Page 1 of 11
SU12.1 | Surgical Malnutrition — SDL Guide
Learning Objectives
- Define malnutrition and classify its types relevant to the surgical patient — undernutrition (marasmus, kwashiorkor, marasmic-kwashiorkor), sarcopenia, micronutrient deficiency and over-nutrition with deficiency (SU12.1).
- Enumerate the causes of malnutrition in the surgical patient grouped as reduced intake, impaired digestion and absorption, increased losses, and increased catabolic requirement (SU12.1).
- Enumerate the consequences of malnutrition system by system — impaired wound healing, immune dysfunction and sepsis, muscle and respiratory wasting, gut mucosal atrophy and translocation, organ dysfunction — and relate them to surgical outcomes (SU12.1).
- Describe how malnutrition is recognised and assessed using clinical evaluation, anthropometry, the Subjective Global Assessment, validated screening tools and biochemical markers, including their limitations (SU12.1).
INSTRUCTIONS
Malnutrition is the commonest, most under-recognised and most readily modifiable risk factor on a surgical ward. As many as a third to a half of hospitalised surgical patients are malnourished on admission, and most become more so during their stay — yet it is rarely measured and frequently ignored. A malnourished patient heals badly, leaks anastomoses, succumbs to infection, breathes poorly off the ventilator and stays in hospital far longer than a well-nourished one. This module builds the foundation for everything that follows on nutritional support: it teaches you to define malnutrition, to understand why surgical patients in particular slide into it, to recognise the damage it does, and to detect it at the bedside before it costs your patient an outcome.
References
- Bailey & Love's Short Practice of Surgery, Nutrition and Fluid Therapy chapter (textbook)
- SRB's Manual of Surgery, Nutrition in Surgical Patients (textbook)
- Sabiston Textbook of Surgery, Surgical Metabolism and Nutrition (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old man has lost 12 kilograms over four months. He puts it down to a poor appetite, but the real cause is a slowly obstructing carcinoma of the stomach. By the time he reaches the operating list he looks gaunt, his trousers hang loose, and his grip is weak — yet his blood tests are 'normal' and nobody has weighed him. Five days after an otherwise technically perfect gastrectomy his wound gapes, his chest is full of secretions he is too weak to cough up, and the anastomosis begins to leak. None of this is bad luck. It is the entirely predictable consequence of an unrecognised, untreated state that was present long before he came to theatre: malnutrition. Spot it early and you change the whole trajectory; ignore it and the best operation in the world can still fail.
WHY THIS MATTERS
Nutrition sits beneath almost every surgical outcome, which is exactly why it is examined as foundational science and applied every day on the ward. A malnourished patient is the one who leaks an anastomosis, dehisces a wound, develops a surgical-site infection, fails to wean from the ventilator because the diaphragm has wasted, and occupies a bed for twice as long at twice the cost. Crucially, unlike the patient's age or the stage of their cancer, malnutrition is modifiable — it can be screened for in minutes, quantified, and corrected before and after surgery. The whole point of learning to define, cause-map, and assess malnutrition is so that you can intervene. Get this foundation right and your later decisions about who to feed, by what route, and how much become reasoned rather than reflexive. Get it wrong — by trusting a 'normal' albumin or by never weighing the patient — and you will keep being surprised by complications that were avoidable.
RECALL
Before going further, recall three things you already know. First, from the metabolic response to injury (SU1): major surgery, trauma and sepsis trigger a catabolic flow phase in which counter-regulatory hormones (cortisol, catecholamines, glucagon) drive proteolysis, lipolysis and a negative nitrogen balance — the body breaks down its own muscle for fuel and repair. Second, basic nutritional physiology: the body's fuel reserves are glycogen (small, exhausted within a day of starvation), fat (large, the main long-term store) and protein (structural, not a true 'store' — using it means consuming functioning tissue). Third, normal protein turnover and the role of albumin and other plasma proteins synthesised by the liver. Keep these in mind: surgical malnutrition is essentially what happens when reduced intake collides with the increased demands of the catabolic surgical state, forcing the body to cannibalise its own protein.
Why Malnutrition Matters on the Surgical Ward
Malnutrition is any state of nutrition in which a deficiency, excess or imbalance of energy, protein and other nutrients causes measurable adverse effects on body composition, function and clinical outcome. In surgical practice the word almost always means undernutrition — a deficit of energy and protein — although the modern obese patient with hidden micronutrient and lean-mass deficiency reminds us that a high body weight does not exclude malnutrition. It is, by some distance, the single most important modifiable risk factor a surgical patient carries: large hospital surveys consistently find that roughly a third to a half of surgical inpatients are malnourished on admission, the proportion is highest in those with gastrointestinal cancer, sepsis and chronic disease, and nutritional status typically deteriorates further during the admission as patients are kept nil-by-mouth, undergo repeated investigations, and mount a catabolic response to their illness and operations. What makes this matter so much to the surgeon is the combination of three features: malnutrition is common, it is damaging to every surgical outcome that we care about, and — unlike age, comorbidity or cancer stage — it is modifiable. A patient identified as malnourished before an elective operation can be optimised; one identified after a major resection can be supported through the catabolic period. The cost of missing it is paid in dehisced wounds, leaked anastomoses, infections, prolonged ventilation, longer stays and excess deaths. The whole purpose of this module is to make malnutrition visible — to define it, understand its surgical causes, recognise its consequences, and assess it reliably at the bedside — so that it can be treated rather than discovered too late at the post-mortem of a complication.
What Is Malnutrition? Definitions and Types
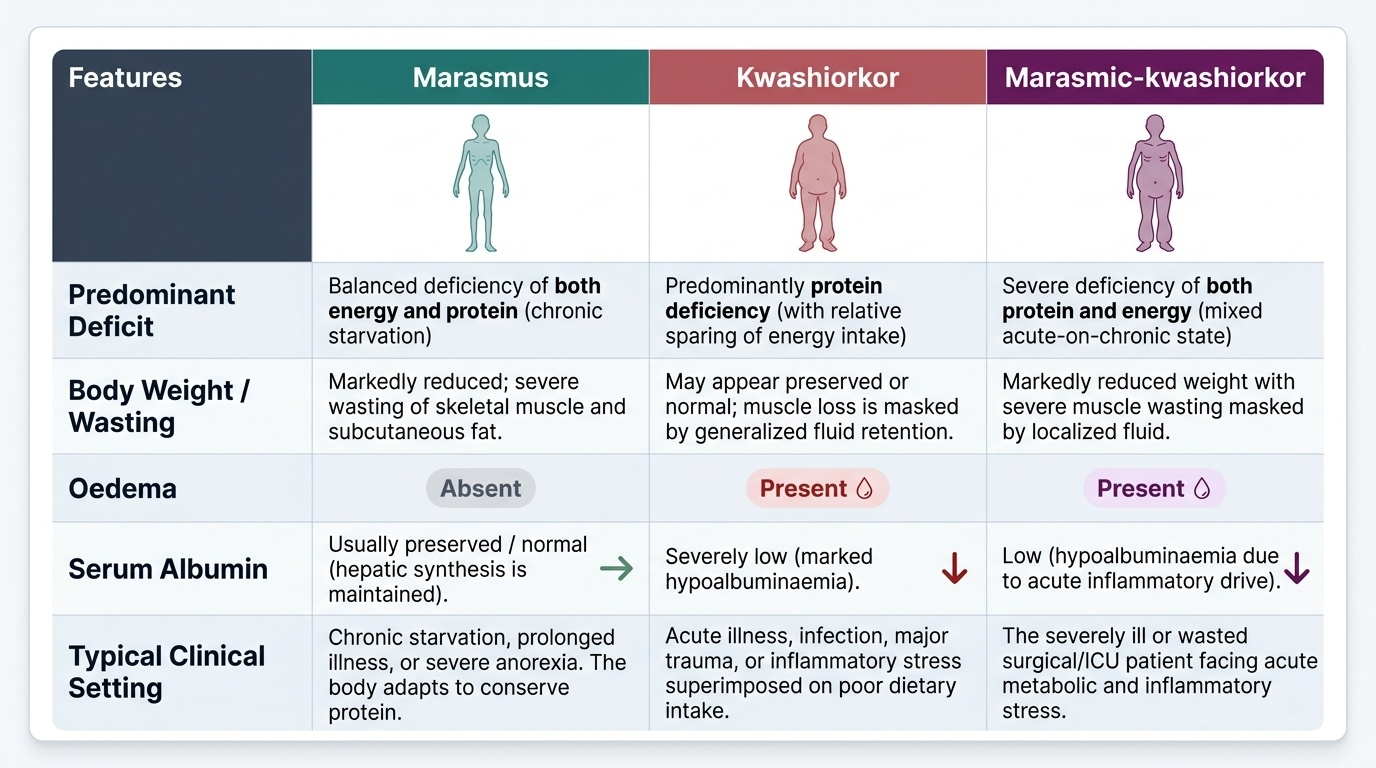
Malnutrition is not a single entity, and recognising its forms helps you anticipate the pattern of harm. The dominant surgical concern is protein-energy malnutrition (PEM), classically described in two extremes with a mixed middle. Marasmus is chronic, balanced deficiency of both energy and protein: the body adapts by consuming its own fat and muscle, producing the wasted, 'skin-and-bones' patient with profound loss of subcutaneous fat and skeletal muscle but, characteristically, a preserved (normal) serum albumin because hepatic synthesis is maintained and there is no major inflammatory drive. Kwashiorkor is predominantly protein deficiency, often precipitated by acute stress or inflammation on a background of poor intake; it is marked by hypoalbuminaemia, oedema (and in children a fatty liver), so the patient may look deceptively well-covered or even swollen despite being severely depleted. Marasmic-kwashiorkor is the common mixed picture in sick surgical patients — established wasting plus a superimposed hypoalbuminaemic, oedematous, inflammatory state. Beyond PEM, you must also recognise sarcopenia (the disease- or age-related loss of skeletal muscle mass and function, increasingly identified on CT as a powerful predictor of poor surgical outcome), micronutrient (vitamin and trace-element) deficiencies such as vitamin C and zinc (impairing wound healing), vitamin K (coagulopathy) and thiamine, and over-nutrition — obesity — which carries its own surgical risks and can coexist with lean-tissue and micronutrient deficiency ('sarcopenic obesity'). Holding this map in mind lets you predict whether a given patient is wasted, oedematous, immunosuppressed or all three.
Provided image
| Feature | Marasmus | Kwashiorkor | Marasmic-kwashiorkor |
|---|---|---|---|
| Predominant deficit | Energy + protein (balanced) | Protein (relative energy spared) | Both, severe |
| Body weight / wasting | Markedly reduced, severe wasting | May appear preserved (oedema masks loss) | Severe wasting + oedema |
| Oedema | Absent | Present (hypoalbuminaemic) | Present |
| Serum albumin | Usually preserved | Low (hypoalbuminaemia) | Low |
| Typical setting | Chronic starvation, slow obstruction | Protein-poor intake + acute stress/inflammation | Sick, stressed surgical patient |
SELF-CHECK
A cachectic patient with a slowly obstructing oesophageal cancer has obvious muscle and fat wasting but a normal serum albumin. Which pattern of protein-energy malnutrition does this best fit?
A. Marasmus
B. Kwashiorkor
C. Refeeding syndrome
D. Sarcopenic obesity
Reveal Answer
Answer: A. Marasmus
Chronic balanced energy-and-protein deficiency producing severe wasting WITH a preserved albumin is marasmus. Kwashiorkor is characterised by hypoalbuminaemia and oedema; refeeding syndrome is a metabolic complication of re-feeding, not a baseline pattern; sarcopenic obesity implies a high body weight.
Why Surgical Patients Become Malnourished — The Causes
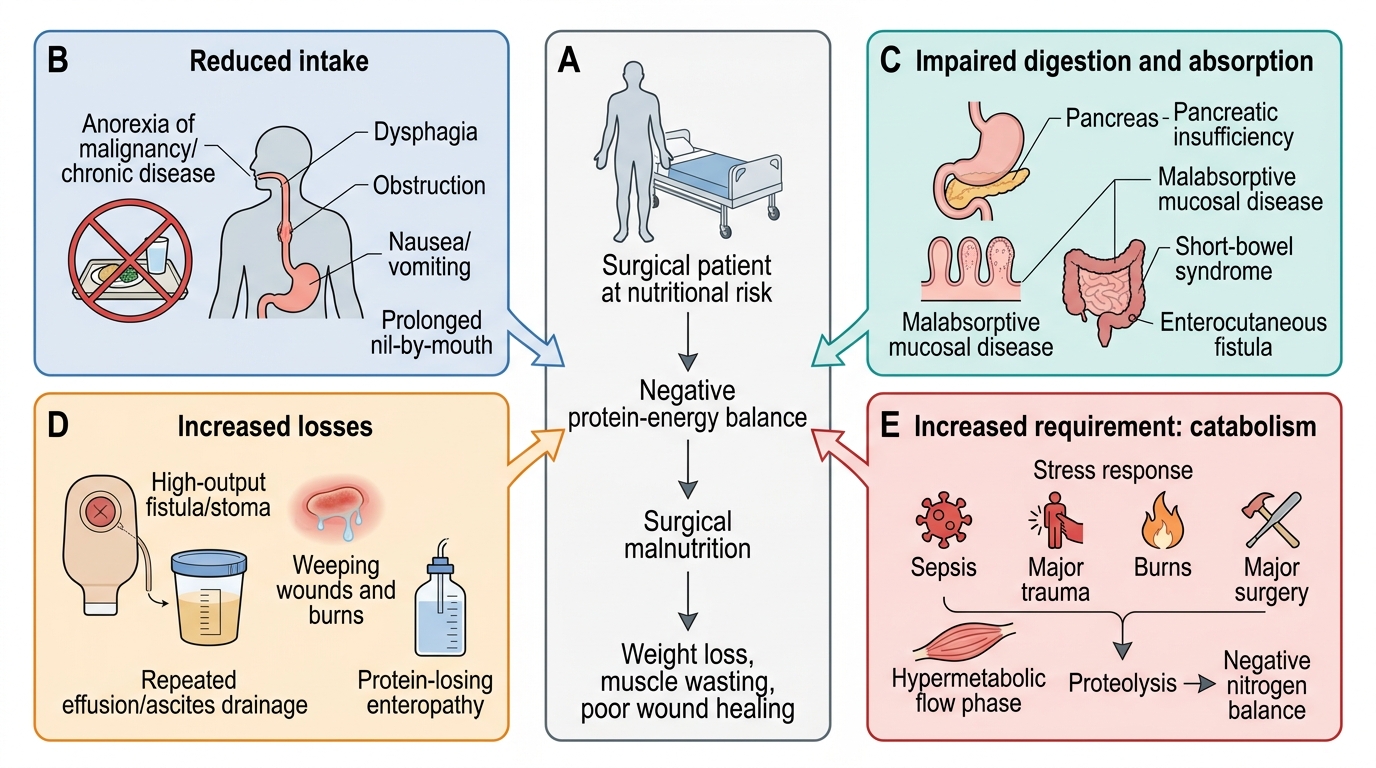
The causes of malnutrition in the surgical patient are best enumerated as four mechanistic groups, because each points to a different remedy. The first is reduced intake: anorexia of malignancy and chronic disease, painful or obstructing lesions of the mouth, oesophagus and gut (dysphagia, gastric outlet or intestinal obstruction), nausea and vomiting, the depression and unfamiliar food of hospital, and — very importantly and iatrogenically — prolonged nil-by-mouth orders for investigations and repeated procedures. The second is impaired digestion and absorption (maldigestion and malabsorption): pancreatic insufficiency, biliary obstruction, mucosal disease such as coeliac or Crohn's, extensive bowel resection producing short-bowel syndrome, and enterocutaneous fistulae that both bypass absorptive surface and drain nutrient-rich fluid. The third is increased losses: protein and fluid lost through fistulae, stomas with high output, large weeping wounds and burns, repeated drainage of effusions or ascites, and protein-losing enteropathy. The fourth, and the one that makes the surgical patient special, is increased requirement from the catabolic, hypermetabolic state — the flow phase of the metabolic response to injury, sepsis, major burns and major surgery, in which counter-regulatory hormones and inflammatory cytokines drive proteolysis and raise energy expenditure so that even a previously well-nourished patient runs a steep negative nitrogen balance. In real patients these mechanisms overlap: the man with a gastric cancer eats little (reduced intake), may malabsorb, loses protein from his tumour and surgery, and is profoundly catabolic afterwards — four hits at once. Mapping a patient onto these four groups tells you both why they are malnourished and where to intervene.
Mechanisms of Surgical Malnutrition
- Reduced intake: anorexia of malignancy/chronic disease, dysphagia, obstruction, nausea/vomiting, prolonged nil-by-mouth.
- Impaired digestion/absorption: pancreatic insufficiency, malabsorptive mucosal disease, short-bowel syndrome, enterocutaneous fistula.
- Increased losses: high-output fistula/stoma, weeping wounds and burns, repeated effusion/ascites drainage, protein-losing enteropathy.
- Increased requirement (catabolism): sepsis, major trauma, burns and major surgery — the hypermetabolic flow phase driving proteolysis and negative nitrogen balance.