Page 5 of 13
MI3.13 | HIV/AIDS — Epidemiology, Evolution & Opportunistic Infections — SDL Guide (Part 2)
Opportunistic Infections: CD4+ Count Thresholds
CD4+ Count Thresholds for Opportunistic Infections in HIV
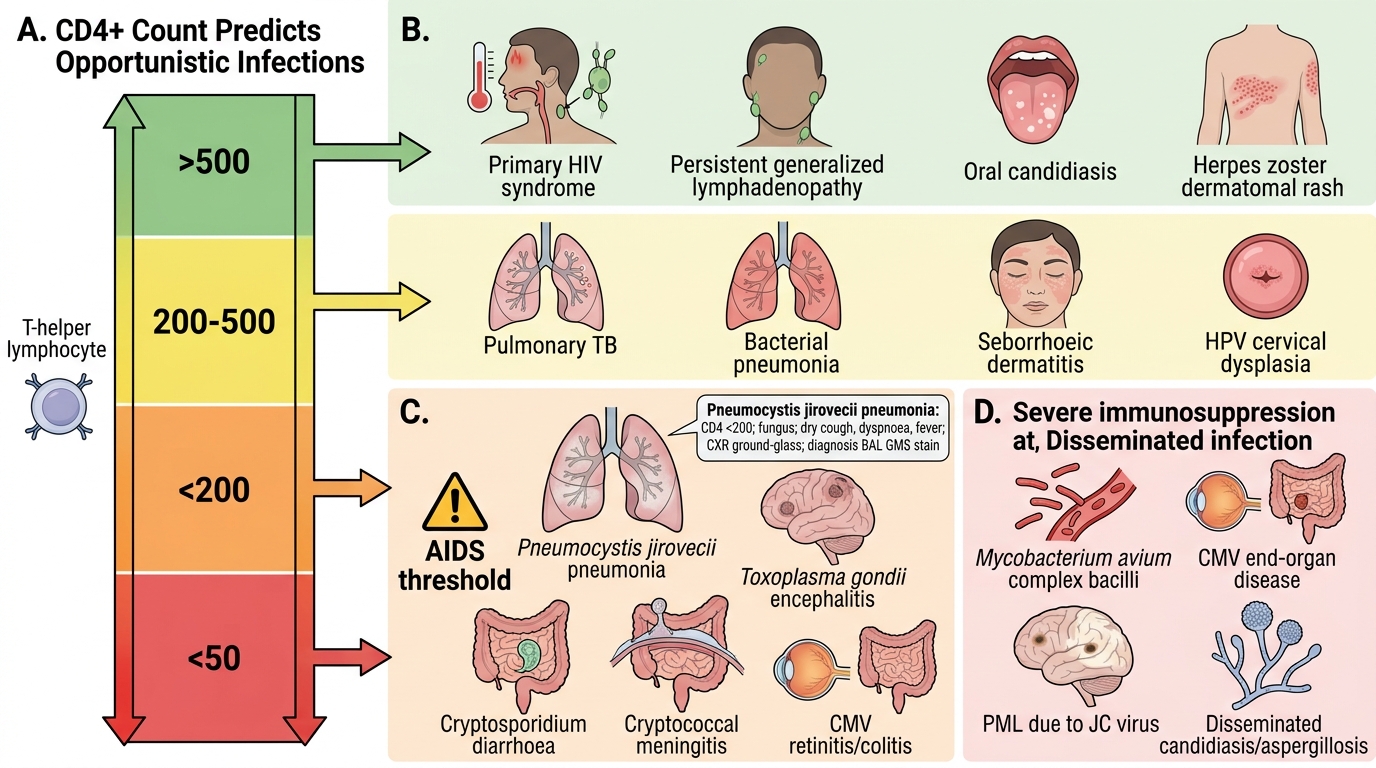
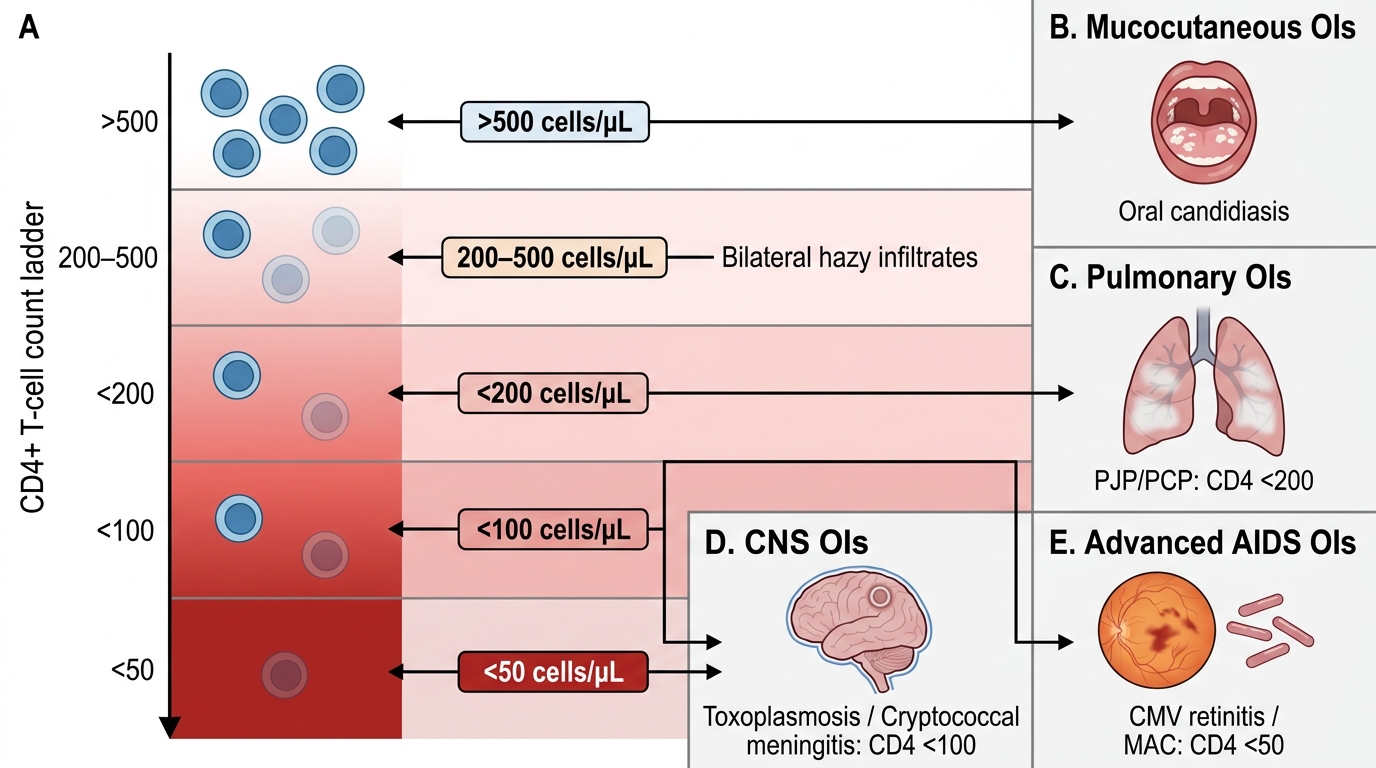
The CD4+ count predicts which opportunistic infections (OIs) are likely — this is a high-yield clinical correlation:
| CD4+ count (cells/μL) | Opportunistic Infections & Conditions |
|---|---|
| >500 | Primary HIV infection syndrome; persistent generalised lymphadenopathy |
| 200–500 | Oral candidiasis; herpes zoster (shingles); pulmonary TB; bacterial pneumonias; seborrhoeic dermatitis; cervical dysplasia (HPV) |
| <200 | AIDS threshold — Pneumocystis jirovecii pneumonia (PCP); Toxoplasma gondii encephalitis; Cryptosporidium diarrhoea; Cryptococcal meningitis (often at ~100); CMV retinitis/colitis |
| <50 | Disseminated Mycobacterium avium complex (MAC/MAI); CMV end-organ disease; PML (JC virus); Disseminated candidiasis/aspergillosis |
High-yield OIs to know in detail:
1. Pneumocystis jirovecii Pneumonia (PCP) — CD4 <200:
- Organism: Pneumocystis jirovecii (formerly carinii) — a fungus, not a protozoan (re-classified 2002)
- Presentation: Insidious onset dry cough, progressive dyspnoea, fever; CXR: bilateral diffuse interstitial infiltrates ('ground-glass appearance')
- Diagnosis: BAL staining — GMS (Gomori Methenamine Silver) or toluidine blue O staining shows cysts; DIF (Direct Immunofluorescence) with monoclonal antibodies (most sensitive)
- Treatment: Trimethoprim-sulfamethoxazole (TMP-SMX) — drug of choice; add corticosteroids if PaO₂ <70 mmHg
- Prophylaxis: TMP-SMX when CD4 <200 (primary prophylaxis)
2. Toxoplasma gondii Encephalitis — CD4 <100–200:
- Presentation: Fever, headache, focal neurological deficits, seizures; CT/MRI — multiple ring-enhancing lesions in basal ganglia
- Diagnosis: Serology (IgG anti-Toxoplasma — reactivation of latent infection); brain biopsy for confirmation
- Treatment: Pyrimethamine + sulfadiazine + folinic acid
3. Cryptococcal Meningitis — CD4 <100:
- Organism: Cryptococcus neoformans — encapsulated yeast
- Presentation: Subacute meningitis (weeks), headache, fever, altered sensorium; meningism may be minimal
- Diagnosis: India ink staining of CSF (encapsulated yeasts with halo); CrAg (Cryptococcal antigen) latex agglutination or LFA — most rapid and sensitive; CSF culture on Sabouraud agar
- Treatment: Amphotericin B + flucytosine (induction) → fluconazole (maintenance)
4. CMV Retinitis — CD4 <50:
- Presentation: Progressive painless visual loss, floaters
- Fundoscopy: Haemorrhagic necrotic retinitis ('pizza-pie' appearance)
- Treatment: Ganciclovir IV (then valganciclovir oral maintenance)
5. Tuberculosis — CD4 200–500 (and lower):
- Most common OI in India (TB-HIV coinfection)
- Atypical presentations at low CD4: disseminated TB, extrapulmonary TB (lymph node, meningeal)
- Smear may be negative (poor granuloma formation); culture + GeneXpert essential
- ART + ATT — start ART within 2–4 weeks of ATT initiation (not simultaneously — IRIS risk)
CLINICAL PEARL
Immune Reconstitution Inflammatory Syndrome (IRIS):
When ART is started in a severely immunocompromised patient with an active OI (especially TB or Cryptococcus), the recovering immune system mounts a vigorous inflammatory response against the existing pathogen → paradoxical worsening of the OI. This is IRIS — not treatment failure. It typically occurs within 4–8 weeks of ART initiation. Prevention: delay ART in TB meningitis patients until neurological stabilisation; for pulmonary TB and most other OIs, start ART within 2–4 weeks of OI treatment.
Laboratory Diagnosis of HIV
Laboratory Diagnosis of HIV
Screening tests:
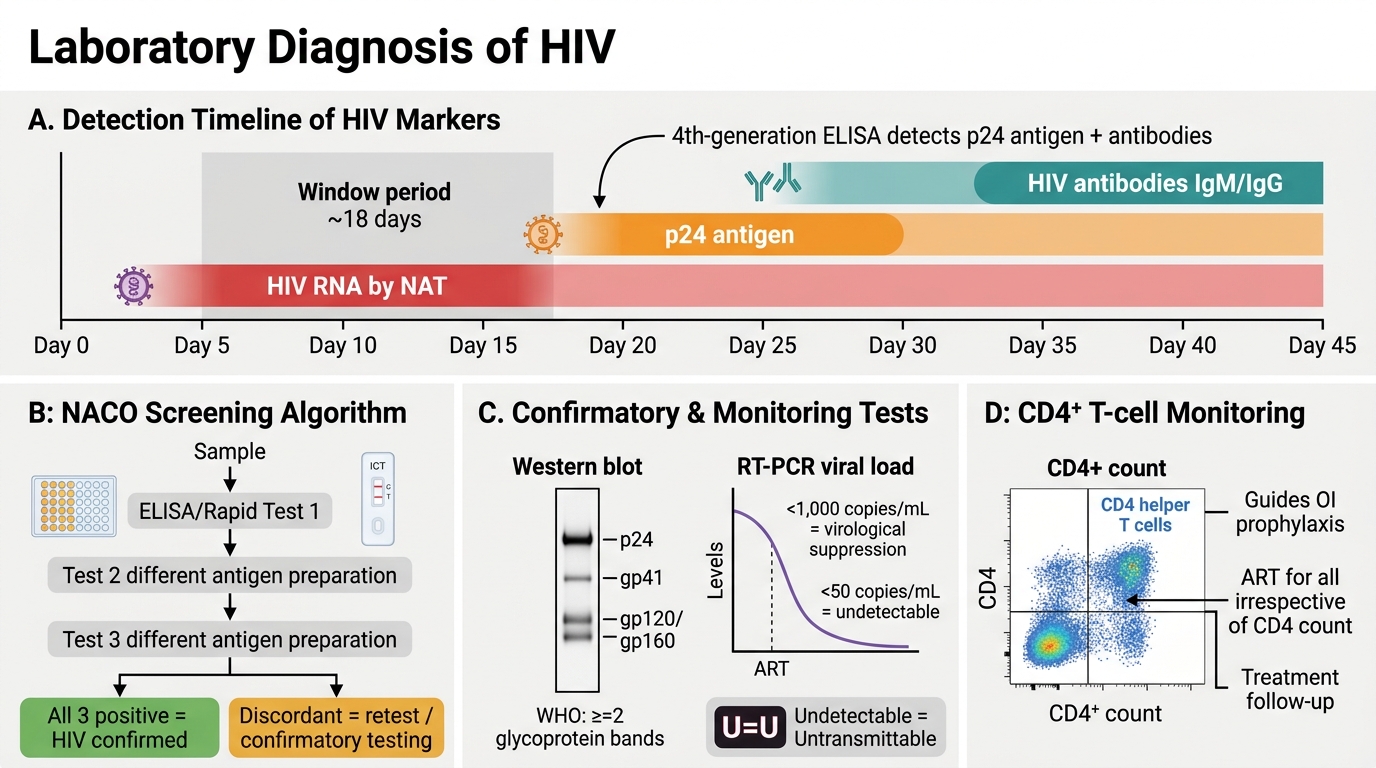
4th-generation ELISA (antigen-antibody combination assay) — current standard:
- Detects both HIV p24 antigen (appears 18 days post-infection) AND HIV antibodies (IgG/IgM against HIV-1 and HIV-2)
- Window period: ~18 days
- High sensitivity (>99.5%); specificity ~99.5%
- NACO algorithm (India): 3 ELISA kits in series (different antigen preparations) — positive on all 3 = confirmed HIV; discordant = retest/Western blot
Rapid tests (ICT-based):
- Point-of-care; results in 15–30 minutes; suitable for antenatal, ICTC settings
- Used in NACO's three-test algorithm at field level
Confirmatory tests:
Western blot:
- Detects antibodies against specific HIV proteins separated by electrophoresis
- Positive = bands at p24, gp41, gp120/gp160 (per WHO criteria: ≥2 glycoprotein bands)
- Current practice: largely replaced by NAT and 4th-gen ELISA algorithms; still used when needed
Viral load (RT-PCR / NAAT):
- Quantifies HIV RNA copies/mL plasma
- Not used for diagnosis (can be positive in window period — but not routinely used for this)
- Monitoring treatment response: Viral load <1,000 copies/mL = virological suppression; undetectable (<50 copies/mL) = optimal ART response
- U=U: Undetectable = Untransmittable — HIV-positive person on effective ART with undetectable viral load CANNOT sexually transmit HIV
CD4+ count:
- Absolute count (flow cytometry) — guides OI prophylaxis, ART initiation (though India now starts ART at ANY CD4 count — 'test and treat')
- CD4:CD8 ratio (normal >1; inverted <1 = advanced HIV)
HIV p24 antigen:
- Appears in window period before antibodies — detectable by 4th-gen ELISA
- As viral load rises, p24 is consumed by antibody → may become negative at seroconversion
Nucleic Acid Testing (NAT/PCR):
- HIV RNA detection — earliest window (10–12 days)
- Mandatory for blood bank screening in India (since 2014 at major blood banks)
- Qualitative PCR used for early infant diagnosis (EID) in babies born to HIV-positive mothers (below 18 months where maternal antibodies confound ELISA)
SELF-CHECK
A 6-week-old infant is born to an HIV-positive mother who received PMTCT (Prevention of Mother-to-Child Transmission). The standard HIV antibody ELISA is performed and comes back POSITIVE. What is the CORRECT interpretation and next step?
A. The infant is HIV-positive — start ART immediately
B. A positive ELISA at this age reflects MATERNAL antibodies transferred across the placenta; HIV DNA/RNA PCR is required to determine if the infant is truly infected
C. Repeat the ELISA at 12 months — maternal antibody clearance takes exactly 12 months
D. The ELISA is inconclusive — Western blot is the only valid test for infants
Reveal Answer
Answer: B. A positive ELISA at this age reflects MATERNAL antibodies transferred across the placenta; HIV DNA/RNA PCR is required to determine if the infant is truly infected
Maternal IgG antibodies cross the placenta and remain detectable in the infant's blood for up to 18 months — making standard antibody-based ELISA unreliable for diagnosing HIV in infants below 18 months. A positive ELISA in this age group reflects maternal antibodies, NOT infant infection. HIV DNA PCR (qualitative) is the test of choice for Early Infant Diagnosis (EID) — it detects the viral genome regardless of antibody status. First EID test: at 6 weeks of age (or at birth for high-risk infants). A positive PCR confirms infant HIV infection and ART should be started promptly.
Prevention, HAART & National Programme
CD4+ Count Thresholds for Opportunistic Infections in HIV
Principles of HIV prevention:
- Primary prevention: ABC — Abstinence, Be faithful, Condom use; harm reduction (needle exchange for IDUs); blood safety (mandatory HIV testing of all donations)
- Pre-Exposure Prophylaxis (PrEP): Tenofovir-emtricitabine (TDF-FTC) daily for high-risk seronegative individuals; reduces transmission by >90% with good adherence
- Post-Exposure Prophylaxis (PEP): TDF + 3TC + dolutegravir (or lopinavir/ritonavir) × 28 days; must be started within 72 hours of exposure
- PMTCT (Prevention of Mother-to-Child Transmission): Universal antenatal HIV testing; ART for all HIV-positive pregnant women; infant prophylaxis with nevirapine (NVP) for 6 weeks; avoidance of breastfeeding OR exclusive breastfeeding + maternal ART
HAART (Highly Active Antiretroviral Therapy) — principles:
- Goal: viral suppression to undetectable → immune reconstitution → near-normal life expectancy
- 'Test and treat' policy (India, 2017): ALL HIV-positive individuals, regardless of CD4 count, should start ART
- First-line regimen (India, NACO): TDF + 3TC (or FTC) + dolutegravir (DTG) — a once-daily fixed-dose combination
Drug classes and targets:
| Class | Examples | Mechanism |
|---|---|---|
| NRTI (Nucleoside RT Inhibitors) | TDF, 3TC, zidovudine (ZDV/AZT), abacavir | False substrate for RT — chain termination |
| NNRTI (Non-nucleoside RT Inhibitors) | Efavirenz, nevirapine | Bind RT allosterically |
| PI (Protease Inhibitors) | Lopinavir/ritonavir | Block viral protease → immature virions |
| INSTI (Integrase Inhibitors) | Dolutegravir, raltegravir | Block integrase → proviral DNA not inserted |
| Entry/Fusion Inhibitors | Maraviroc (CCR5 antagonist), enfuvirtide | Block co-receptor binding or gp41 fusion |
Monitoring on ART:
- Viral load: 6 months after starting ART, then annually (target: undetectable)
- CD4+ count: annually (guides OI prophylaxis)
- Routine: LFT, RFT, CBC, blood glucose (monitor for drug toxicities)
National AIDS Control Programme (NACP), India:
- NACP-IV running 2012–2017 (NACP-V ongoing)
- NACO (National AIDS Control Organisation) — apex body
- ICTC (Integrated Counselling and Testing Centres) — free, confidential HIV testing with pre- and post-test counselling nationwide
- Free ART at ART Centres in every district hospital
- 90-90-90 UNAIDS target → 95-95-95 by 2025: 95% of PLHIV know their status, 95% on treatment, 95% virally suppressed
SELF-CHECK
A person presents with headache and fever for 3 weeks. CSF analysis: opening pressure high, clear fluid, glucose low, protein elevated. India ink staining reveals round organisms with a wide, refractile capsule. CD4+ count is 92 cells/μL. What is the MOST likely diagnosis and the MOST appropriate confirmatory test?
A. Toxoplasma encephalitis — CT brain with ring-enhancing lesions confirms
B. Cryptococcal meningitis — CrAg (cryptococcal antigen) latex agglutination or LFA is most rapid and sensitive
C. Bacterial meningitis — Gram stain and culture of CSF
D. PCP — GMS staining of BAL fluid confirms
Reveal Answer
Answer: B. Cryptococcal meningitis — CrAg (cryptococcal antigen) latex agglutination or LFA is most rapid and sensitive
India ink staining demonstrating encapsulated yeasts with a wide refractile capsule in CSF is characteristic of Cryptococcus neoformans. Cryptococcal meningitis typically occurs when CD4+ is <100 cells/μL. The CrAg (cryptococcal antigen) test — by latex agglutination or lateral flow assay (LFA) — is more sensitive than India ink (nearly 100% in active disease) and is the recommended confirmatory and screening test. CSF culture on Sabouraud agar also confirms (but takes days). Treatment: amphotericin B + flucytosine induction → fluconazole maintenance.