Page 1 of 10
MI6.1-3 | CNS Infections — Meningitis & Encephalitis — SDL Guide
Learning Objectives
- Enumerate the microbial agents causing bacterial, viral, fungal, and parasitic meningitis
- Explain the pathogenesis and clinical course of meningitis caused by each major agent
- Describe the laboratory diagnosis of meningitis including CSF analysis, Gram stain, culture, and ancillary tests
- Enumerate the microbial agents causing encephalitis and describe their pathogenesis and laboratory diagnosis
- Read and interpret CSF Gram stain and culture reports to diagnose CNS infection by aetiology and guide management
INSTRUCTIONS
CNS infections are neurological emergencies — meningitis and encephalitis can kill or cause permanent disability within hours of onset. The ability to interpret a CSF result rapidly and accurately is a life-saving clinical skill. This module integrates microbiology with clinical reasoning: you will learn the organisms, their pathogenesis, and the CSF findings that distinguish each, so you can act correctly in the emergency room.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, 11th ed., Ch 24, 35, 44, 49 (textbook)
- Harrison's Principles of Internal Medicine, 21st ed., Ch 140-142 (textbook)
- Mandell, Douglas & Bennett's Principles of Infectious Diseases, 9th ed., Ch 89 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 19-year-old engineering student is brought to the emergency room with a 6-hour history of severe headache, high fever, neck stiffness, and non-blanching petechial rash on his trunk. His GCS is 13/15. His classmate died of the same illness 3 days ago. Within 30 minutes of your clinical assessment, you perform a lumbar puncture. The CSF is turbid; you see Gram-negative diplococci in pairs on the emergency Gram stain. You know immediately: Neisseria meningitidis, purulent meningitis. You start ceftriaxone before the culture result. He survives; your rapid interpretation made the difference.
WHY THIS MATTERS
India carries one of the world's highest burdens of CNS infections — including tuberculous meningitis, Japanese encephalitis, and viral meningitis from enteroviruses. Bacterial meningitis carries a 20-30% mortality even with treatment, rising to >50% if treatment is delayed beyond 6 hours of symptom onset. Identifying the aetiology from CSF within the first hour of presentation is the single most important determinant of outcome. Encephalitis, while rarer, is often harder to diagnose and increasingly important in India following Japanese encephalitis vaccination campaigns.
RECALL
From Anatomy, recall the meninges: dura mater (outermost), arachnoid (middle), pia mater (innermost). Cerebrospinal fluid (CSF) circulates in the subarachnoid space between arachnoid and pia. From Physiology, recall the blood-brain barrier (BBB) — formed by tight junctions between cerebral capillary endothelial cells; lipid-soluble drugs cross readily, most antibiotics and pathogens do not. Bacterial meningitis involves inflammation of the meninges; encephalitis involves inflammation of the brain parenchyma itself.
Pathogenesis of Bacterial Meningitis
Pathogenesis of Bacterial Meningitis
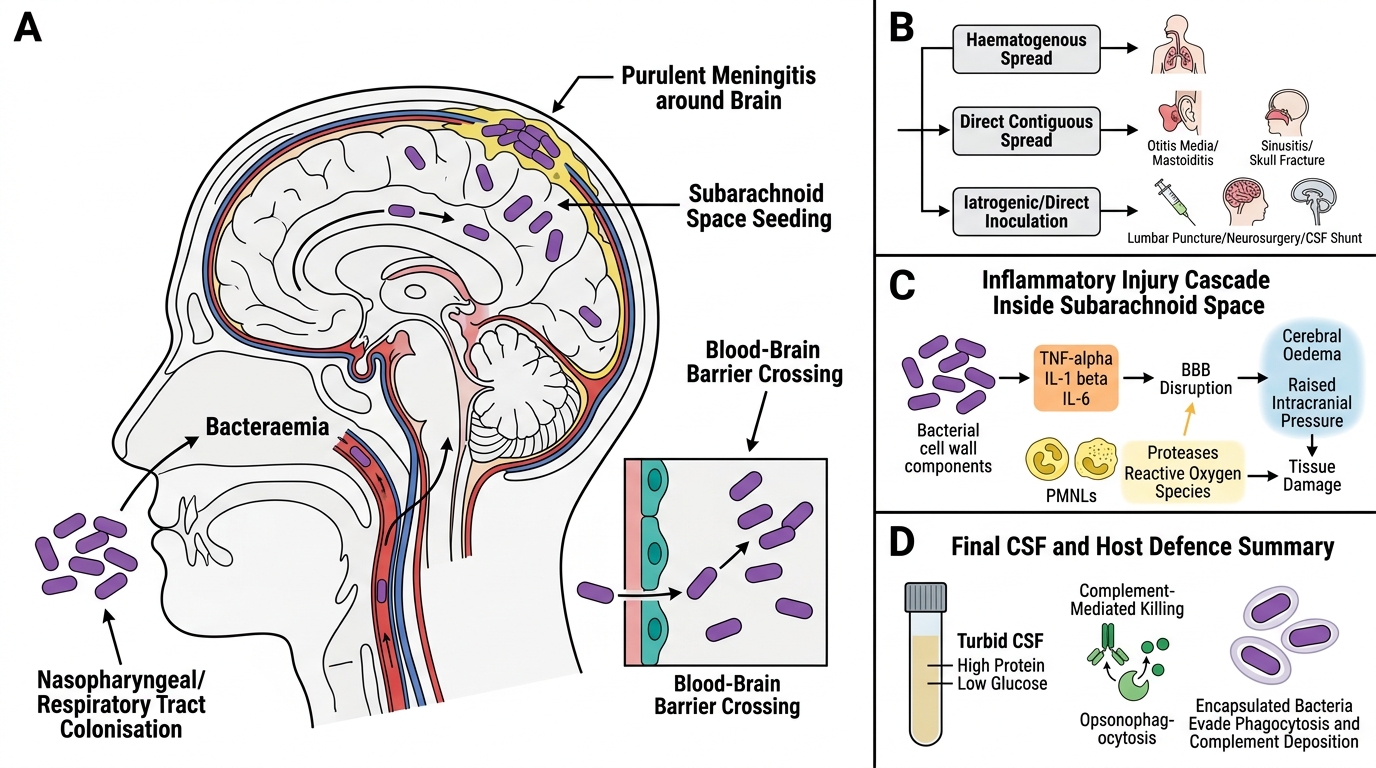
Bacterial meningitis follows one of three routes of CNS invasion:
- Haematogenous spread (most common) — bacteraemia from respiratory tract colonisation → bacteria cross the BBB via transcytosis or paracellular invasion of endothelial cells → subarachnoid space seeding.
- Direct spread — from contiguous infection: otitis media → mastoiditis → meningitis; sinusitis → frontal lobe abscess; skull fracture → meningitis.
- Iatrogenic/direct inoculation — lumbar puncture, neurosurgery, CSF shunts → Staphylococcus epidermidis, S. aureus.
Mechanism of CNS damage in bacterial meningitis:
Bacterial cell wall components (LPS in Gram-negative; peptidoglycan + teichoic acid in Gram-positive) trigger cytokine release (TNF-α, IL-1β, IL-6) → BBB disruption → cerebral oedema → raised intracranial pressure.
Simultaneously, PMNLs flood the subarachnoid space → release proteases and reactive oxygen species → further tissue damage. The net result: turbid CSF, high protein (from BBB breakdown), low glucose (consumed by bacteria and PMNLs).
Complement-mediated killing and opsonophagocytosis are the primary host defences. Encapsulated organisms (Neisseria meningitidis, Streptococcus pneumoniae, Haemophilus influenzae) evade both — their capsule resists phagocytosis and complement deposition.
Causes of Meningitis by Age Group and Category
Causes of Meningitis by Age and Risk Category
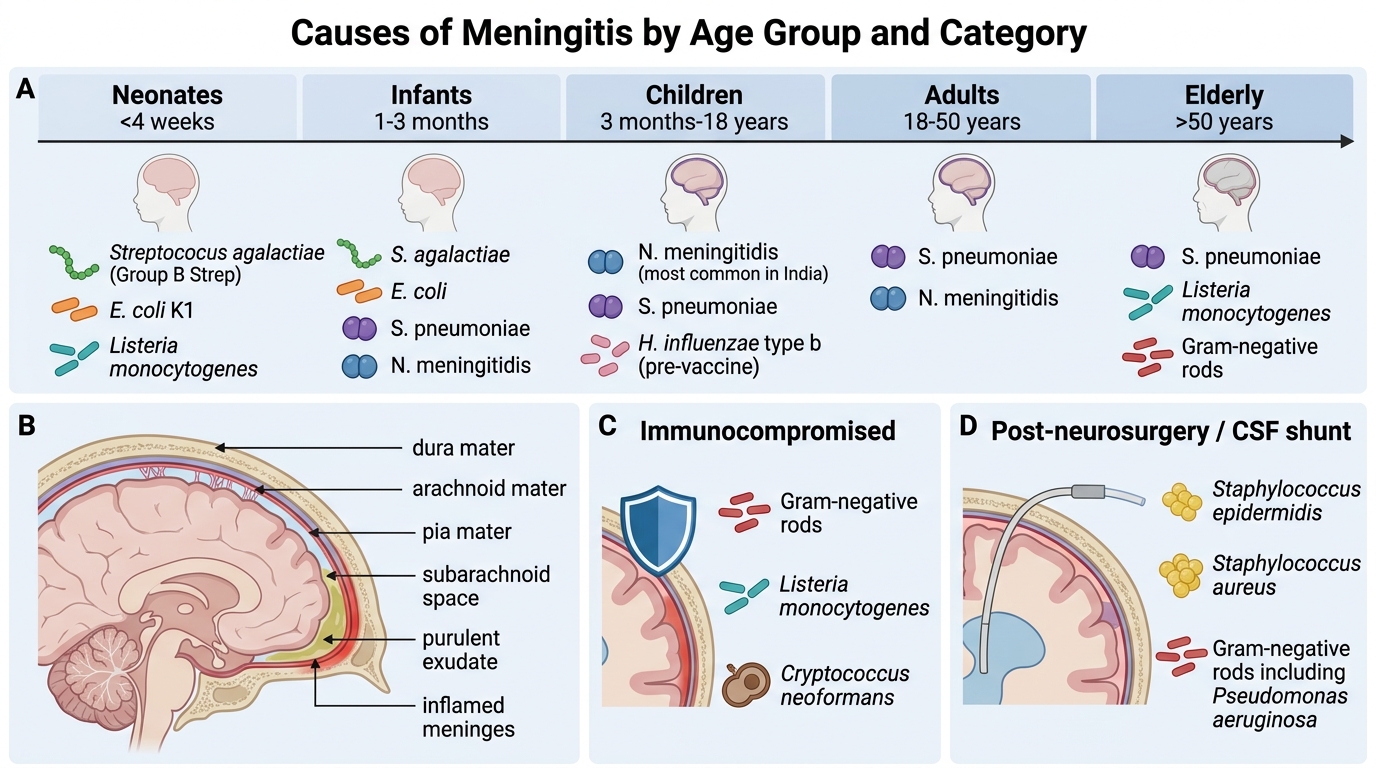
Bacterial Meningitis — organisms by age group
| Age group | Common organisms |
|---|---|
| Neonates (<4 weeks) | Streptococcus agalactiae (Group B Strep), E. coli (K1 capsule), Listeria monocytogenes |
| Infants (1-3 months) | S. agalactiae, E. coli, S. pneumoniae, N. meningitidis |
| Children (3 months - 18 years) | N. meningitidis (most common in India), S. pneumoniae, H. influenzae type b (pre-vaccine) |
| Adults (18-50 years) | S. pneumoniae, N. meningitidis |
| Elderly (>50 years) | S. pneumoniae, Listeria monocytogenes, Gram-negative rods |
| Immunocompromised | Gram-negative rods, Listeria, Cryptococcus neoformans |
| Post-neurosurgery/shunt | S. epidermidis, S. aureus, Acinetobacter |
Special forms of bacterial meningitis
Tuberculous meningitis (TBM) — caused by Mycobacterium tuberculosis:
• Commonest cause of chronic meningitis in India
• Route: haematogenous spread from primary focus → subependymal Rich foci rupture into subarachnoid space
• Course: subacute/chronic (days to weeks) — headache, low-grade fever, cranial nerve palsies (CN III, IV, VI from basal exudate)
• CSF: clear/xanthochromic, lymphocytic pleocytosis (100-400 cells/mm³), high protein, very low glucose, cobweb clot on standing
• AFB smear sensitivity: only 10-40%; culture is gold standard (slow, 4-6 weeks); CBNAAT (GeneXpert Ultra) is now first-line rapid test
Viral (aseptic) meningitis:
• Enteroviruses (most common — Coxsackievirus, Echovirus, Enterovirus 71)
• Mumps virus, HSV-2, HIV (primary infection), West Nile Virus
• CSF: clear, lymphocytic pleocytosis, mildly elevated protein, normal glucose
• Self-limiting; no specific antiviral therapy except HSV (aciclovir) and HIV (ART)
Fungal meningitis:
• Cryptococcus neoformans — subacute meningitis in immunocompromised (HIV, steroids, organ transplant)
• CSF: clear, lymphocytic, elevated protein, LOW glucose; India ink preparation shows encapsulated yeasts
• Cryptococcus gattii — sporadic in immunocompetent (Southern India cases reported)
• Cryptococcal antigen (CrAg) latex agglutination test — highly sensitive and specific
Parasitic meningitis:
• Naegleria fowleri — primary amoebic meningoencephalitis (PAM); acquired via swimming in warm freshwater; rapidly fatal; CSF shows amoebic trophozoites on wet mount
• Angiostrongylus cantonensis — eosinophilic meningitis; consumed raw molluscs; CSF eosinophilia
• Plasmodium falciparum — cerebral malaria (technically encephalitis, not meningitis)

CSF Findings in Meningitis
Laboratory Diagnosis of Meningitis — CSF Analysis
CSF Analysis in Meningitis
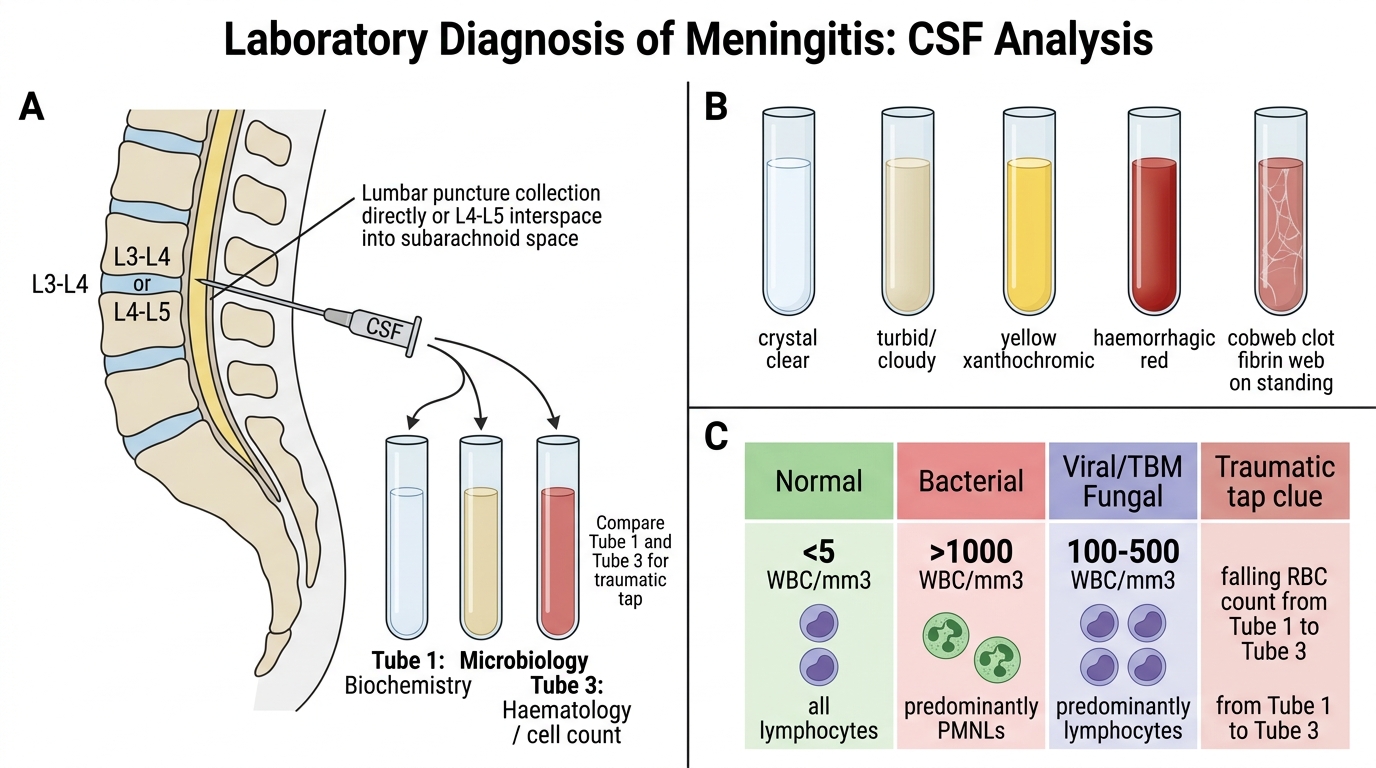
CSF is obtained by lumbar puncture (L3-L4 or L4-L5 interspace). Three tubes are typically collected: Tube 1 (biochemistry), Tube 2 (microbiology), Tube 3 (haematology — cell counts, to compare with tube 1 for traumatic tap).
Macroscopic appearance:
| Appearance | Interpretation |
|---|---|
| Crystal clear | Normal / viral / early TBM |
| Turbid/cloudy | Bacterial (>200 cells/mm³) |
| Xanthochromic (yellow) | Subarachnoid haemorrhage, jaundice, high protein, old TBM |
| Haemorrhagic | SAH or traumatic tap |
| Cobweb clot on standing | Tuberculous meningitis (fibrin web) |
Cell count and differential:
• Normal: <5 WBC/mm³ (all lymphocytes)
• Bacterial: >1000 WBC/mm³, predominantly PMNLs (neutrophils)
• Viral / TBM / Fungal: 100-500 WBC/mm³, predominantly lymphocytes
Biochemistry:
| Parameter | Normal | Bacterial | Viral | TBM | Fungal |
|---|---|---|---|---|---|
| Protein (g/L) | 0.2-0.4 | >1.0 | 0.5-1.0 | 1.0-3.0 | 0.5-1.5 |
| Glucose (mmol/L) | 2.5-4.0 (60-70% of blood glucose) | Very low (<2.2) | Normal | Low (<2.2) | Low |
| Chloride | 120-130 mEq/L | Low | Normal | Very low | Low |
Microbiological tests:
1. Gram stain (see below) — rapid morphological identification
2. India ink preparation — for Cryptococcus neoformans (unstained capsule appears as clear halo around dark-background yeast)
3. ZN stain — for AFB in suspected TBM (low sensitivity but fast)
4. Wet mount — for amoebic trophozoites in PAM
5. Culture:
- Blood agar, chocolate agar, MacConkey agar — for bacteria
- Löwenstein-Jensen medium / MGIT 960 — for M. tuberculosis (4-6 weeks)
- Sabouraud's dextrose agar — for fungi
6. Antigen tests:
- Cryptococcal antigen (CrAg) — latex agglutination or LFA (highly sensitive)
- Bacterial antigen detection (latex — for S. pneumoniae, N. meningitidis, H. influenzae b) — now replaced largely by PCR
7. Molecular tests:
- CSF GeneXpert Ultra (CBNAAT) — for M. tuberculosis and rifampicin resistance — recommended first-line in India
- Multiplex PCR (FilmArray Meningitis/Encephalitis panel) — detects 14 bacterial, viral, fungal agents simultaneously in 1 hour