Page 2 of 15
SU11.{1-2,6} | Preoperative Assessment and Safe Anaesthesia Principles — SDL Guide (Part 2)
Principles of General, Regional and Local Anaesthesia
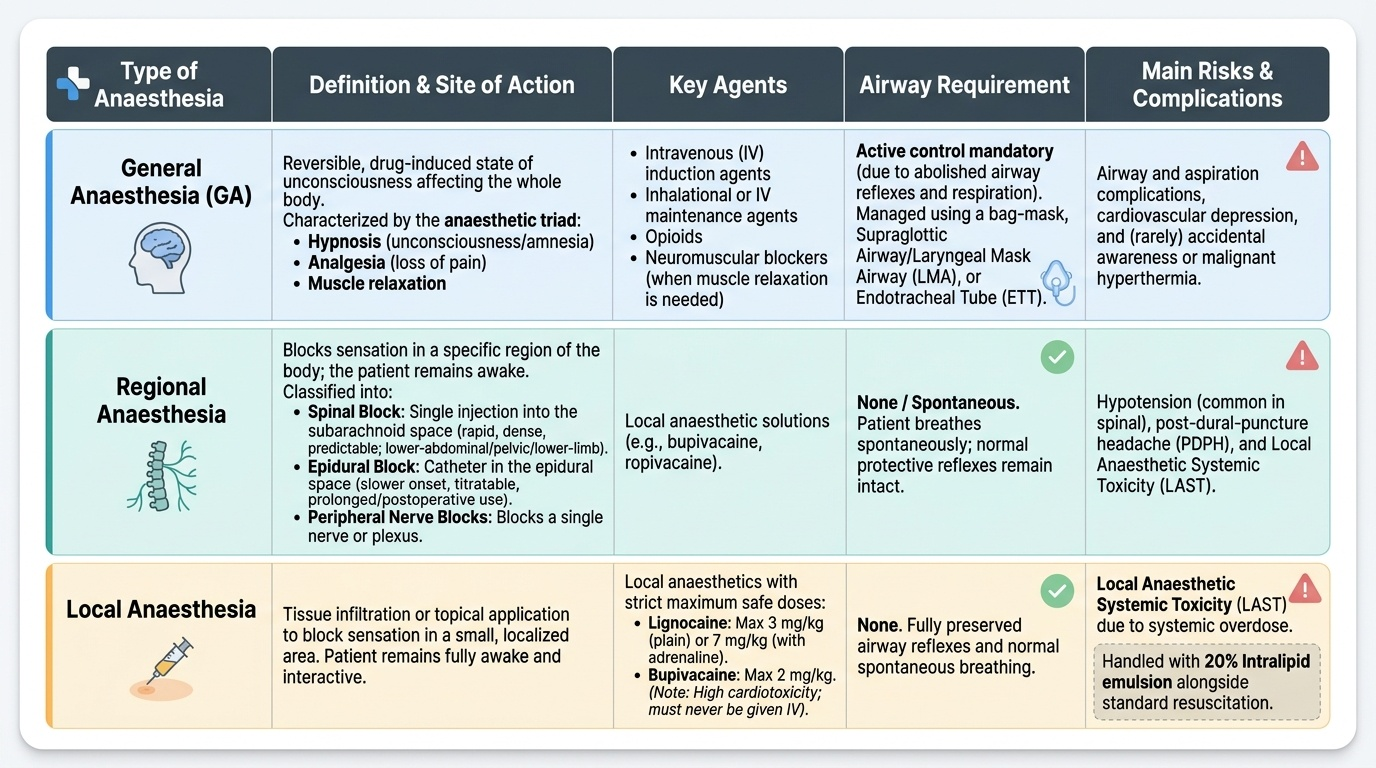
Anaesthesia is classified into three principal types, and understanding each lets you choose and conduct it safely. General anaesthesia (GA) is a reversible, drug-induced state of unconsciousness affecting the whole body, classically described by the anaesthetic triad of hypnosis (unconsciousness/amnesia), analgesia (loss of pain) and muscle relaxation, achieved with a combination of agents — intravenous induction agents, inhalational or intravenous maintenance, opioids and, when needed, neuromuscular blockers. Because GA abolishes airway reflexes and often respiration, it demands active airway control (bag-mask, supraglottic airway/LMA, or endotracheal intubation) and full monitoring; its risks include airway and aspiration complications, cardiovascular depression and, rarely, awareness or malignant hyperthermia. Regional anaesthesia blocks sensation in a region of the body while the patient may remain awake. Its central neuraxial forms are the spinal block (a single injection into the subarachnoid space, giving a rapid, dense, predictable block ideal for lower-abdominal, pelvic and lower-limb surgery, but carrying risks of hypotension and post-dural-puncture headache) and the epidural block (a catheter in the epidural space, slower in onset, titratable, and useful for prolonged surgery and postoperative analgesia); peripheral nerve blocks anaesthetise a single nerve or plexus. Local anaesthesia is the infiltration of tissue, or topical application, to anaesthetise a small area for minor procedures, with the patient fully awake. Local-anaesthetic drugs have maximum safe doses that must never be exceeded: lignocaine 3 mg/kg plain and 7 mg/kg with adrenaline, and bupivacaine 2 mg/kg (bupivacaine is the most cardiotoxic and must never be given intravenously); systemic overdose causes local-anaesthetic systemic toxicity (LAST), treated with 20% intralipid emulsion alongside resuscitation.
Provided image
| Type | Definition / site | Key agents | Airway | Main risks |
|---|---|---|---|---|
| General | Whole-body unconsciousness (triad: hypnosis + analgesia + relaxation) | IV induction + inhalational/IV maintenance ± opioid ± relaxant | Active control (mask/LMA/ETT) | Airway/aspiration, CVS depression, awareness, malignant hyperthermia |
| Regional (spinal) | Single subarachnoid injection; dense fast block | Bupivacaine ± opioid | Usually awake, airway intact | Hypotension, post-dural-puncture headache |
| Regional (epidural) | Catheter in epidural space; titratable, slower | Bupivacaine/levobupivacaine ± opioid | Usually awake | Hypotension, patchy block, dural puncture |
| Local | Infiltration/topical of a small area | Lignocaine, bupivacaine | Awake | LAST (toxicity if max dose exceeded) |
Interpreting Risk and Choosing the Anaesthetic Plan
The findings of the assessment are only useful when they are interpreted into a risk statement and a plan, and this is the step where assessment becomes decision. The interpretation runs along several axes. The ASA grade summarises systemic-disease burden and broadly tracks perioperative risk: an ASA I–II patient is usually straightforward, while ASA III–IV signals the need for optimisation, possibly higher-level postoperative care, and a careful weighing of whether and when to operate. The airway assessment (Mallampati grade, mouth opening, neck movement, dentition) is interpreted separately to predict a difficult intubation and to plan the airway strategy in advance — remembering that ASA and Mallampati measure entirely different things and must not be conflated. Functional capacity is read as a marker of cardiorespiratory reserve. The medication review is interpreted into concrete actions (stop, continue, bridge, or add perioperative cover). These threads then converge on the anaesthetic choice: a fit patient for a minor peripheral procedure may need only local anaesthesia; a lower-limb or lower-abdominal operation in a patient with significant respiratory disease may be safer under a spinal block that avoids general anaesthesia and airway instrumentation; a long, complex intra-abdominal operation will require general anaesthesia with controlled ventilation, perhaps combined with an epidural for postoperative analgesia. The plan must also account for urgency — an emergency (the ASA "E" suffix) compresses the time for optimisation and shifts the risk-benefit balance. Good interpretation produces a clear, defensible, patient-specific plan rather than a reflex default.
SELF-CHECK
A healthy adult is to have a 10 mm skin lesion excised under local infiltration. The team plans to use lignocaine. Which statement about the maximum safe dose is correct?
A. Lignocaine 7 mg/kg plain, 3 mg/kg with adrenaline
B. Lignocaine 3 mg/kg plain, 7 mg/kg with adrenaline
C. Lignocaine has no maximum dose for skin infiltration
D. Bupivacaine 7 mg/kg plain is the safer alternative
Reveal Answer
Answer: B. Lignocaine 3 mg/kg plain, 7 mg/kg with adrenaline
Lignocaine's maximum safe dose is 3 mg/kg plain and 7 mg/kg WITH adrenaline (adrenaline causes vasoconstriction, slowing systemic absorption and allowing a higher dose). Bupivacaine's maximum is 2 mg/kg and it is the most cardiotoxic local anaesthetic. Exceeding these doses causes LAST, treated with 20% intralipid.
Principles of Safe General Surgery and the WHO Checklist
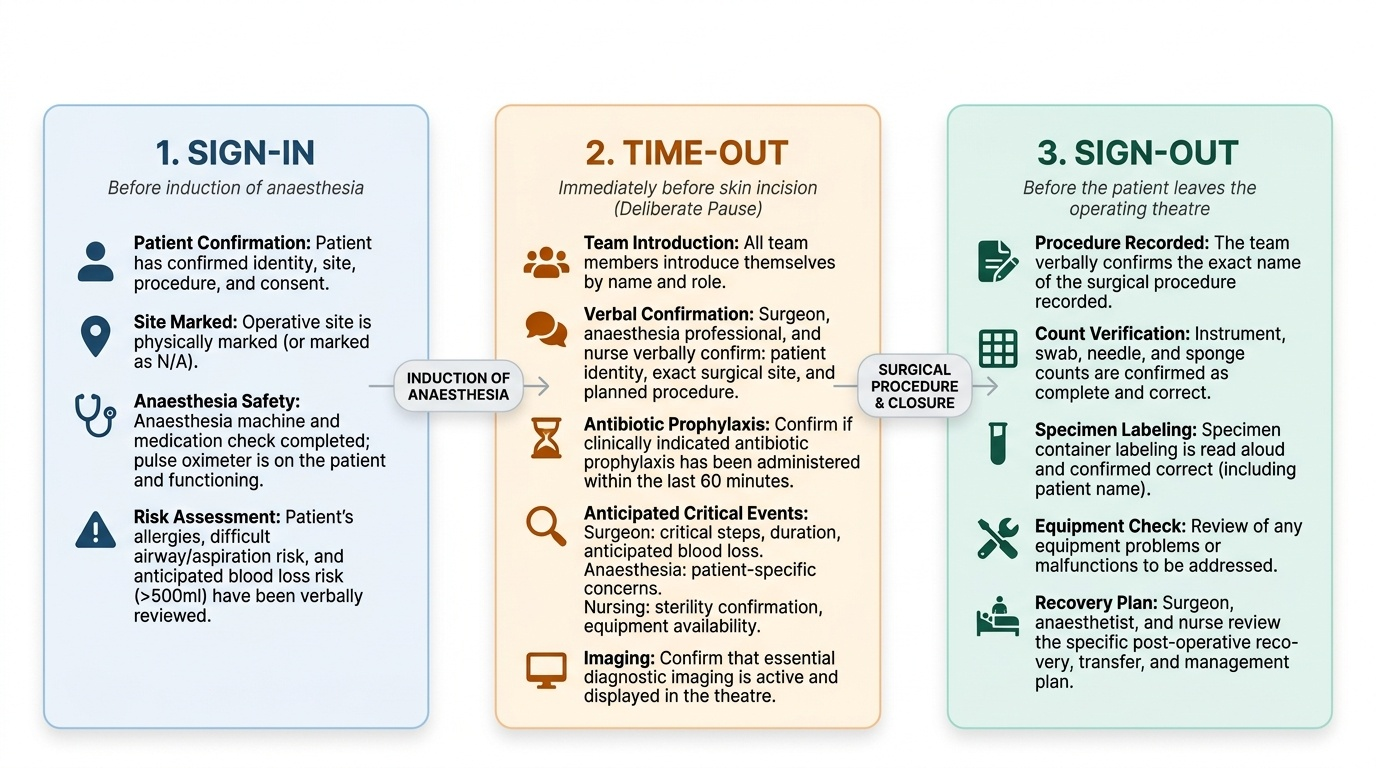
Even a well-assessed patient with a sound anaesthetic plan can be harmed by a preventable team error — the wrong patient, the wrong side, a forgotten antibiotic, an unanticipated airway, a retained swab. The principles of safe general surgery address these systematically: correct identification of the patient, procedure and site (with the operative site marked); shared situational awareness through structured team communication; anticipation of and preparation for foreseeable problems (blood loss, difficult airway, equipment needs); reliable infection prevention (timely prophylactic antibiotics, asepsis); and accurate instrument and swab counts to prevent retained items. These principles are operationalised by the WHO Surgical Safety Checklist, a brief, three-phase verbal checklist performed by the whole team. The sign-in, before induction of anaesthesia, confirms patient identity, site, procedure and consent, checks the anaesthesia machine and pulse oximeter, and reviews allergies and airway/aspiration risk. The time-out, immediately before skin incision, is a deliberate pause in which every team member is introduced, the patient-procedure-site is confirmed aloud, antibiotic prophylaxis and critical concerns are reviewed, and imaging is confirmed available. The sign-out, before the patient leaves theatre, confirms the procedure recorded, that instrument, swab and needle counts are correct, that specimens are labelled, and reviews any equipment problems and the recovery plan. Used reliably, the checklist catches exactly the errors that individual vigilance eventually misses, which is why it measurably reduces surgical mortality and complications.
Provided image
CLINICAL PEARL
ASA physical status and the Mallampati score answer different questions and must never be conflated: ASA grades the patient's systemic disease (how sick the patient is), while Mallampati grades the oropharyngeal view (how hard the airway may be). A fit ASA I patient can still have a Mallampati IV difficult airway, and a frail ASA IV patient can have an easy airway. Likewise, never quote a local-anaesthetic dose in millilitres alone — always work in mg/kg (lignocaine 3 mg/kg plain, 7 mg/kg with adrenaline; bupivacaine 2 mg/kg), because the safe volume depends on the concentration and the patient's weight.
Check Your Understanding
Consolidate the skill by walking the whole chain from the clinic to the closed wound. Start with the preoperative assessment: take a focused history (especially comorbidities and antiplatelet/anticoagulant, diabetic and steroid medications), examine the patient including a deliberate airway assessment, assign the ASA physical status grade, order only targeted investigations, optimise what is modifiable, take informed consent, and give clear 2-4-6-8 fasting instructions. Then interpret these findings — ASA grade for systemic risk, Mallampati and airway for intubation risk (a separate scale), functional capacity for reserve, the medication list for concrete perioperative actions — and translate them into an anaesthetic choice: general anaesthesia (the triad of hypnosis, analgesia and relaxation, with active airway control), regional anaesthesia (spinal in the subarachnoid space versus epidural in the epidural space), or local anaesthesia (respecting the maximum safe doses — lignocaine 3/7 mg/kg, bupivacaine 2 mg/kg — and ready to treat LAST with intralipid). Finally, deliver the operation under the discipline of safe general surgery, running the WHO Surgical Safety Checklist at sign-in, time-out and sign-out. Self-test on four links: can you list what a preoperative assessment covers and what ASA grades; can you state the 2-4-6-8 fasting rule and why fasting matters; can you define general, regional and local anaesthesia and the local-anaesthetic dose limits; and can you name the three phases of the WHO checklist and a key check in each? The questions in this module check exactly these.