetic problems; and functional capacity (how far the patient can walk or climb stairs, a practical marker of cardiorespiratory reserve). The examination covers the general state, the cardiovascular and respiratory systems, and a dedicated airway assessment (mouth opening, neck movement, Mallampati grade, dentition) to anticipate difficult intubation. From history and examination the team assigns an ASA physical status grade, a six-point scale that communicates the patient's burden of systemic disease in a single shared term. Investigations are targeted, not routine — ordered because the history, examination, age or proposed surgery makes them likely to change management (for example renal function before a contrast study, a coagulation screen in a patient on warfarin, an ECG in a patient with cardiac symptoms), rather than as a reflex panel for everyone. The framework then drives optimisation of modifiable risk, informed consent (explaining the procedure, its material risks, alternatives and the anaesthetic), and clear fasting instructions. Stating risk in the shared ASA language is what lets the surgeon and anaesthetist plan together.
Provided image
| ASA class | Definition | Example |
|---|---|---|
| I | A normal healthy patient | Fit non-smoker, no systemic disease |
| II | Mild systemic disease | Well-controlled hypertension or diabetes; current smoker |
| III | Severe systemic disease (functional limitation) | Poorly controlled diabetes, stable angina, moderate COPD |
| IV | Severe systemic disease that is a constant threat to life | Recent MI, decompensated heart failure, ongoing sepsis |
| V | Moribund patient not expected to survive without the operation | Ruptured aneurysm, massive trauma |
| VI | Brain-dead patient for organ donation | Declared brain-dead organ donor |
| E suffix | Added to any class for an emergency operation | Class III E = severe disease, emergency surgery |
SELF-CHECK
The ASA physical status classification is used preoperatively. What does it actually grade?
A. The technical difficulty of the planned operation
B. The patient's burden of systemic disease
C. The predicted difficulty of intubation
D. The expected duration of surgery
Reveal Answer
Answer: B. The patient's burden of systemic disease
ASA physical status (I healthy to VI brain-dead, with an E suffix for emergencies) grades the patient's BURDEN OF SYSTEMIC DISEASE, not operative difficulty, duration, or airway. Airway/intubation difficulty is graded separately by the Mallampati classification — do not conflate the two.
Conducting the Preoperative Assessment, Step by Step
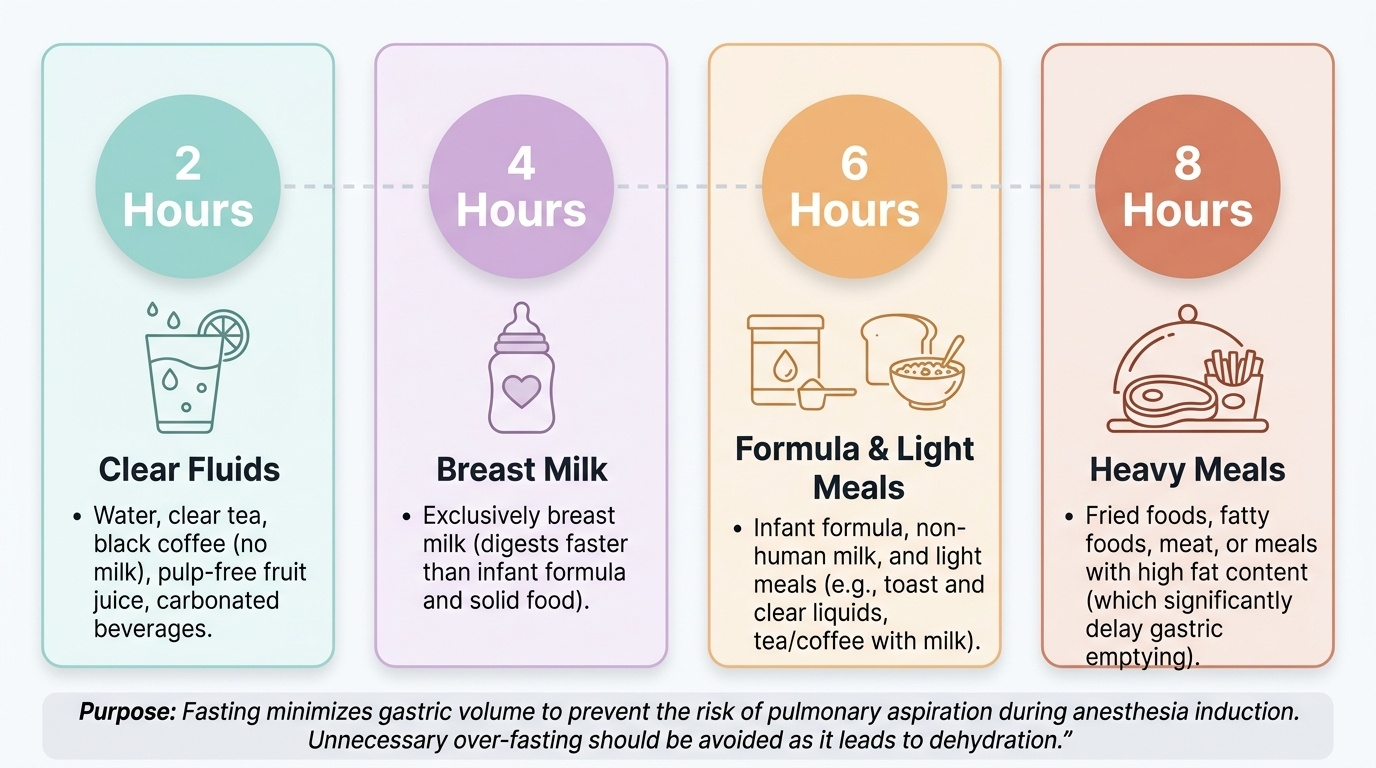
Performed in a consistent sequence, the assessment becomes reliable and quick. First, take the focused history as above, paying particular attention to the medication list and to drugs that must be managed around surgery — antiplatelets and anticoagulants (whether and when to stop or bridge), insulin and oral hypoglycaemics (sliding scales, omitted morning doses), steroids (perioperative cover), and antihypertensives. Second, examine the patient, including a deliberate airway assessment, and assign the ASA grade. Third, order only targeted investigations justified by the findings or the surgery. Fourth, optimise what is modifiable: control hyperglycaemia and hypertension, correct significant anaemia or electrolyte derangement, treat active infection, and arrange any specialist input the comorbidity demands — never operate electively on a patient who could safely be made better first. Fifth, take informed consent, documenting that the procedure, its material risks and benefits, the alternatives and the anaesthetic have been explained and understood. Sixth, give clear fasting instructions using the standard ASA "2-4-6-8" guidance, which balances aspiration risk against unnecessary dehydration: clear fluids until 2 hours before, breast milk 4 hours, infant formula or a light meal 6 hours, and a fatty or fried or meat-containing meal 8 hours before induction. The purpose of fasting is to minimise gastric volume and so the risk of pulmonary aspiration at induction; over-fasting a patient for an entire day is both unnecessary and harmful. The sequence ends with a documented, agreed anaesthetic and surgical plan.
Provided image
| Intake | Minimum fasting before induction |
|---|---|
| Clear fluids (water, clear juice, black tea/coffee) | 2 hours |
| Breast milk | 4 hours |
| Infant formula / non-human milk / light meal | 6 hours |
| Fatty or fried meal, or meat | 8 hours |