Page 2 of 10
MI6.1-3 | CNS Infections — Meningitis & Encephalitis — SDL Guide (Part 2)
Reading and Interpreting CSF Gram Stain (MI6.3)
CSF Gram Stain: Procedure and Organism Patterns
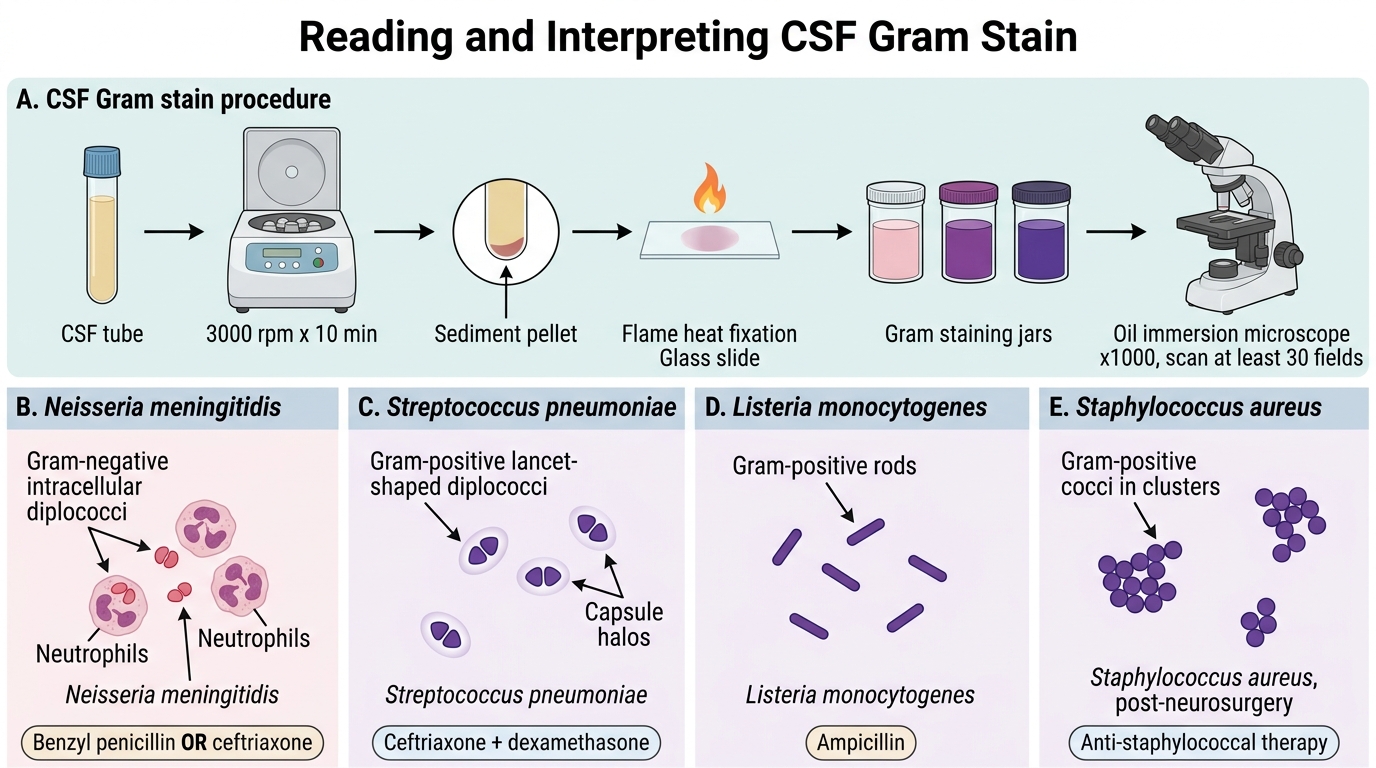
The CSF Gram stain is the most immediately actionable bedside diagnostic tool in meningitis. Systematic reading:
Procedure for CSF Gram stain:
1. Centrifuge CSF at 3000 rpm × 10 min to concentrate organisms.
2. Use the sediment for smear preparation; air dry, heat fix.
3. Perform Gram stain as standard (see staining practical module).
4. Examine under oil immersion (×1000) — scan at least 30 fields.
CSF Gram stain interpretation — organism-specific patterns:
| Gram stain finding | Likely organism | Empiric treatment |
|---|---|---|
| Gram-negative diplococci (intracellular, kidney-shaped) | Neisseria meningitidis | Benzyl penicillin OR ceftriaxone |
| Gram-positive diplococci (lancet-shaped, encapsulated) | Streptococcus pneumoniae | Ceftriaxone + dexamethasone |
| Gram-positive rods | Listeria monocytogenes | Ampicillin |
| Gram-positive cocci in clusters | Staphylococcus aureus (post-neurosurgery) | Vancomycin |
| Gram-negative rods (neonates, elderly, immunocompromised) | E. coli, Klebsiella | Ceftriaxone + gentamicin |
| Gram-negative coccobacilli | Haemophilus influenzae | Ceftriaxone |
| No organisms seen; lymphocytic, low glucose | TBM suspected | ZN stain, GeneXpert, ADA |

CSF Gram Stain in Meningococcal Meningitis
Sensitivity of CSF Gram stain by organism:
• S. pneumoniae: 90-95% in untreated cases
• N. meningitidis: 75-90%
• Gram-negative rods: 50-80%
• Listeria: 33-50%
• After antibiotic pretreatment: sensitivity drops significantly — cultures may become negative within hours
Reporting a CSF culture result:
• Positive culture: organism name, colony morphology, biochemical profile, antibiotic sensitivity profile (MIC)
• Negative culture with positive Gram stain: may indicate antibiotic pretreatment, fastidious or slow-growing organisms (Mycobacterium, viruses)
• For TBM: report AFB count per NTEP grading; note colony growth time on culture
CLINICAL PEARL
In suspected bacterial meningitis, do not delay antibiotics to wait for LP results if the patient shows signs of raised ICP (papilloedema, focal neurological signs, GCS <10). In such cases, take blood cultures, start empiric ceftriaxone immediately, then arrange CT head before LP. Every 30-minute delay in antibiotic therapy in bacterial meningitis increases mortality by approximately 5%. The Gram stain sensitivity drops significantly once antibiotics are given — but antibiotic sterilises CSF cultures within 2-4 hours; the biochemical profile (cells, protein, glucose) persists and guides diagnosis.
Encephalitis — Causes, Pathogenesis, and Diagnosis
Encephalitis: Causes, Pathogenesis, and Diagnosis
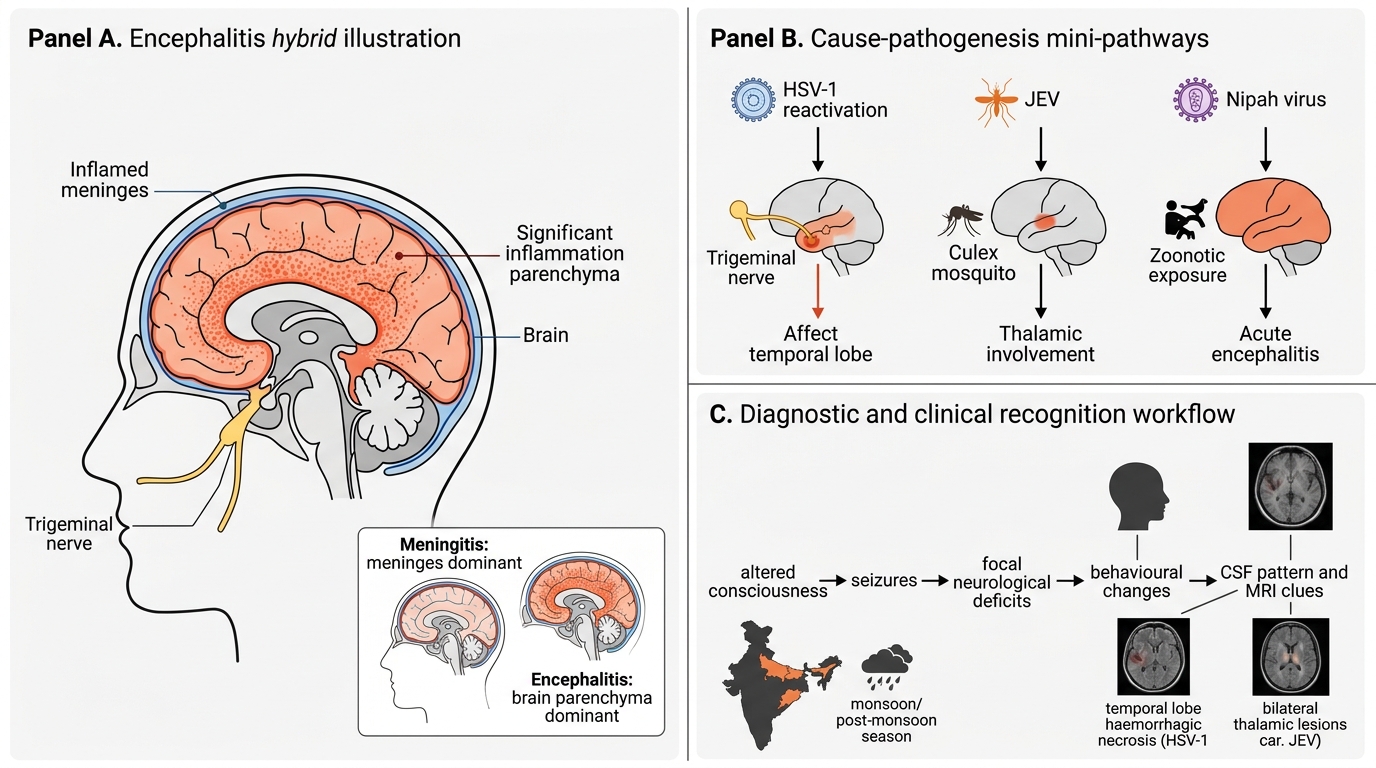
Encephalitis = inflammation of the brain parenchyma (not just meninges). Often combined with meningeal involvement (meningoencephalitis).
Key distinction from meningitis:
• Meningitis — meningeal signs dominant (neck stiffness, Kernig's, Brudzinski's)
• Encephalitis — altered consciousness, seizures, focal deficits, behavioural changes
Major viral causes of encephalitis:
| Virus | Transmission | Key feature | India context |
|---|---|---|---|
| Herpes simplex virus 1 (HSV-1) | Reactivation via trigeminal nerve | Temporal lobe involvement (limbic encephalitis); haemorrhagic necrosis; treat with aciclovir | Sporadic; commonest treatable cause worldwide |
| Japanese encephalitis virus (JEV) | Culex mosquito bite | Acute encephalitis; thalamic lesions on MRI; CSF — lymphocytic, mildly elevated protein, normal glucose | Endemic India (UP, Bihar, Assam, Odisha); seasonal (monsoon/post-monsoon); JE vaccine national program |
| Nipah virus | Bats → infected pigs/humans; human-to-human spread | Acute encephalitis with respiratory involvement; high mortality (40-70%); BSL-4 pathogen | Kerala outbreaks 2018, 2019, 2023 |
| Rabies virus | Dog/bat bite | Furious or paralytic form; Negri bodies in Purkinje cells; universally fatal once symptomatic | India: 36% of global rabies deaths |
| Enteroviruses | Faecal-oral | Enterovirus 71 — hand, foot, mouth disease + brainstem encephalitis | Epidemic in India |
| West Nile Virus | Culex mosquito | Meningoencephalitis; flaccid paralysis | Cases in Kerala, Karnataka |
Bacterial encephalitis:
• Listeria monocytogenes — brainstem encephalitis (rhombencephalitis)
• Mycobacterium tuberculosis — tuberculous encephalitis
• Rickettsia — scrub typhus (leading cause of febrile encephalitis in South India)
Parasitic:
• Plasmodium falciparum — cerebral malaria (sequestration of parasitised RBCs in cerebral capillaries)
• Trypanosoma brucei — sleeping sickness (not endemic in India but global context)
• Toxoplasma gondii — ring-enhancing lesions in HIV/AIDS

MRI Patterns in CNS Infections
Laboratory diagnosis of encephalitis:
• CSF: usually lymphocytic pleocytosis, normal glucose; RBCs in HSV (haemorrhagic)
• PCR on CSF: gold standard for HSV (sensitivity >95%), JEV, Enterovirus, Nipah
• Serology: JEV IgM in CSF or serum (MAC-ELISA) — first-line for JE; Nipah ELISA
• Brain biopsy: reserved for atypical/diagnostic uncertainty — shows Negri bodies (rabies), Cowdry A inclusions (HSV), perivascular cuffing
• EEG: temporal lobe periodicity in HSV; diffuse slowing in others
SELF-CHECK
A 35-year-old farmer from Bihar presents in August with fever, headache, altered sensorium, and seizures following a course of mosquito bites. CSF shows 120 lymphocytes/mm³, protein 90 mg/dL, glucose 55 mg/dL (blood glucose 90 mg/dL). Gram stain is negative. What is the most appropriate next diagnostic test?
A. CSF culture on Löwenstein-Jensen medium for Mycobacterium
B. CSF GeneXpert (CBNAAT) for tuberculosis
C. CSF and serum Japanese encephalitis virus IgM (MAC-ELISA)
D. India ink preparation for Cryptococcus
Reveal Answer
Answer: C. CSF and serum Japanese encephalitis virus IgM (MAC-ELISA)
The clinical picture — Bihar, August (post-monsoon), mosquito exposure, lymphocytic CSF with normal glucose and negative Gram stain — is classic for Japanese encephalitis virus (JEV) infection. MAC-ELISA for JEV IgM in CSF or serum is the gold standard diagnostic test. TBM would show lower glucose and more protein; Cryptococcus would be suspected in immunocompromised patients with very low glucose and a positive India ink or CrAg test.
SELF-CHECK
On CSF Gram stain from a 22-year-old with purulent meningitis, you see lancet-shaped Gram-positive diplococci. What is the most likely organism and the drug of choice?
A. Neisseria meningitidis — benzyl penicillin
B. Streptococcus pneumoniae — ceftriaxone plus dexamethasone
C. Listeria monocytogenes — ampicillin
D. Haemophilus influenzae — chloramphenicol
Reveal Answer
Answer: B. Streptococcus pneumoniae — ceftriaxone plus dexamethasone
Lancet-shaped (flame/candle-shaped) Gram-positive diplococci in CSF are pathognomonic of Streptococcus pneumoniae (pneumococcal meningitis). Treatment of choice is ceftriaxone (or benzyl penicillin if sensitive) plus dexamethasone to reduce inflammation and prevent neurological complications (deafness). Neisseria meningitidis appears as Gram-negative kidney-shaped diplococci. Listeria produces Gram-positive rods, not diplococci.