Page 1 of 13
MI3.10-12 | Malaria & Blood Parasites (incl. Peripheral Smear) — SDL Guide
Learning Objectives
- Describe the morphology, life cycle, pathogenesis, laboratory diagnosis, prevention and control of common parasites causing anaemia
- Describe the morphology, life cycle, pathogenesis, clinical presentation, laboratory diagnosis, and prevention of haemoparasites common in India — including malaria, kala-azar, and filariasis
- Differentiate malignant (P. falciparum) from benign (P. vivax, P. ovale, P. malariae) malaria on peripheral blood smear examination and serology, and explain clinical significance
INSTRUCTIONS
Malaria kills one child every two minutes worldwide, and India contributes significantly to this burden. The peripheral blood smear is the definitive diagnostic tool — and reading it is a skill you must master. This session integrates parasite morphology, life cycle, and clinical features into a unified framework, culminating in the practical skill of smear interpretation.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 54 (Plasmodium), Ch 56 (Leishmania), Ch 60 (Filarial worms) (textbook)
- Harrison's Principles of Internal Medicine — Malaria, Leishmaniasis, Lymphatic Filariasis (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients arrive in the same Indian district hospital on a monsoon morning:
Patient A: 28-year-old farmer, 3 days of fever with chills every 48 hours, mild splenomegaly, Hb 10.2 g/dL. Peripheral smear: enlarged RBCs with Schüffner's dots; ameboid trophozoites inside cells.
Patient B: 7-year-old child, 4 days of continuous high fever, confusion, Hb 6.2 g/dL. Peripheral smear: normal-sized RBCs, multiple ring forms per cell, 'appliqué' (accolé) forms at the RBC edge; banana-shaped gametocytes.
Patient A gets chloroquine and is discharged. Patient B is admitted to ICU, started on IV artesunate. One lived; the other survived only because a blood smear distinguished them.
You will be the person reading that smear — or supervising the reading. Today you learn how.
WHY THIS MATTERS
India reported approximately 3.6 million malaria cases and 1,800 deaths in 2022 — and these are gross underestimates from passive surveillance. P. falciparum accounts for about 50% of cases and nearly all deaths. Kala-azar (visceral leishmaniasis) is endemic in Bihar, Jharkhand, and West Bengal. Filariasis affects 650 million people globally, with India bearing 40% of the lymphatic filariasis burden. These are not exotic diseases — they will walk into your outpatient clinic. Smear reading and clinical recognition will be daily skills.
RECALL
Before proceeding, recall:
- Protozoa = unicellular eukaryotes (Plasmodium, Leishmania); Helminths = multicellular worms (Wuchereria)
- Schüffner's dots — intracellular stippling in RBCs; Maurer's clefts — irregular, fewer spots
- Anopheles mosquito = malaria vector; Phlebotomus sandfly = kala-azar vector; Culex mosquito = filariasis vector
- Reticuloendothelial system — liver, spleen, bone marrow macrophages; critical for both malaria pathogenesis and kala-azar tissue tropism
Malaria: Causative Agents & Life Cycle
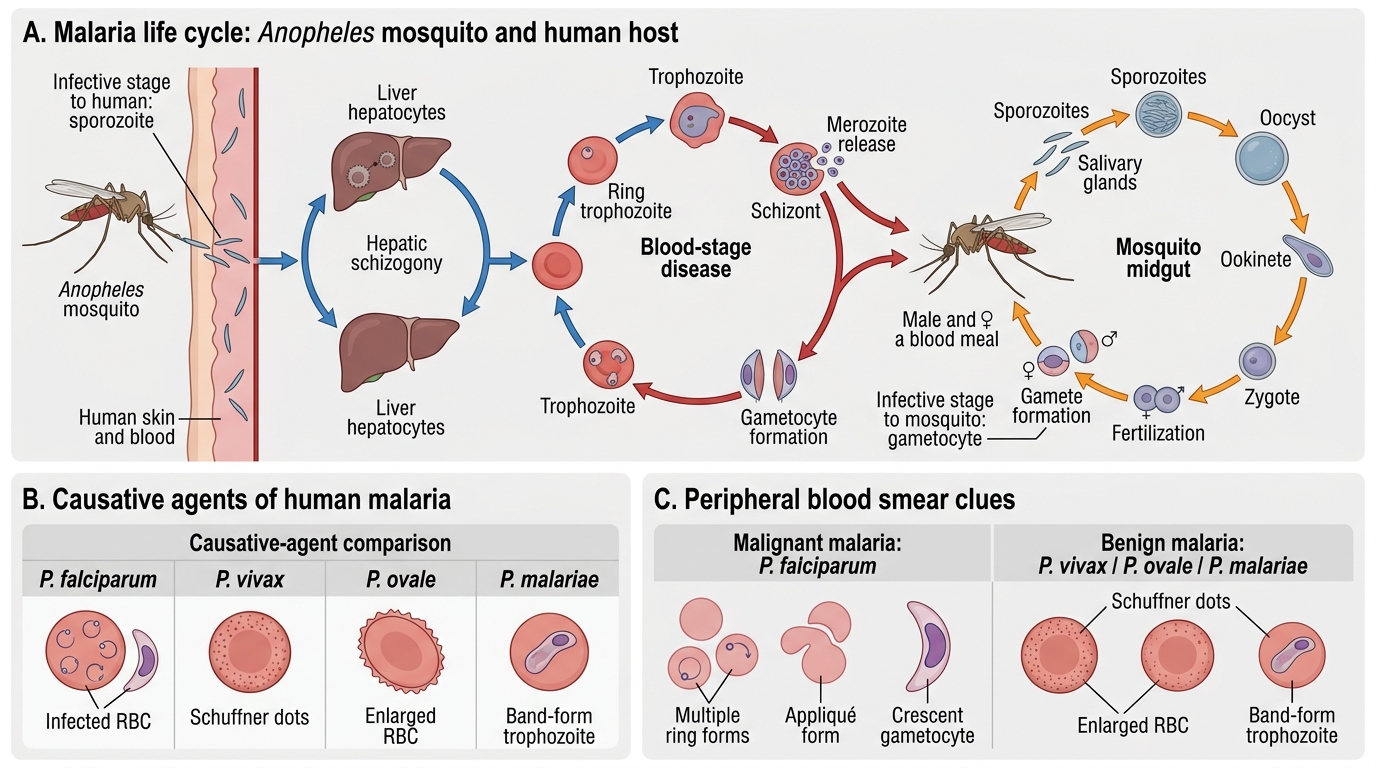
Malaria: Causative Agents and Life Cycle
Four species of Plasmodium infect humans:
| Species | Fever periodicity | RBCs infected | Severity |
|---|---|---|---|
| P. falciparum | Tertian (48 hr; irregular) | All ages | Malignant — life-threatening |
| P. vivax | Tertian (48 hr) | Reticulocytes only | Benign tertian |
| P. ovale | Tertian (48 hr) | Reticulocytes only | Benign tertian (mild) |
| P. malariae | Quartan (72 hr) | Senescent RBCs | Benign quartan |
Life cycle — two hosts:
In the mosquito (sexual cycle — sporogony):
- Anopheles female ingests gametocytes during blood meal
- Gametocytes → gametes → zygote → ookinete → oocyst → sporozoites in salivary gland
- Sporozoites = infective form for humans
In the human (asexual cycle — schizogony):
Exo-erythrocytic (hepatic) phase:
1. Sporozoites injected → travel to liver → infect hepatocytes
2. Liver schizogony → hepatic schizonts → merozoites released (5–16 days)
3. P. vivax and P. ovale: form hypnozoites (dormant liver forms) → responsible for relapse months to years later
Erythrocytic phase:
1. Merozoites invade RBCs → trophozoites (ring stage) → schizonts → merozoite burst (rupturing of RBC) → cyclical fever
2. Some merozoites → gametocytes (sexual forms) → ingested by mosquito → continue cycle

Malaria Life Cycle in Humans
Malaria Pathogenesis & Clinical Features
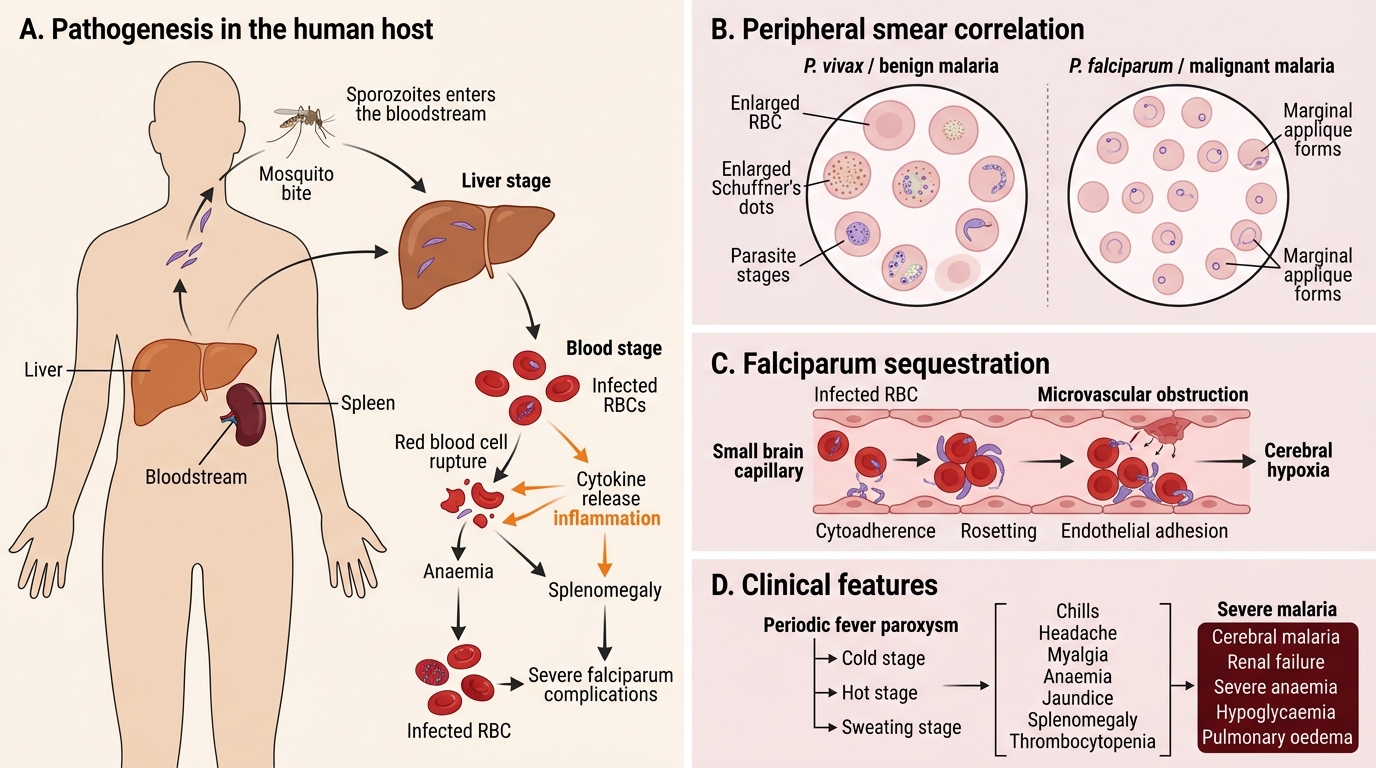
Malaria Pathogenesis and Clinical Features
Mechanism of fever:
RBC rupture → merozoite burst → release of malaria pigment (haemozoin) + merozoites into bloodstream → stimulate macrophages → release TNF-α, IL-1, IL-6 → hypothalamic fever
- Periodicity: tertian (P. falciparum, P. vivax, P. ovale) = 48-hour cycle; quartan (P. malariae) = 72-hour cycle
Classic malaria paroxysm (cold-hot-sweating triad):
1. Cold stage (30–60 min) — rigors, shivering, vasoconstriction
2. Hot stage (2–6 hr) — high fever (40–41°C), headache, nausea, vomiting
3. Sweating stage (2–4 hr) — profuse sweating, rapid defervescence, fatigue
Why P. falciparum is malignant:
1. Cytoadherence — infected RBCs express PfEMP1 (P. falciparum erythrocyte membrane protein 1) on their surface → cytoadhere to endothelial cells via ICAM-1, CD36 → microvascular occlusion → sequestration
2. Rosetting — infected RBCs clump with uninfected RBCs → further impedes circulation
3. High parasitaemia — infects all RBC ages (not just reticulocytes) → 10–30% of RBCs can be parasitised
4. Cerebral malaria — sequestration in cerebral microvasculature → coma, seizures, death
Complications of P. falciparum malaria (WHO severe malaria criteria):
- Cerebral malaria (unarousable coma)
- Severe anaemia (Hb <7 g/dL)
- Respiratory distress (acidotic breathing)
- Blackwater fever (massive haemolysis → haemoglobinuria → dark urine → renal failure)
- Hypoglycaemia (glucose consumption by parasites + quinine-induced hyperinsulinaemia)
- Multi-organ failure
Relapse vs recrudescence:
- Relapse (P. vivax, P. ovale): hypnozoites reactivate months/years after primary infection — treated with primaquine
- Recrudescence (P. falciparum, P. malariae): persistent low-level erythrocytic parasitaemia resurges — due to incomplete treatment, NOT hypnozoites
CLINICAL PEARL
Glucose-6-Phosphate Dehydrogenase (G6PD) deficiency — the primaquine trap:
Primaquine is the only drug that eliminates P. vivax/ovale hypnozoites (radical cure). However, primaquine causes haemolytic anaemia in G6PD-deficient patients (common in India, especially males). Always test for G6PD deficiency BEFORE prescribing primaquine. G6PD-deficient patients can still be treated for acute malaria with chloroquine — only the radical cure needs modification (weekly primaquine under supervision or an alternative).
Peripheral Smear Interpretation: Falciparum vs Benign Malaria
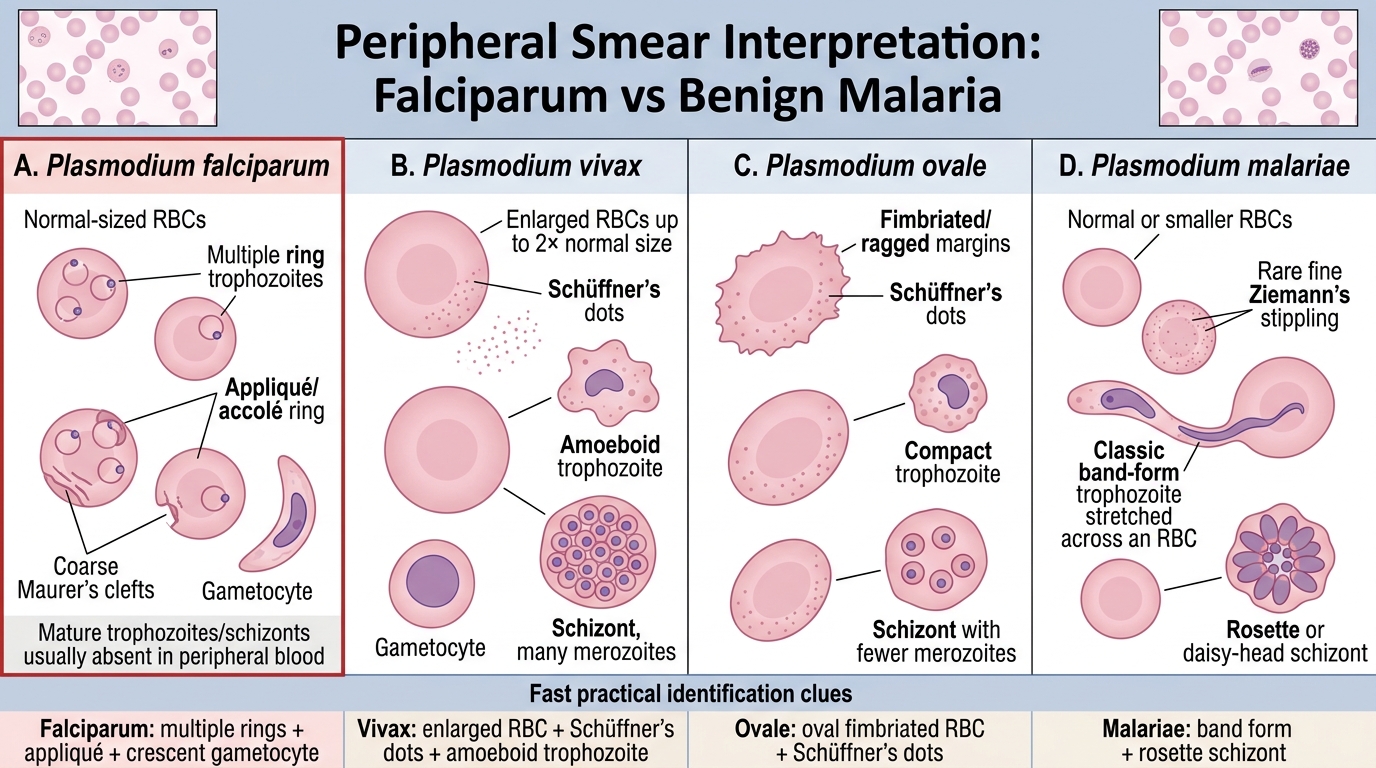
Peripheral Smear Clues in Malaria Species
This is the most examined practical skill in malaria microbiology. Learn the differences by smear feature:
| Feature | P. falciparum | P. vivax | P. ovale | P. malariae |
|---|---|---|---|---|
| RBC size | Normal (not enlarged) | Enlarged (up to 2×) | Slightly enlarged, oval/fimbriated | Normal or smaller |
| Stippling | Maurer's clefts (coarse, 1–2 per cell; not always visible on routine stain) | Schüffner's dots (fine pink stippling, many per cell) | Schüffner's dots | Ziemann's stippling (rarely seen) |
| Rings (trophozoite) | Multiple rings per cell (often 2–3); appliqué/accolé forms (ring pressed against RBC membrane) | One large ring per cell; ameboid, irregular shape by late trophozoite | One ring per cell; compact | One ring per cell; compact |
| Gametocytes | Banana/crescent-shaped (pathognomonic) | Round/oval | Round | Round |
| Stage seen in peripheral blood | Only rings and gametocytes (mature forms sequestered in vessels) | All stages visible | All stages visible | All stages visible |
| Parasitaemia level | Can be >5% (heavy) | Usually <2% | Low | Very low |
Critical distinguishing points for examinations:
- Banana-shaped gametocyte = P. falciparum — no other Plasmodium has this
- Multiple rings per RBC + normal RBC size = P. falciparum (vs. P. vivax which shows single ring in enlarged RBC)
- Schüffner's dots = P. vivax or P. ovale (not P. falciparum)
- Only rings seen on smear (no trophozoites/schizonts) = P. falciparum sequestration phenomenon
- Appliqué form = ring lying flat against inner RBC membrane = P. falciparum
Smear preparation:
- Thick smear: concentrated layer of RBCs (more sensitive, detects low parasitaemia); cells lyse, so only WBCs and parasite elements visible — used for screening
- Thin smear: monolayer of RBCs; species-level morphology; used for identification after thick smear positivity
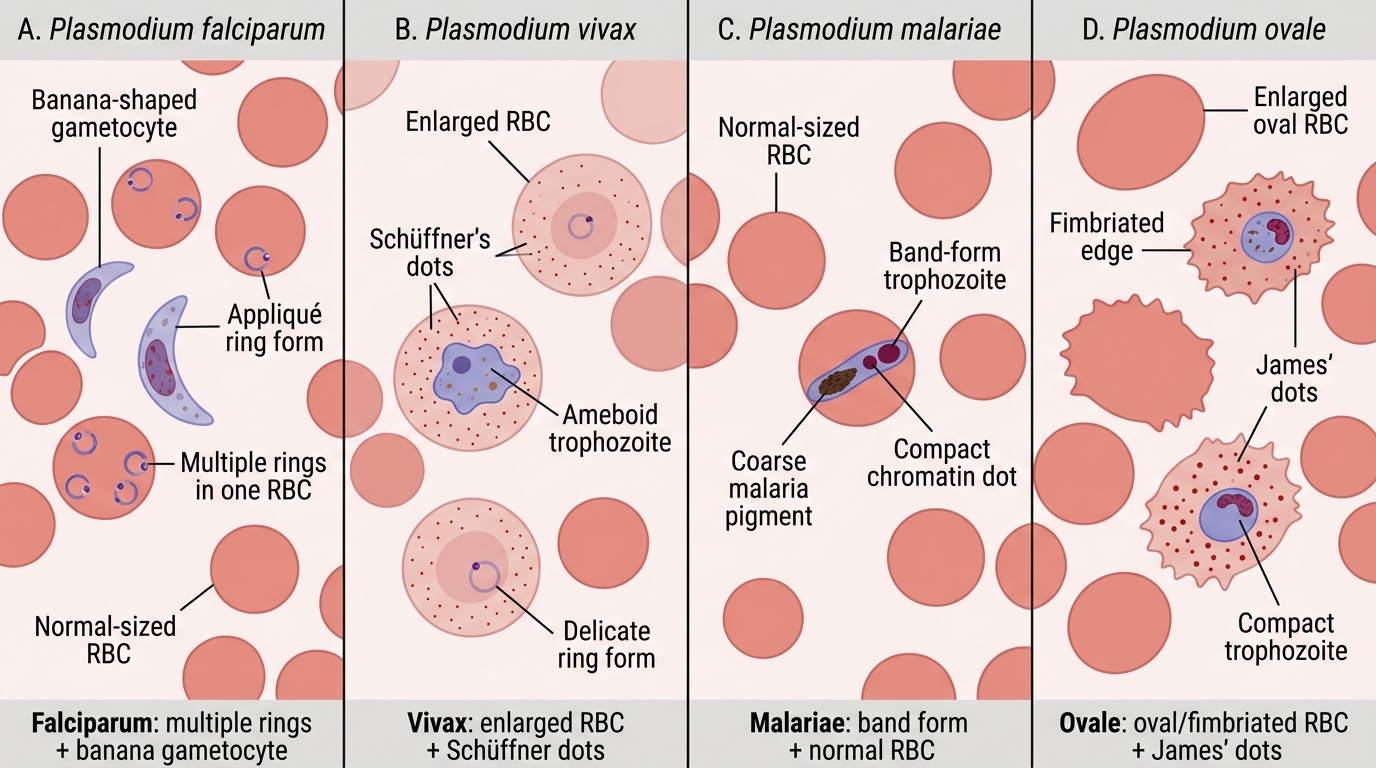
Peripheral Smear Features of Major Malarial Parasites
SELF-CHECK
A peripheral blood smear shows RBCs with multiple ring forms per cell, some rings pressed against the inner RBC membrane (appliqué position), and banana-shaped gametocytes. The infected RBCs appear normal in size. What species does this smear represent, and why is immediate treatment critical?
A. P. vivax — Schüffner's dots confirm benign malaria; chloroquine adequate
B. P. falciparum — banana gametocytes and appliqué forms confirm malignant malaria; IV artesunate needed if severe
C. P. malariae — quartan fever; only Ziemann's stippling visible
D. P. ovale — oval RBCs confirm diagnosis; radical cure with primaquine required
Reveal Answer
Answer: B. P. falciparum — banana gametocytes and appliqué forms confirm malignant malaria; IV artesunate needed if severe
The combination of banana-shaped (crescent) gametocytes, multiple rings per RBC, appliqué/accolé forms, and normal-sized RBCs is pathognomonic for P. falciparum (malignant malaria). Immediate treatment with artemisinin-based combination therapy (ACT) — or IV artesunate if severe — is critical because P. falciparum can progress to cerebral malaria, severe anaemia, and multi-organ failure within hours. P. vivax shows Schüffner's dots in enlarged RBCs; P. ovale shows oval/fimbriated RBCs; P. malariae has normal-sized RBCs with band-form trophozoites.