Page 4 of 14
MI3.5-8 | Enteric Fever, PUO & Sepsis — SDL Guide
Learning Objectives
- Define pyrexia of unknown origin (PUO) and classify its infective causes with appropriate diagnostic modalities
- Classify enteric fever pathogens and describe the clinical course, pathogenesis, complications, and laboratory diagnosis of enteric fever
- Select the most appropriate laboratory test for enteric fever based on the duration of illness and carrier status
- Read and interpret serological test results (Widal test) in suspected enteric fever, noting their limitations
INSTRUCTIONS
Typhoid fever remains one of the top five causes of fever in Indian hospitals. PUO is a clinical puzzle where microbiology holds the key. This module follows the patient's journey — from Peyer's patches to bacteraemia to the Widal tube — equipping you with the systematic approach needed to investigate fever without an obvious source.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 28 (Salmonella) (textbook)
- Harrison's Principles of Internal Medicine — Enteric (Typhoid) Fever, Fever of Unknown Origin (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old college student from Puducherry presents with 10 days of continuous fever (38.8°C), headache, constipation, and a mild cough. On Day 8, his doctor noticed the fever was 'step-ladder' in pattern and ordered a Widal test which returned: O antigen 1:160, H antigen 1:80. He was labelled as 'enteric fever' and started on ciprofloxacin.
On Day 14, he returns — worse. Blood cultures (taken on Day 12) now flag positive after 48 hours: Salmonella Typhi, MDR, resistant to fluoroquinolones.
Two questions:
1. Was the Widal result truly diagnostic?
2. Why was the blood culture more useful than the Widal, and what was the ideal timing for each test?
By the end of this session you will know precisely which test to order on which day of enteric fever — and why.
WHY THIS MATTERS
India has an estimated 4–6 million enteric fever cases annually. Typhoid kills approximately 40,000 Indians per year — almost all preventable deaths. The emergence of Multi-Drug Resistant (MDR) and extensively drug resistant (XDR) Salmonella Typhi has made correct laboratory diagnosis critical — you cannot guess the antibiotic. PUO is the presenting diagnosis in up to 20% of inpatient fevers in Indian hospitals; a systematic microbiological approach catches the treatable causes before organ failure.
RECALL
Before proceeding, recall:
- Salmonella is a Gram-negative, facultative intracellular organism belonging to the family Enterobacteriaceae
- O antigens = somatic (lipopolysaccharide, LPS) cell wall antigens; H antigens = flagellar; Vi antigen = capsular (virulence)
- Peyer's patches — lymphoid aggregates in the terminal ileum
- The Widal test is an agglutination test (tube or slide) — if you are unclear on how agglutination reactions work, quickly revise before continuing
Pyrexia of Unknown Origin (PUO): Definition & Causes
Pyrexia of Unknown Origin: Definition, Causes, and Diagnostic Approach
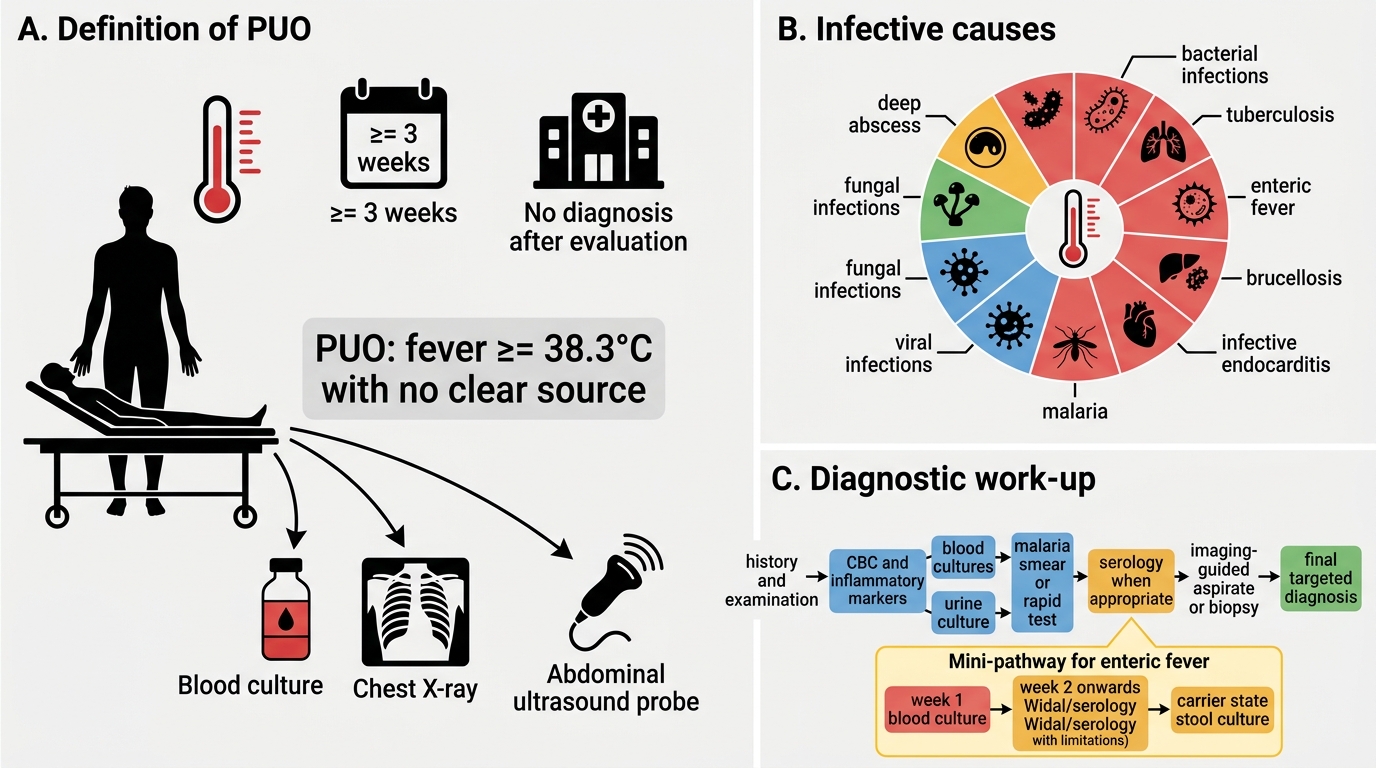
PUO was defined by Petersdorf & Beeson (1961) as:
- Fever >38.3°C (101°F) on several occasions
- Duration >3 weeks
- No diagnosis after 1 week of thorough inpatient investigation
Modified Durack-Street classification (1991) adds sub-types: classic PUO (the original), nosocomial PUO, neutropenic PUO, and HIV-associated PUO.
Infective causes of PUO (the largest category — 30–40% in India):
| Category | Examples |
|---|---|
| Bacterial | Enteric fever, tuberculosis (commonest in India), brucellosis, infective endocarditis, liver abscess, osteomyelitis |
| Viral | EBV/CMV (infectious mononucleosis), HIV seroconversion |
| Parasitic | Malaria (most common infective PUO in endemic areas), kala-azar (visceral leishmaniasis) |
| Fungal | Histoplasmosis, disseminated candidiasis (immunocompromised) |
Diagnostic approach to infective PUO:
1. Detailed history — travel, animal exposure, sexual history, immunisation status, drug history
2. Complete examination — lymph nodes, spleen, fundus, murmurs
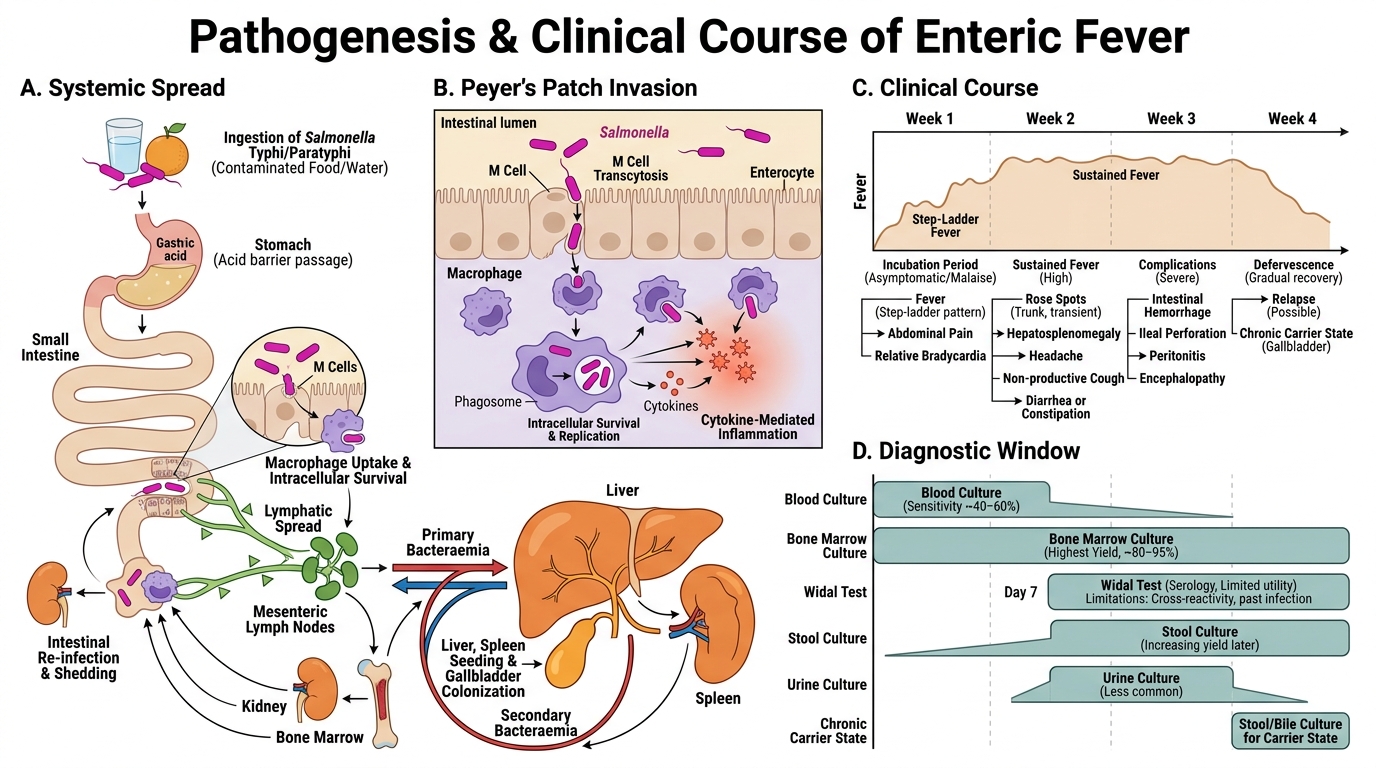
3. Repeated blood cultures (3–6 sets) — gold standard for bacterial PUO
4. Serology panel — based on epidemiology: Widal, Weil-Felix, Brucella agglutination, Paul-Bunnell, HIV ELISA
5. Bone marrow biopsy and culture — highest yield in enteric fever (90%), TB, kala-azar — valuable when blood cultures negative
6. Imaging — ultrasound (liver abscess, lymphadenopathy), CT, PET-CT for occult neoplasm vs infection
7. Molecular diagnostics — 16S rRNA PCR, Xpert MTB/RIF
Enteric Fever: Pathogens & Classification
Enteric Fever Pathogens and Classification
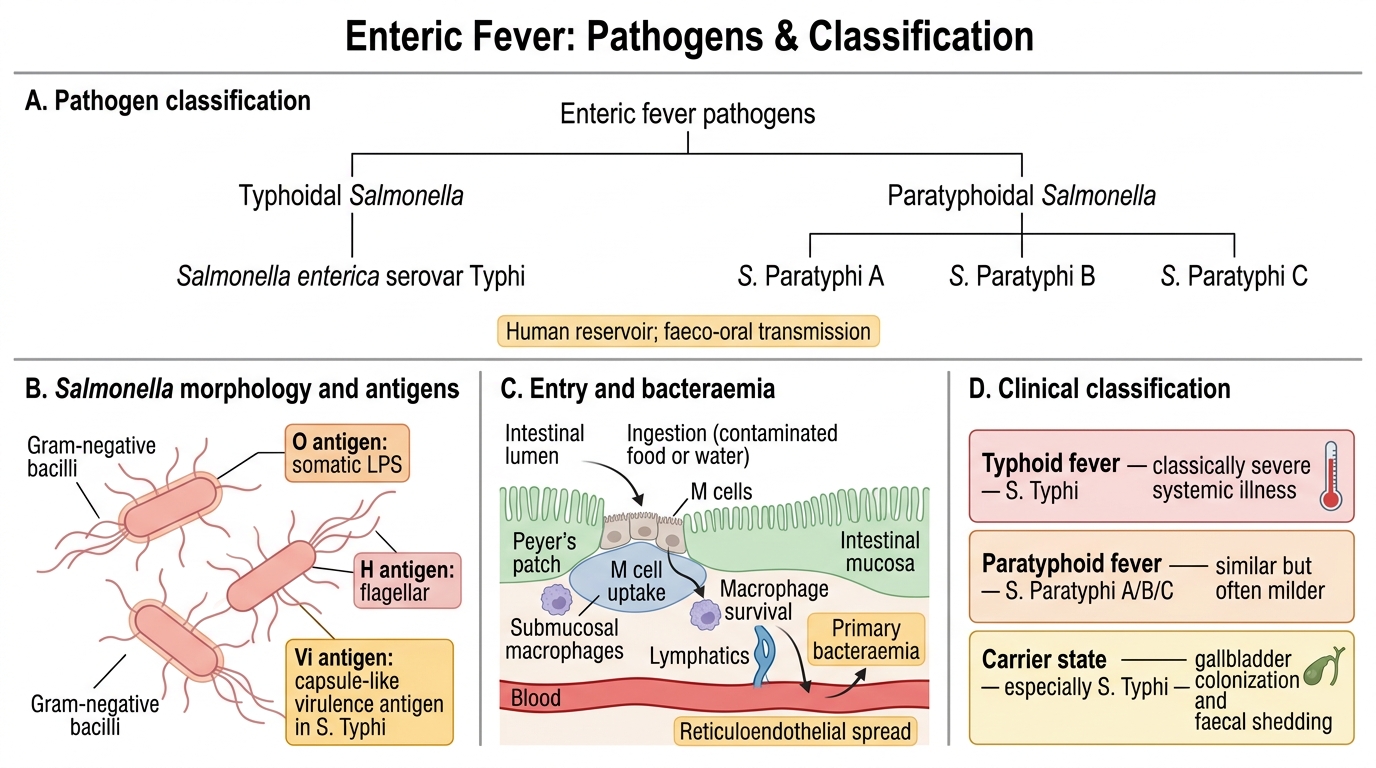
Enteric fever = typhoid + paratyphoid fever.
Causative organisms:
| Species | Biovar | Serovar | Disease |
|---|---|---|---|
| Salmonella enterica | Typhi | Typhi | Typhoid fever (most severe) |
| Salmonella enterica | Paratyphi A | Paratyphi A | Paratyphoid A (milder; common in India) |
| Salmonella enterica | Paratyphi B | Schottmuelleri | Paratyphoid B |
| Salmonella enterica | Paratyphi C | Hirschfeldii | Paratyphoid C (rare) |
Salmonella Typhi characteristics:
- Gram-negative, motile (peritrichous flagella), non-sporing, non-capsulate (except Vi antigen — a polysaccharide virulence capsule that helps evade phagocytosis)
- Kauffmann-White scheme — serotyping based on O, H, Vi antigens:
- O antigen: group D (1, 9, 12)
- H antigen: phase 1 'd'
- Vi antigen: present (marker of virulence; lost in Vi-negative mutants)
- Reservoir: Exclusively humans (carrier state — chronic biliary carrier)
- Transmission: Faeco-oral route; contaminated water/food — the 5 Fs (Food, Fingers, Flies, Faeces, Fomites)
Drug resistance pattern (important for India):
- MDR S. Typhi: resistant to chloramphenicol, ampicillin, co-trimoxazole (all first-line agents)
- Fluoroquinolone resistance: nalidixic acid-resistant S. Typhi (NARST) — reduced susceptibility to ciprofloxacin
- XDR S. Typhi (Pakistan outbreak 2016–2019): also resistant to 3rd-gen cephalosporins + fluoroquinolones; only azithromycin and carbapenems remain
- Antibiotic of choice for susceptible strains: Fluoroquinolones; for MDR: azithromycin or 3rd-gen cephalosporins (ceftriaxone)
Pathogenesis & Clinical Course of Enteric Fever
Enteric Fever: Pathogenesis, Clinical Course, and Diagnostic Timing
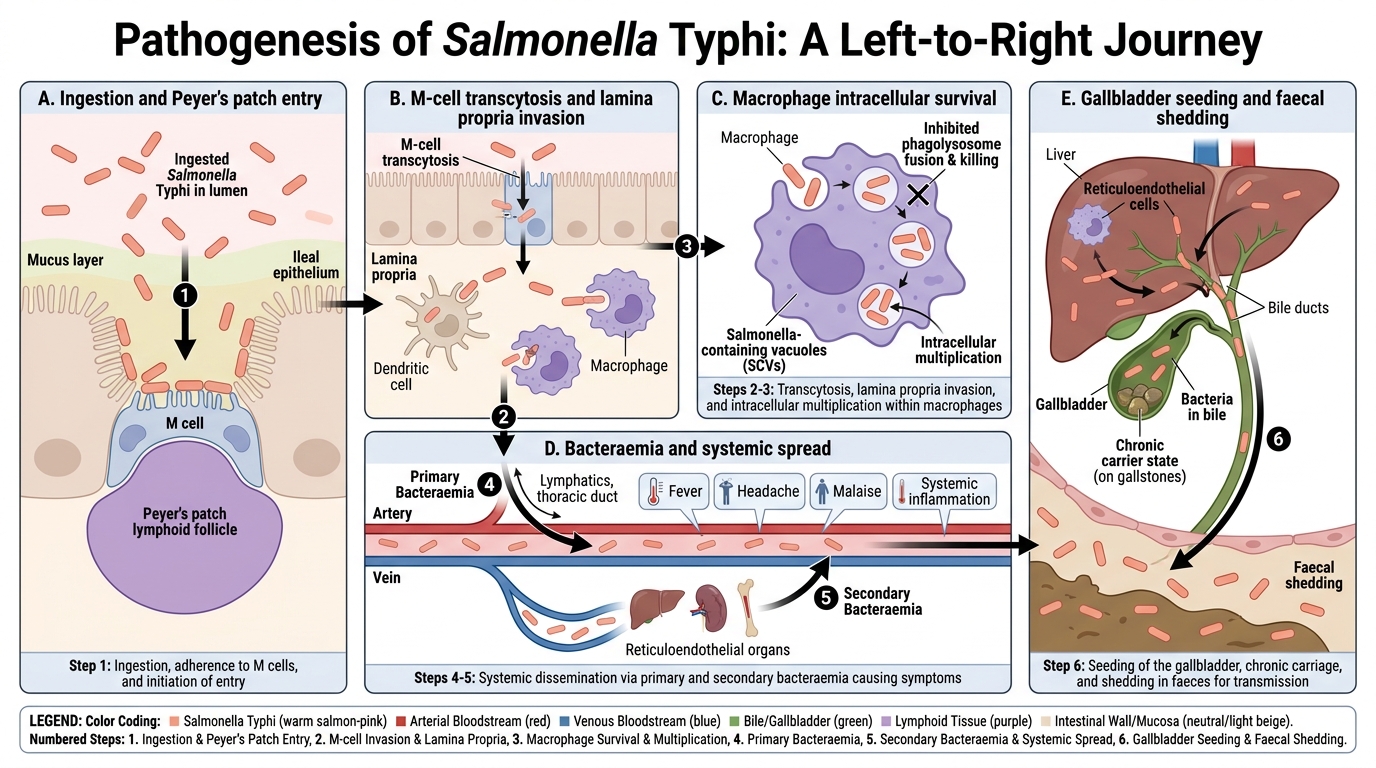
Pathogenesis — step by step:
- Ingestion — infective dose 10⁵–10⁷ organisms (lower for S. Typhi in contaminated water)
- Ileal invasion — Salmonella crosses the intestinal epithelium via M-cells overlying Peyer's patches, enters the lamina propria
- Intracellular survival — engulfed by macrophages in Peyer's patches; survives via Salmonella Pathogenicity Islands (SPI-1, SPI-2) — suppresses phagosome-lysosome fusion
- Primary bacteraemia — organisms reach mesenteric lymph nodes → thoracic duct → bloodstream (end of incubation period, 1–2 weeks)
- Systemic seeding — liver, spleen, bone marrow, gallbladder (gallbladder = reservoir for chronic carrier state)
- Secondary bacteraemia — organisms re-enter bloodstream from liver/spleen (Week 2–3 of illness); correlates with peak clinical fever
- Re-invasion of Peyer's patches — hypersensitivity reaction in sensitised lymphoid tissue → necrosis, ulceration → intestinal perforation (Week 3–4)
Clinical stages:
| Week | Stage | Features |
|---|---|---|
| 1 | Incubation/early | Step-ladder fever, headache, constipation, dry cough, relative bradycardia |
| 2 | Bacteraemic | High fever (39–40°C), rose spots (faint pink macules on trunk — pathognomonic), splenomegaly, hepatomegaly |
| 3 | Complication | Intestinal ulcers at risk of perforation and haemorrhage; fever starts to decline |
| 4 | Resolution | Defervescence; risk of relapse if undertreated |
Complications:
- Intestinal: Perforation (most feared, 1–3%), haemorrhage
- Systemic: Typhoid hepatitis, myocarditis, encephalopathy, DIC
- Carrier state: Chronic biliary carrier (usually female; chronic cholecystitis) — excretes organisms in bile/faeces for >1 year
Salmonella Typhi Pathogenesis
CLINICAL PEARL
Relative bradycardia (Faget's sign): In most fevers, heart rate rises ~10 bpm per degree Celsius. In typhoid fever, the heart rate paradoxically does NOT rise proportionately with the temperature — this relative bradycardia is caused by S. Typhi endotoxin acting on the cardiac conduction system. It is a classic bedside clue, though not pathognomonic (also seen in brucellosis, Legionella, dengue).