Page 4 of 13
MI3.13 | HIV/AIDS — Epidemiology, Evolution & Opportunistic Infections — SDL Guide
Learning Objectives
- Describe the epidemiology of HIV/AIDS globally and in India
- Explain the etiopathogenesis and evolution of HIV infection — from primary infection to AIDS
- Enumerate the opportunistic infections associated with AIDS and their relationship to CD4+ count
- Describe the laboratory diagnosis of HIV — screening, confirmatory, and monitoring tests
- Outline the principles of prevention and management of HIV/AIDS including HAART
INSTRUCTIONS
HIV/AIDS is the defining epidemic of our era — and India is home to the third-largest HIV-positive population in the world. This session builds your understanding from the molecular level (CCR5 co-receptor, immune evasion) to the clinical level (which infection strikes at which CD4+ count) to the public health level (National AIDS Control Programme). Every clinical posting will involve HIV — either directly or as a factor in treatment decisions.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 66 (Retroviruses — HIV) (textbook)
- Harrison's Principles of Internal Medicine — Human Immunodeficiency Virus Disease: AIDS and Related Disorders (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 32-year-old lorry driver from Tamil Nadu presents with 6 weeks of fever, weight loss (8 kg in 3 months), and whitish plaques in his mouth that bleed on touching. His CD4+ count is 78 cells/μL. Sputum smear shows acid-fast bacilli. Silver stain of a bronchoalveolar lavage shows cyst-like organisms.
He has two infections that healthy adults never get: Pneumocystis jirovecii pneumonia and pulmonary tuberculosis — both occurring because his CD4+ count has collapsed below the thresholds that normally keep these pathogens in check.
This patient's journey from first HIV exposure to this moment took approximately 8–10 years. Every year of that trajectory could have been interrupted — by testing, by counselling, by antiretrovirals. The oral white plaques are oropharyngeal candidiasis — the first visible marker that his immune system is failing.
By the end of this session, you will understand that HIV is not a death sentence — but ignorance of its microbiology and management pathways is.
WHY THIS MATTERS
India has approximately 2.4 million people living with HIV (PLHIV) — the third-largest HIV-positive population globally. Andhra Pradesh, Telangana, Karnataka, Maharashtra, and Tamil Nadu bear the highest burden. India's National AIDS Control Programme (NACP) through NACO provides free testing (ICTC — Integrated Counselling and Testing Centres) and free antiretroviral therapy (ART) to all PLHIV. The HIV/AIDS Prevention and Control Act (2017) makes it illegal to discriminate against PLHIV. As a doctor, you will diagnose HIV, initiate ART conversations, and manage opportunistic infections — this is not a theoretical topic.
RECALL
Before proceeding, recall:
- CD4+ T lymphocytes (T-helper cells) — direct the immune response by activating macrophages, cytotoxic T cells, and B cells; normal count = 500–1,500 cells/μL
- Retrovirus — RNA virus that uses reverse transcriptase to transcribe its genome into DNA, which integrates into the host cell chromosome
- Opportunistic infection — infection by organisms that do not normally cause disease in immunocompetent hosts but exploit impaired immunity
- ELISA and Western blot — serological tests (recall: ELISA for sensitivity/screening; Western blot for specificity/confirmation)
HIV: Structure & Classification
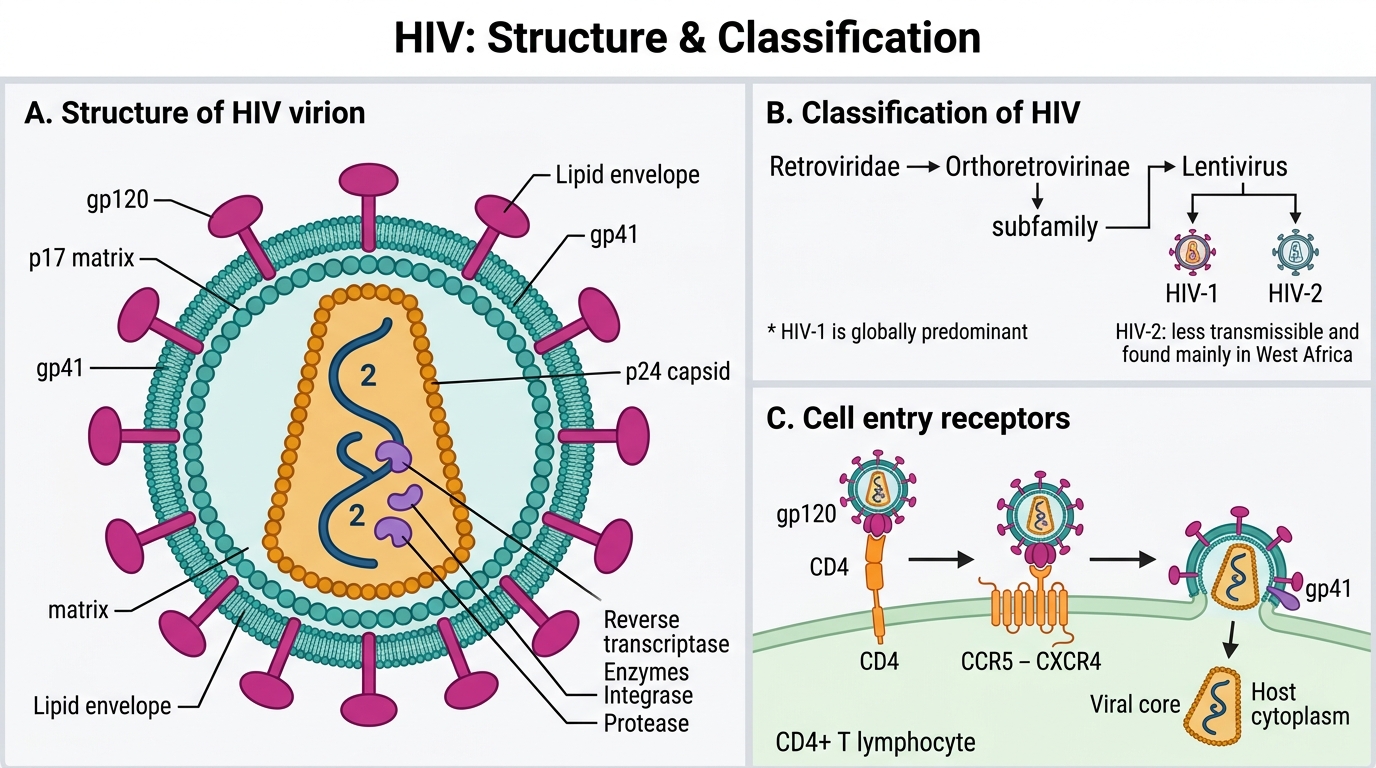
HIV Structure and Classification
HIV (Human Immunodeficiency Virus) belongs to:
- Family: Retroviridae
- Subfamily: Lentivirinae (lentiviruses = 'slow viruses' with long incubation)
- Two types: HIV-1 (pandemic; cause of most AIDS globally) and HIV-2 (less virulent; limited to West Africa)
Structure of HIV-1:
Genome: Two copies of single-stranded, positive-sense RNA (~9.7 kb)
Enzymes (encoded by pol gene):
- Reverse transcriptase (RT): RNA → DNA (with high error rate — ~1 error per replication → mutation and drug resistance)
- Integrase: inserts proviral DNA into host chromosome
- Protease: cleaves polyproteins into functional units during viral maturation
Structural proteins (gag gene):
- p24 (capsid) — most abundant; used as diagnostic antigen in 4th-generation ELISA
- p17 (matrix)
- p7 (nucleocapsid)
Envelope proteins (env gene):
- gp120 (surface glycoprotein) — binds CD4 receptor and CCR5/CXCR4 co-receptor on target cells
- gp41 (transmembrane) — mediates viral-cell membrane fusion after gp120 binding
Regulatory/accessory genes:
- tat: transactivation — markedly increases viral replication
- rev: regulates export of viral mRNA from nucleus
- vif, vpr, vpu, nef: immune evasion and viral fitness

Structure of HIV Virion
HIV Epidemiology & Transmission
HIV Epidemiology and Transmission
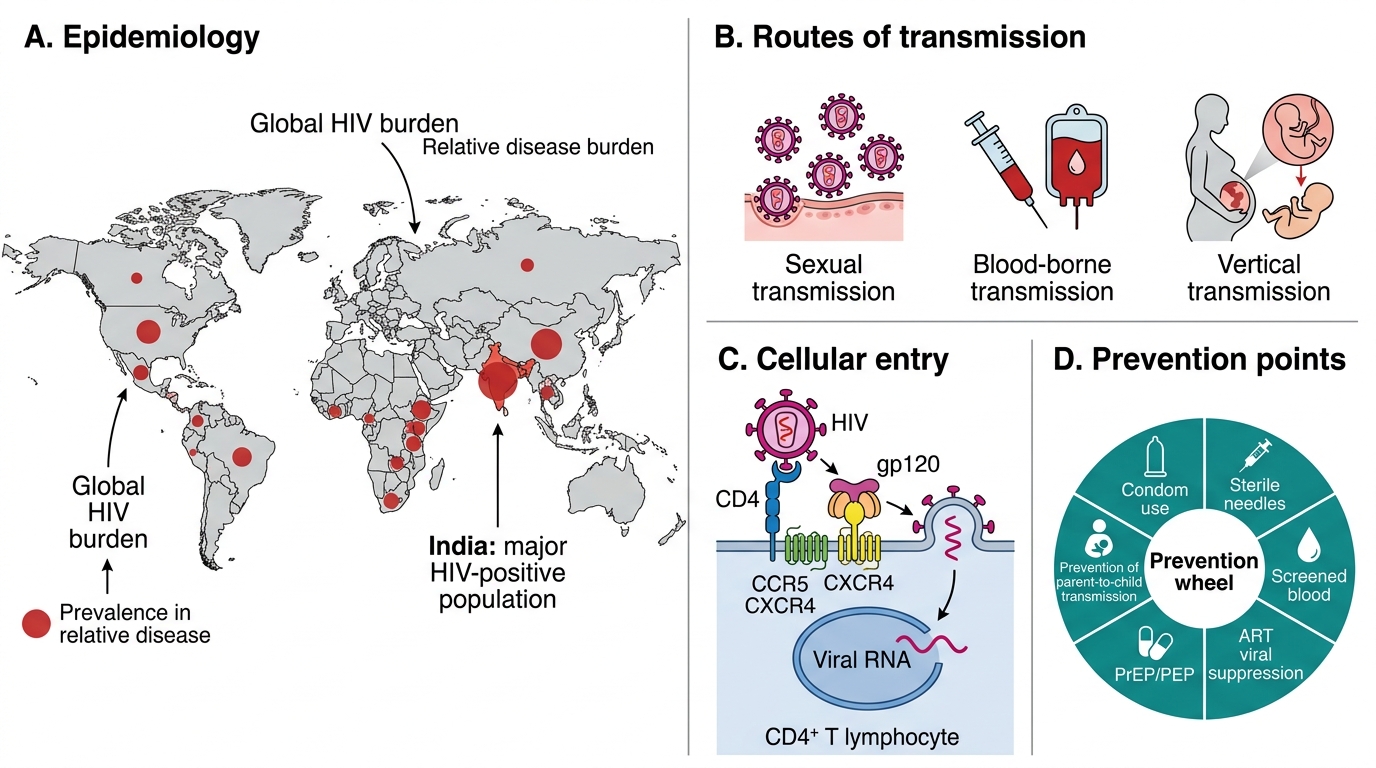
Global epidemiology:
- 39.9 million PLHIV worldwide (2023, UNAIDS)
- ~1.3 million new infections annually; ~630,000 deaths annually
- Sub-Saharan Africa: 67% of global burden
- India: ~2.4 million PLHIV (2022); adult HIV prevalence ~0.2% (declining, but heterogeneous)
High-prevalence groups in India (key populations):
- Sex workers and clients
- Men who have sex with men (MSM)
- Injecting drug users (IDUs)
- Truckers and migrant workers
- Partners and spouses of above groups
Routes of transmission:
| Route | Risk per exposure | Comments |
|---|---|---|
| Unprotected anal intercourse (receptive) | 1.4% | Highest per-act risk |
| Unprotected vaginal intercourse (receptive) | 0.08–0.19% | Most common route globally |
| Needle/syringe sharing | 0.63–2.4% | IDU; high risk |
| Needlestick injury (healthcare) | 0.3% | Professional occupational risk |
| Mother-to-child (vertical) | 15–45% without intervention | Antenatal, intrapartum, breastfeeding |
| Blood transfusion (untested) | 90–95% | Mandatory HIV testing of all blood donations in India |
NOT transmitted by: Casual contact, saliva, tears, sweat, insect bites, shared toilets, food/water.
Window period:
- Time between HIV infection and detectable antibodies on standard ELISA
- 4th-generation (antigen-antibody combination) ELISA: window period ~18 days (detects p24 antigen before antibodies appear)
- Older 3rd-generation ELISA: window period 3–12 weeks
Pathogenesis & Natural History of HIV Infection
Pathogenesis and Natural History of HIV Infection
Entry mechanism:
1. gp120 binds CD4 receptor on T-helper lymphocytes, macrophages, dendritic cells
2. Co-receptor binding: gp120 undergoes conformational change and binds CCR5 (on macrophages — M-tropic strains; early infection) or CXCR4 (on T cells — T-tropic strains; late infection)
3. gp41 mediates membrane fusion → viral core enters cytoplasm
4. Reverse transcriptase transcribes RNA → double-stranded DNA (proviral DNA)
5. Integrase inserts proviral DNA into host chromosome → latent reservoir (NOT eliminated by antiretrovirals)
6. Upon activation: tat drives viral replication → new virions bud and mature
CCR5 delta-32 mutation: Individuals homozygous for this mutation lack functional CCR5 → M-tropic HIV cannot enter → near-complete resistance to HIV infection (basis for CCR5 antagonists like maraviroc)
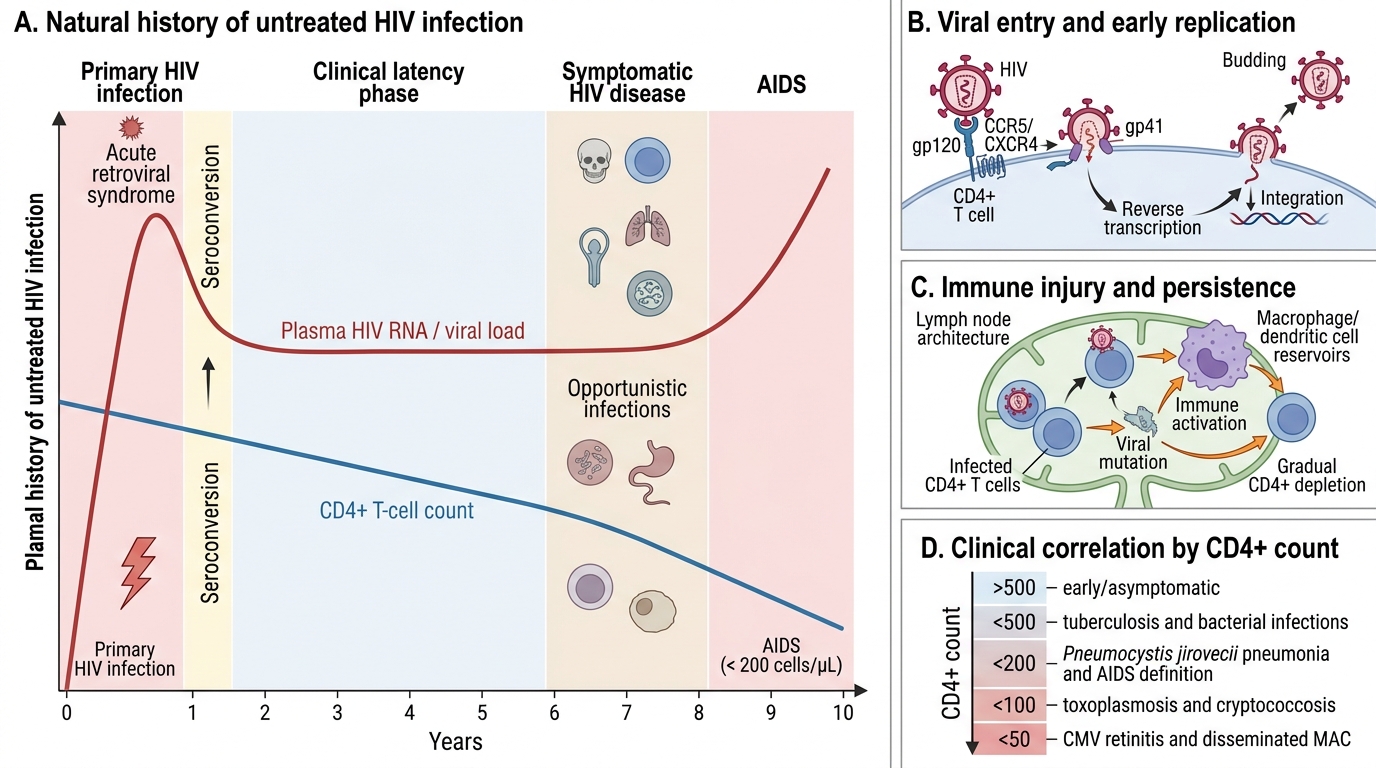
Natural history — three phases:
Phase 1 — Primary HIV infection (Acute Seroconversion Illness):
- 2–4 weeks after exposure
- Viral load VERY HIGH → massive CD4 depletion → partial immune reconstitution as CD8+ CTL response mounts
- Clinical: mononucleosis-like illness — fever, pharyngitis, lymphadenopathy, rash, myalgia, headache, sometimes meningitis
- Highly infectious (high viral load); window period — antibody-based tests may be NEGATIVE
- Spontaneous recovery in 2–4 weeks
Phase 2 — Chronic asymptomatic HIV infection (Clinical latency):
- Lasts 8–10 years (untreated)
- CD4+ count: 200–500 cells/μL (declining ~50–80 cells/μL per year)
- Viral load: 'setpoint' established; virus still replicating in lymph nodes
- Patient is asymptomatic but infectious
- Minor conditions: Persistent generalised lymphadenopathy (PGL), oral candidiasis, herpes zoster, seborrhoeic dermatitis
Phase 3 — AIDS (Acquired Immunodeficiency Syndrome):
- CD4+ count <200 cells/μL OR occurrence of an AIDS-defining illness (regardless of CD4 count)
- Without ART: progression to death within 1–3 years
- With ART: near-normal life expectancy

Natural History of HIV Infection
SELF-CHECK
A healthcare worker sustains a needlestick injury from an HIV-positive patient's blood. She is tested immediately by 4th-generation ELISA (antigen-antibody combination test) — the result is negative. This is MOST likely because:
A. She has not been infected — one negative test rules out HIV
B. She is in the window period — p24 antigen and antibodies are not yet detectable
C. The test is invalid — 4th-gen ELISA cannot detect recent infection
D. Needlestick risk is zero — healthcare workers cannot acquire HIV
Reveal Answer
Answer: B. She is in the window period — p24 antigen and antibodies are not yet detectable
The window period for 4th-generation (antigen-antibody combination) ELISA is approximately 18 days. Immediately after exposure, neither p24 antigen nor antibodies will be detectable. A single negative test immediately post-exposure does NOT exclude infection. Repeat testing at 6 weeks, 3 months, and 6 months is standard in occupational exposure protocols, alongside post-exposure prophylaxis (PEP) started within 72 hours. Needlestick risk is 0.3% per exposure — real, if low.