Page 2 of 11
SU12.1 | Surgical Malnutrition — SDL Guide (Part 2)
The Consequences of Malnutrition in the Surgical Patient
The consequences of malnutrition are best learned system by system, because each maps directly onto a surgical complication you will be asked to prevent. Wound healing is impaired: protein, calories, vitamin C and zinc are all needed for collagen synthesis and cross-linking, so the malnourished patient suffers delayed healing, weak wounds, dehiscence and anastomotic breakdown. Immune function is depressed: cell-mediated immunity, neutrophil function and antibody production all fall, producing anergy and a markedly increased risk of surgical-site, chest and line sepsis — and infection in turn deepens catabolism, a vicious cycle. Skeletal muscle wastes, including the respiratory muscles and diaphragm, so the patient ventilates poorly, cannot cough or clear secretions, develops atelectasis and pneumonia, and is difficult to wean from the ventilator; loss of general muscle bulk also delays mobilisation and rehabilitation. The gut mucosa atrophies when it is unused (a key argument for enteral feeding), weakening the mucosal barrier and permitting bacterial translocation that can seed systemic sepsis. Organ function declines — cardiac muscle weakens, hepatic synthetic and metabolic function falters, and thermoregulation and wound contraction suffer. There are psychological effects too: apathy, depression and loss of the will to recover. The net result, demonstrated repeatedly in surgical series and codified in guidelines such as those of ESPEN and ASPEN, is increased post-operative morbidity (especially infective and wound complications and anastomotic leak), increased mortality, prolonged length of stay, more ICU and ventilator days, and higher cost. Every one of these endpoints improves when malnutrition is recognised and corrected — which is precisely why the assessment that follows matters.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
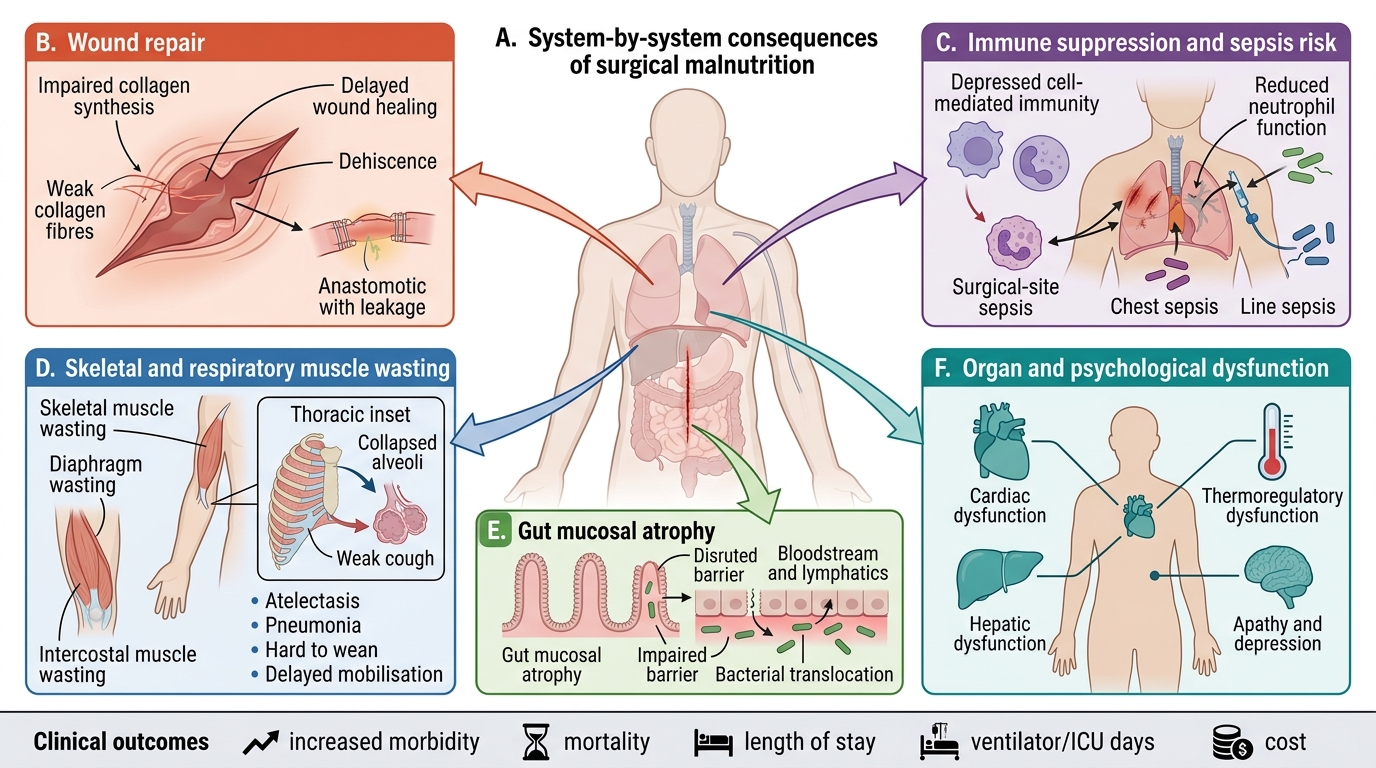
Consequences of Malnutrition in Surgical Patients
- Wound/repair: impaired collagen synthesis → delayed healing, dehiscence, anastomotic leak.
- Immune: depressed cell-mediated immunity and neutrophil function → surgical-site, chest and line sepsis.
- Muscle (incl. respiratory): wasting of diaphragm/intercostals → poor cough, atelectasis, pneumonia, hard to wean; delayed mobilisation.
- Gut: mucosal atrophy with disuse → impaired barrier and bacterial translocation.
- Organs/psyche: cardiac, hepatic and thermoregulatory dysfunction; apathy and depression.
- Outcomes: ↑ morbidity, ↑ mortality, ↑ length of stay, ↑ ventilator/ICU days, ↑ cost.
Recognising and Assessing the Malnourished Patient
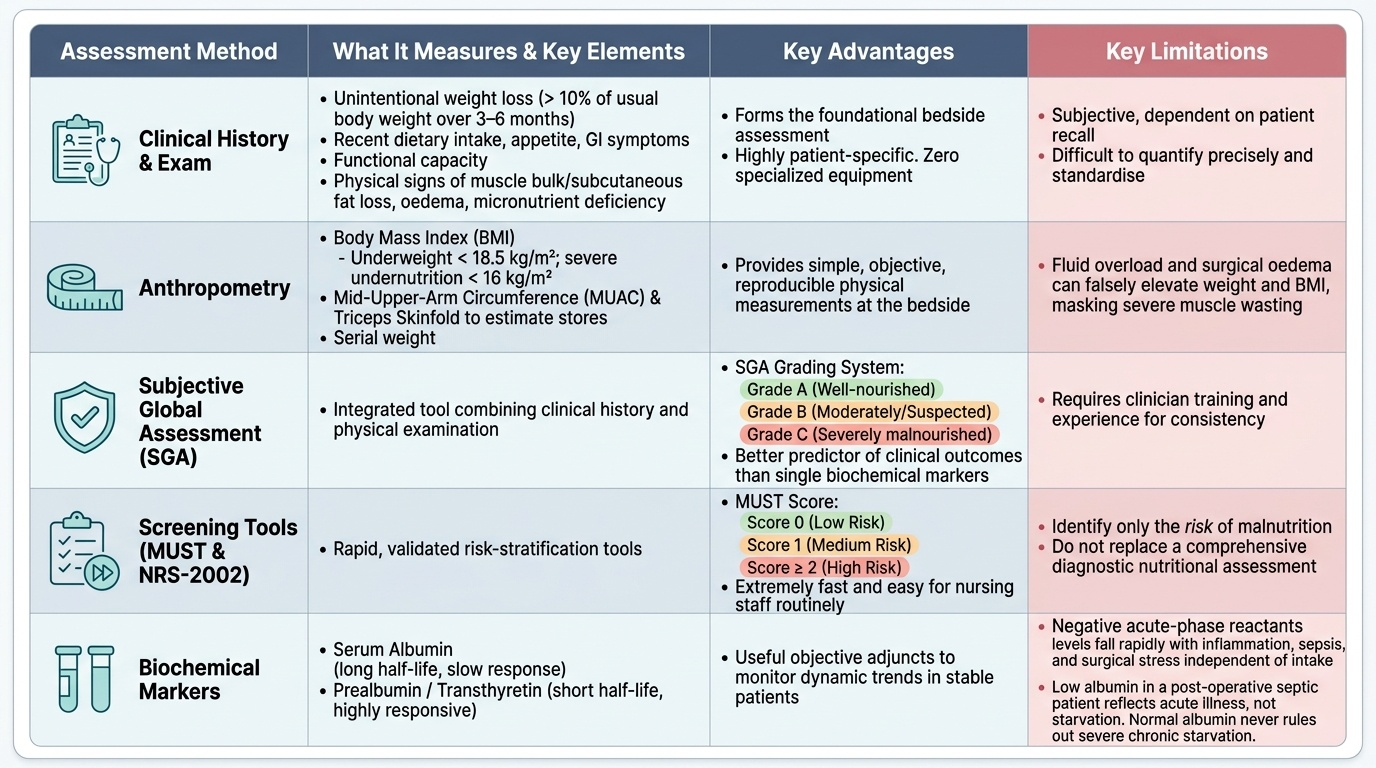
Because malnutrition is silent and routinely missed, structured assessment is essential, and it begins not with a blood test but with the history and clinical examination. Ask about and document unintentional weight loss — a loss of more than 10% of usual body weight over three to six months is clinically significant — recent dietary intake, appetite, gastrointestinal symptoms and functional capacity (grip strength, ability to climb stairs). On examination look for loss of subcutaneous fat and muscle bulk (temples, deltoids, interossei, quadriceps), oedema, loose skin, and signs of micronutrient deficiency. Anthropometry quantifies this: body mass index (BMI <18.5 kg/m² is underweight, <16 indicates severe undernutrition), mid-upper-arm circumference (MUAC) and triceps skinfold thickness for fat and muscle stores, and serial weight (the simplest and most important measurement, which must actually be performed). The best-validated bedside tool is the Subjective Global Assessment (SGA), which integrates history (weight change, intake, symptoms, functional capacity) and examination (fat/muscle loss, oedema) into a single grade — A well-nourished, B moderately or suspected malnourished, C severely malnourished — and predicts outcome better than any single biochemical marker. Validated screening tools for routine use on admission include the Malnutrition Universal Screening Tool (MUST) (scored 0 low / 1 medium / ≥2 high risk) and NRS-2002. Biochemical markers are useful adjuncts but must be interpreted with care: serum albumin (half-life ~20 days) and prealbumin/transthyretin (half-life ~2 days, more responsive) are negative acute-phase reactants — they fall with inflammation and surgical stress independently of nutrition, so a low albumin in a septic post-operative patient reflects illness more than starvation and a normal albumin never excludes malnutrition (recall the marasmic patient with a normal albumin). Used together — history, anthropometry, a structured tool such as SGA, and cautiously interpreted biochemistry — these methods identify the at-risk patient reliably and in minutes.
Provided image
| Method | What it captures | Key limitation |
|---|---|---|
| History & examination | Weight loss %, intake, symptoms, fat/muscle loss, oedema | Subjective; requires the patient be weighed and examined |
| Anthropometry (BMI, MUAC, skinfold, serial weight) | Body stores and trend | Oedema/fluid shifts distort weight and BMI |
| Subjective Global Assessment (SGA, A–C) | Integrated global grade, predicts outcome | Operator training needed; still partly subjective |
| Screening tools (MUST 0/1/≥2; NRS-2002) | Risk stratification at admission | Screen, not a full assessment |
| Biochemistry (albumin t½ ~20 d; prealbumin t½ ~2 d) | Adjunct trend marker | Negative acute-phase reactants — fall with inflammation, not specific to nutrition |
CLINICAL PEARL
Never trust a 'normal' albumin to exclude malnutrition, and never read a low albumin as proof of starvation. Albumin is a negative acute-phase reactant with a ~20-day half-life: it falls with inflammation, sepsis and surgical stress regardless of nutritional intake, and it is preserved in the wasted marasmic patient who is unmistakably malnourished. The two most valuable nutritional 'tests' are free and at the bedside: a documented percentage of unintentional weight loss and a structured Subjective Global Assessment. Weigh the patient.
SELF-CHECK
Which statement about nutritional assessment in the surgical patient is correct?
A. A normal serum albumin reliably excludes malnutrition
B. Unintentional loss of more than 10% of body weight over 3–6 months is clinically significant
C. Albumin rises during the acute inflammatory response
D. Biochemical markers are more reliable than the Subjective Global Assessment for predicting surgical outcome
Reveal Answer
Answer: B. Unintentional loss of more than 10% of body weight over 3–6 months is clinically significant
Unintentional weight loss >10% over 3–6 months is a recognised marker of significant malnutrition. Albumin is a negative acute-phase reactant — it FALLS with inflammation and a normal value does NOT exclude malnutrition (a marasmic patient may have normal albumin). The SGA predicts outcome better than any single biochemical marker.
Check Your Understanding
Before moving on, consolidate by reasoning through an integrated case rather than recalling isolated facts. Return to the man with the obstructing gastric cancer who lost twelve kilograms. First, classify him: chronic, largely balanced energy-and-protein deprivation with severe wasting but, before sepsis supervened, a preserved albumin — a marasmic picture sliding toward marasmic-kwashiorkor once the inflammatory stress of obstruction and surgery is added. Second, enumerate his causes across the four groups: reduced intake (the obstructing tumour and anorexia), possible malabsorption, increased losses (the tumour and the operation), and a steeply increased catabolic requirement after major surgery — several hits at once. Third, predict his consequences system by system and match them to what actually happened: impaired wound healing (the gaping wound), depressed immunity (sepsis), respiratory-muscle wasting (the retained secretions he was too weak to cough up) and impaired anastomotic healing (the leak). Fourth, say how he should have been assessed: he should have been weighed and his >10% weight loss documented, an SGA performed grading him category C, a MUST score recorded as high risk, and his 'normal' albumin recognised as no reassurance at all. Test yourself on three links: can you place a patient's malnutrition into a type; can you sort their causes into the four mechanistic groups; and can you justify which assessment you would use and why a normal albumin does not let you off the hook? The questions below check exactly these connections.