Page 5 of 14
MI3.5-8 | Enteric Fever, PUO & Sepsis — SDL Guide (Part 2)
Laboratory Diagnosis: Which Test on Which Day?
Enteric Fever Laboratory Diagnosis by Week of Illness
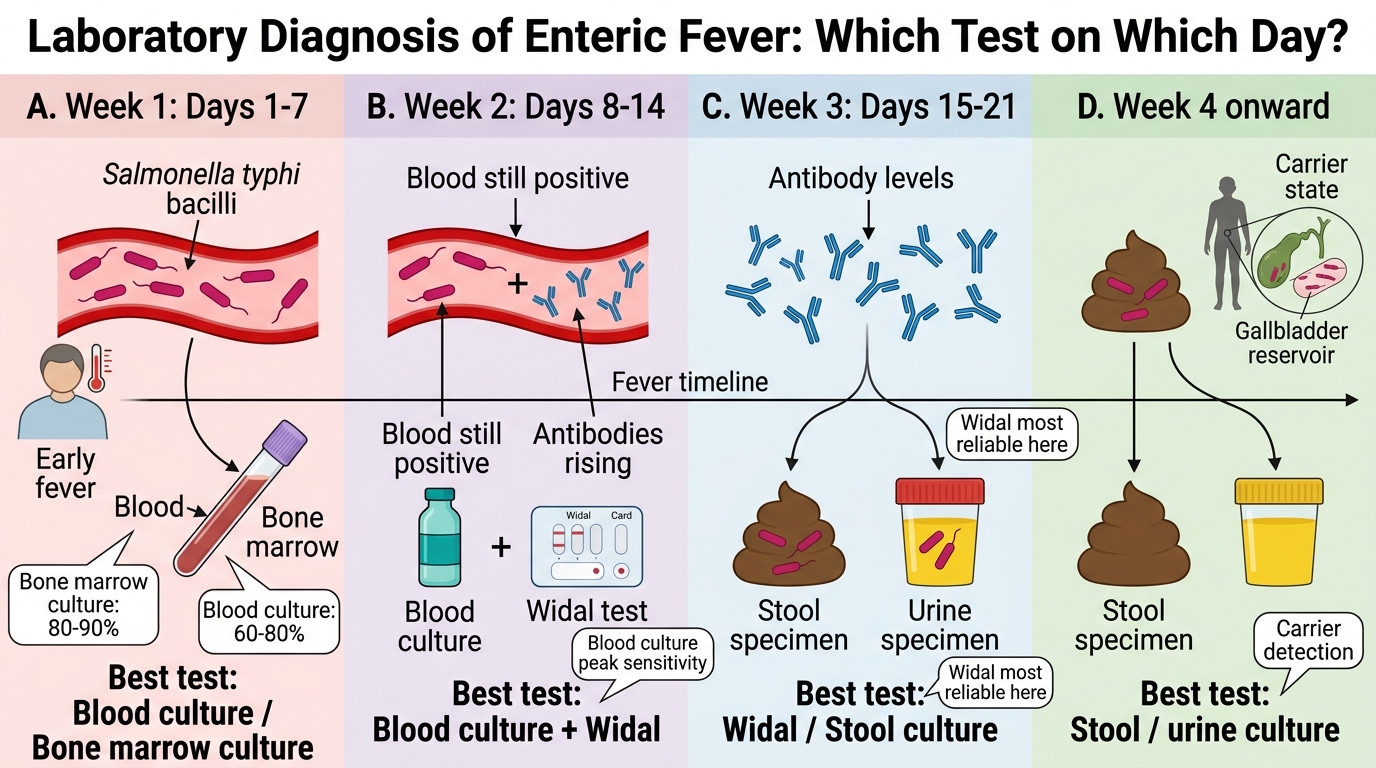
This is the single most high-yield examination topic in enteric fever microbiology. The choice of test depends on which week of illness the patient presents in:
| Week of Illness | Organisms in | Best Test | Sensitivity |
|---|---|---|---|
| Week 1 (Days 1–7) | Blood, bone marrow | Blood culture / Bone marrow culture | 80–90% (BM) / 60–80% (blood) |
| Week 2 (Days 8–14) | Blood still positive; antibodies rising | Blood culture + Widal | Blood culture peak sensitivity |
| Week 3 (Days 15–21) | Urine, stool; antibodies high | Widal / Stool culture | Widal most reliable here |
| Week 4 | Stool, urine | Stool/urine culture | Carrier detection |
Blood culture:
- Best specimen in first 2 weeks — take 10 mL blood in 100 mL broth (1:10 dilution to dilute out serum bactericidal factors)
- Transport: bile broth, brain-heart infusion broth, or tryptic soy broth at 37°C (NOT room temp, NOT refrigerated)
- Incubate 7–14 days (Salmonella may take longer than staphylococci)
- Bone marrow culture is the gold standard at ANY stage of illness (90% sensitivity even after antibiotics)
Widal test:
- Tube agglutination method (quantitative, preferred) or slide method (qualitative, rapid screening)
- Detects agglutinating antibodies against O antigen and H antigen of Salmonella
- Significant titres (single specimen): O ≥ 1:160, H ≥ 1:160 (endemic areas — baseline titres higher, so use 4-fold rise in paired sera)
- O antibodies: rise early, fall quickly — indicate acute/current infection
- H antibodies: rise later, persist longer — indicate past infection or immunisation
- Vi antibody — detected in chronic carriers (chronic biliary carrier screening)
Stool/urine culture:
- Weeks 3–4 of illness and for carrier detection
- Selective media: Wilson-Blair bismuth sulphite agar (black metallic sheen — S. Typhi), MacConkey agar (NLF colonies), XLD (Xylose Lysine Deoxycholate) agar (red/pink colonies with black centres for Salmonella)
- Enrichment broth: Selenite F broth (before plating on selective agar)
Carrier detection:
- Stool culture × 3 (over 3 separate days)
- Vi agglutination: Vi titre ≥ 1:20 suggests carrier state → confirm with multiple stool cultures
- Vi-phage typing for epidemiological strain tracing

Diagnostic Window in Enteric Fever
SELF-CHECK
A 19-year-old student presents with 5 days of continuous fever, headache, and constipation. He is in his first week of illness. Which laboratory investigation offers the HIGHEST diagnostic yield at this stage?
A. Widal test (slide agglutination)
B. Stool culture on XLD agar
C. Blood culture (10 mL in bile broth)
D. Bone marrow biopsy + culture
Reveal Answer
Answer: D. Bone marrow biopsy + culture
Bone marrow culture has 90% sensitivity at ANY stage of enteric fever and remains positive even after a few doses of antibiotics — it is the gold standard. Blood culture (60–80%) is the practical first choice in Week 1. Widal test is most useful in Week 3. Stool culture has highest yield in Weeks 3–4. Slide Widal is only a screening test with low specificity.
Interpreting Widal Test Results
Interpreting Widal Test Results
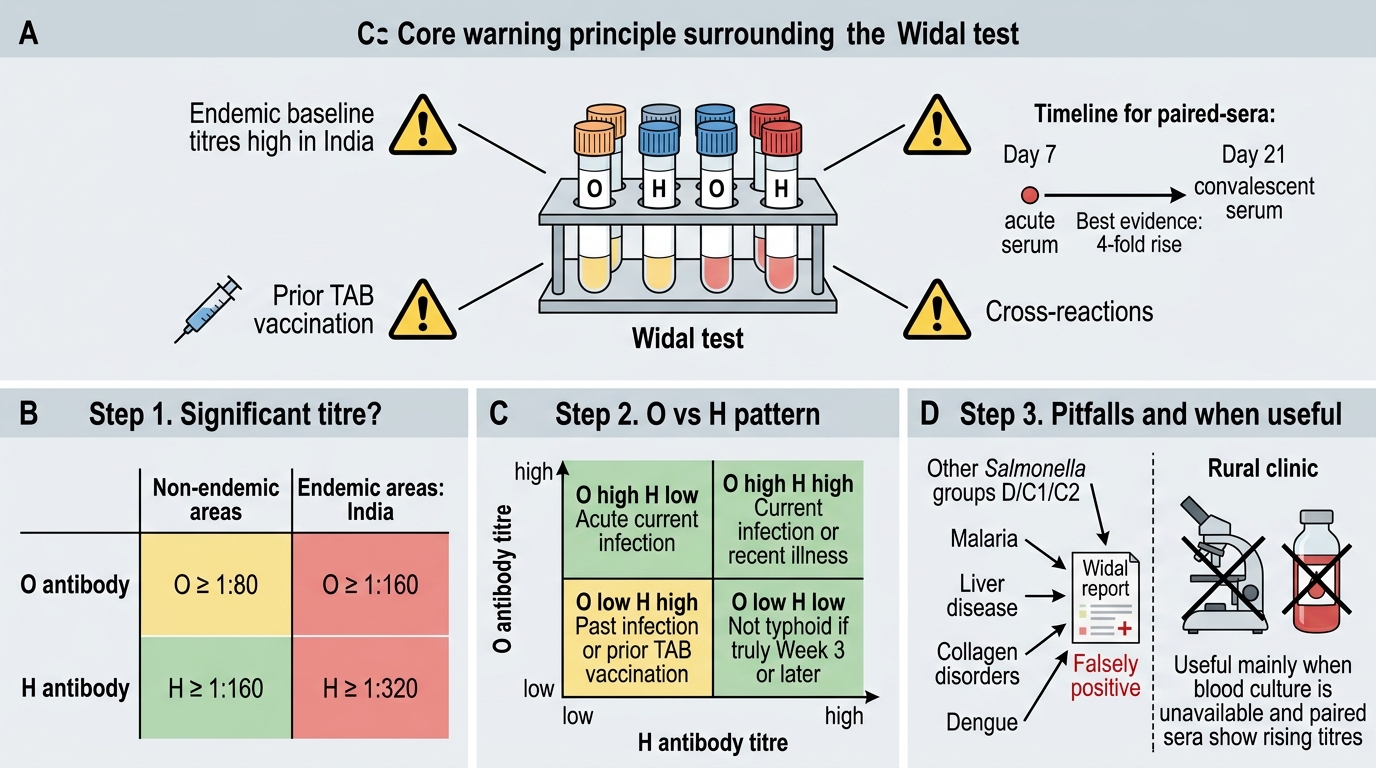
Critical principle: The Widal test is non-specific and fraught with interpretation pitfalls in India — endemic baseline titres are high due to widespread exposure, prior immunisation (TAB vaccine), and cross-reactions.
Step-by-step Widal interpretation:
Step 1 — Is there a significant titre?
- In non-endemic areas: O ≥ 1:80, H ≥ 1:160 considered significant
- In endemic areas (India): O ≥ 1:160, H ≥ 1:320 — or better yet, 4-fold rise between acute (Day 7) and convalescent (Day 21) paired sera
Step 2 — What pattern do you see?
| Pattern | Interpretation |
|---|---|
| O high, H low | Acute current infection |
| O high, H high | Current infection or recent illness |
| O low, H high | Past infection OR prior TAB vaccination |
| O low, H low | Not typhoid (if truly in Week 3+) |
Step 3 — Consider cross-reactions:
- Other Salmonella infections (group D, C1, C2)
- Malaria, liver disease, collagen disorders — may give false positive O
- Prior TAB vaccine — raises H titre only, not O
- Dengue — documented non-specific elevation
When is a positive Widal USEFUL?
- In resource-limited settings without blood culture capability
- When paired sera show a 4-fold rise
- Combined with clinical picture (Week 3 fever, rose spots, splenomegaly)
Newer tests (replacing Widal progressively):
- Typhidot / Typhi IgM dot-ELISA — detects IgM and IgG against S. Typhi 50 kDa OMP; sensitive in first week
- Typhidot-M — IgM only (eliminates IgG background — more specific in endemic areas)
- Tubex test — detects anti-O9 (S. Typhi specific LPS) antibodies; colorimetric; rapid
- PCR/qPCR — detects flagellin/Vi gene; available in reference laboratories
SELF-CHECK
A Widal test on a patient with 18 days of fever shows: O antigen 1:80, H antigen 1:320. Which interpretation is MOST appropriate?
A. Active typhoid fever — O titre is diagnostic
B. Likely past typhoid infection or TAB vaccination — H high, O low
C. Definitive diagnosis of typhoid — H titre exceeds threshold
D. False positive — malaria cross-reaction always gives high H
Reveal Answer
Answer: B. Likely past typhoid infection or TAB vaccination — H high, O low
A high H titre with low/borderline O titre indicates past infection or prior TAB vaccination (TAB vaccine predominantly stimulates H antibody). Active acute typhoid typically shows a rising O titre. H titres persist for months to years after infection or vaccination. This pattern alone should not be used to start typhoid treatment without clinical correlation and blood culture.
SELF-CHECK
A known typhoid patient completed treatment 4 months ago. He remains well but surveillance stool cultures are positive for S. Typhi. Which investigation BEST confirms chronic carrier status?
A. Repeat Widal test — if O titre elevated, confirms carrier
B. Vi agglutination test (Vi titre ≥ 1:20) plus 3 stool cultures
C. Single blood culture — bacteraemia rules in current disease
D. IgG ELISA for H antigen — persistence confirms carrier
Reveal Answer
Answer: B. Vi agglutination test (Vi titre ≥ 1:20) plus 3 stool cultures
Vi agglutination (Vi titre ≥ 1:20) is the standard screening test for chronic biliary carriers, followed by confirmation with ≥3 positive stool cultures. Widal O titre is not reliable for carrier diagnosis. Blood culture is typically negative in carriers. IgG ELISA for H antigen reflects past exposure, not carrier state.