Page 2 of 13
MI3.10-12 | Malaria & Blood Parasites (incl. Peripheral Smear) — SDL Guide (Part 2)
Laboratory Diagnosis, Prevention & Control of Malaria
Laboratory Diagnosis, Prevention and Control of Malaria
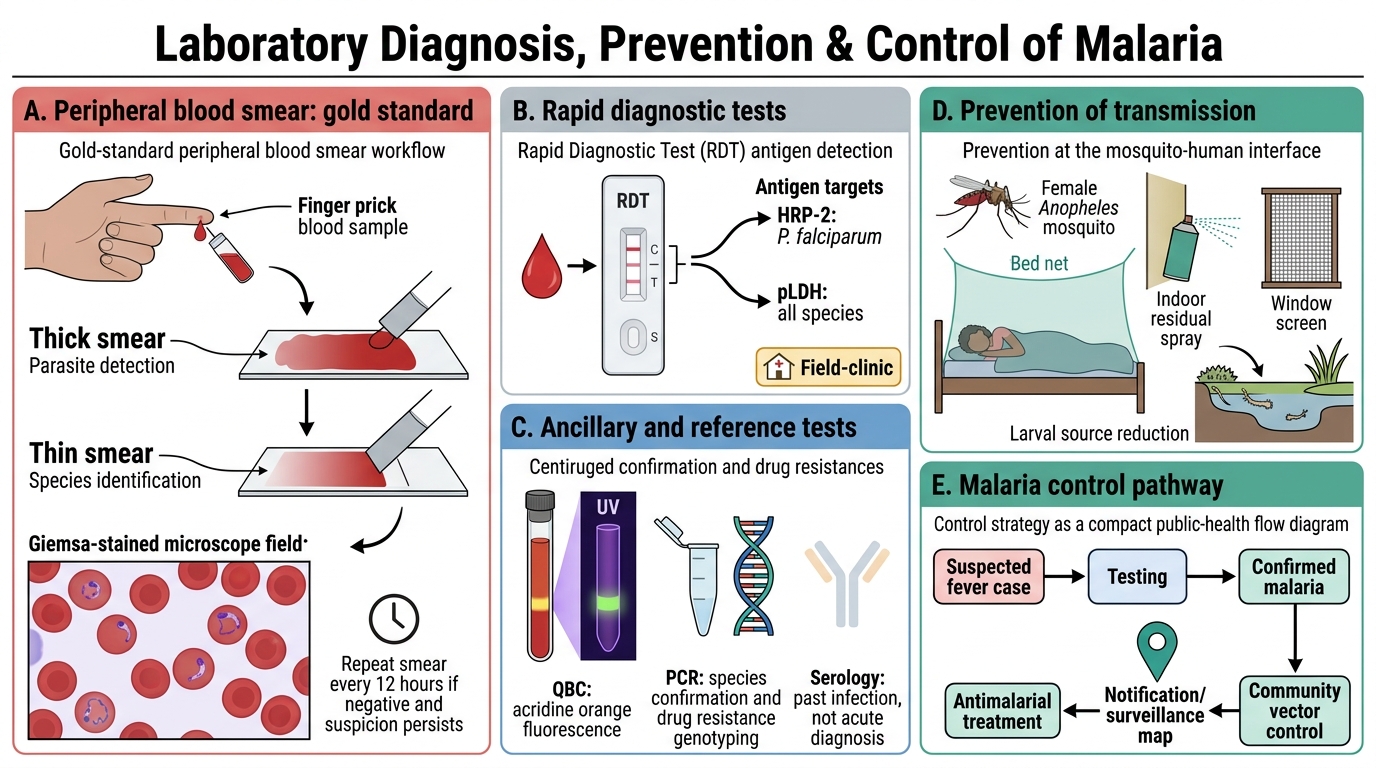
Laboratory diagnosis:
- Peripheral blood smear (gold standard): Thick + thin films, Giemsa stain (or Leishman's); repeat at 12-hour intervals if first smear is negative (parasitaemia may be low)
- Rapid Diagnostic Tests (RDTs): Antigen detection (HRP-2 for P. falciparum; pLDH for all species); useful in field settings; cannot distinguish species in all kits; false negatives with very low parasitaemia
- QBC (Quantitative Buffy Coat): Acridine orange fluorescence on centrifuged blood; sensitive, quantitative
- PCR: Reference standard for species confirmation and drug resistance genotyping; not routine
- Serology (IFA, ELISA): Evidence of past infection; not useful for diagnosis of acute malaria
Prevention and control:
- Vector control: Insecticide-treated bed nets (ITNs), indoor residual spraying (IRS) with pyrethroid or DDT
- Larval control: Elimination of stagnant water breeding sites; larviciding with Bacillus thuringiensis israelensis (Bti)
- Chemoprophylaxis for travellers: Chloroquine (P. vivax endemic areas), atovaquone-proguanil, doxycycline, or mefloquine (P. falciparum endemic or MDR areas)
- Radical cure: Primaquine after chloroquine for P. vivax/ovale (after G6PD testing)
- National programme: National Vector Borne Disease Control Programme (NVBDCP) in India
- Vaccine: RTS,S (Mosquirix) — first licensed malaria vaccine; partial protection against P. falciparum; recommended by WHO for sub-Saharan Africa (2021)
Other Haemoparasites: Kala-azar & Filariasis
Kala-azar and Filariasis: Diagnosis, Prevention and Control
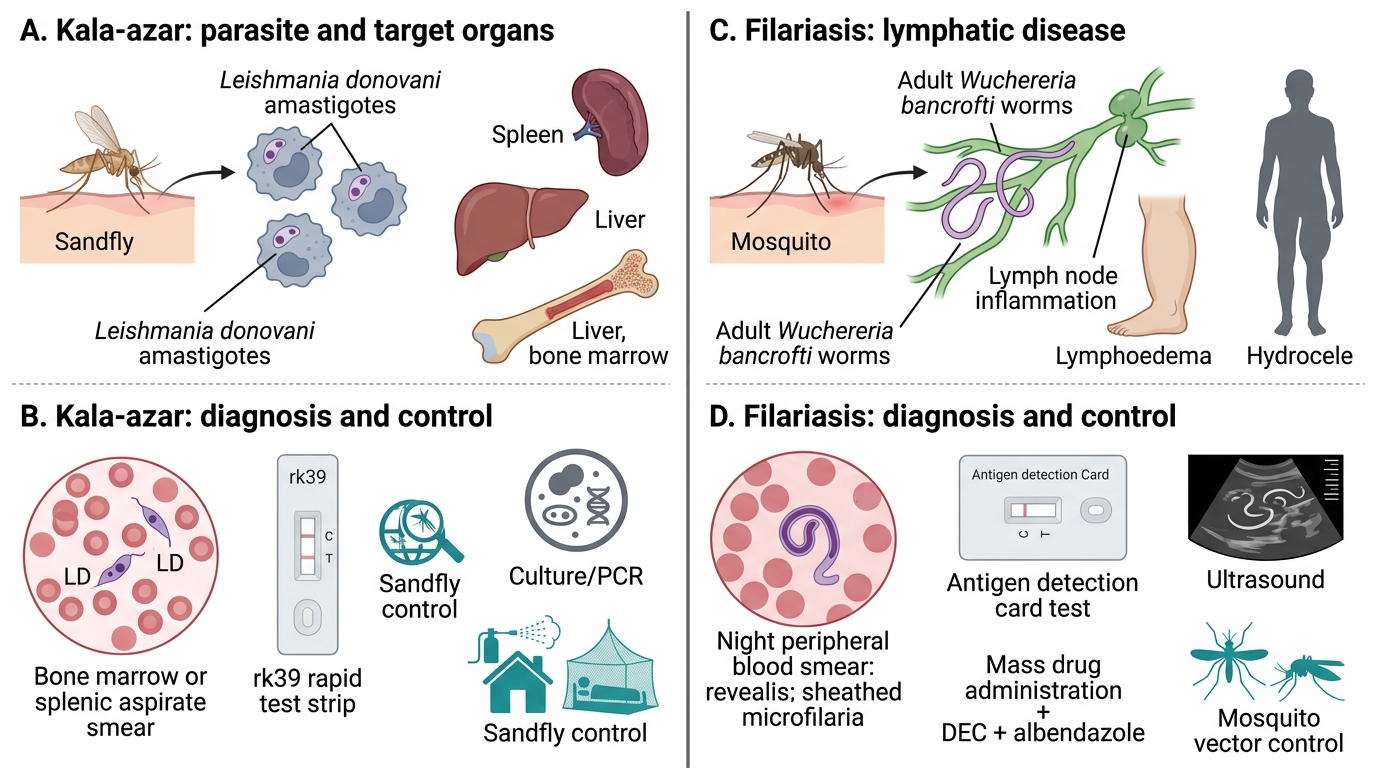
Visceral Leishmaniasis (Kala-azar) — Leishmania donovani:
Morphology:
- Amastigote (Leishman-Donovan/LD body): intracellular, oval, 2–4 μm; found in macrophages of bone marrow, spleen, liver
- Promastigote: extracellular, flagellated; present in sandfly gut and culture
Transmission: Female Phlebotomus argentipes sandfly (India — Bihar, Jharkhand, West Bengal, UP); bites at night; breeds in moist, sandy soil
Pathogenesis: Promastigotes injected → phagocytosed by macrophages → transform to amastigotes → replicate intracellularly (evade phagolysosome via LPG surface coat) → disseminate to RE system
Clinical features: Prolonged fever (>2 weeks), massive splenomegaly, hepatomegaly, progressive weight loss, darkening of skin (kala-azar = 'black sickness' in Hindi), anaemia, pancytopenia
Laboratory diagnosis:
- Tissue smear: Bone marrow or splenic aspirate — LD bodies in macrophages (gold standard)
- rK39 rapid test: Immunochromatographic strip for anti-rK39 antibody; highly sensitive and specific in India; field-applicable
- Aldehyde (formol-gel) test: Non-specific — elevated globulin; historical but still examined
- Culture: NNN (Novy-MacNeal-Nicolle) agar — promastigotes grow
- PCR: Reference labs; highly sensitive
Treatment: Liposomal amphotericin B (first-line in India, National Kala-azar Elimination Programme); miltefosine (oral); antimonials (sodium stibogluconate) — now second-line due to resistance in Bihar
Lymphatic Filariasis — Wuchereria bancrofti:
Morphology: Microfilariae — sheathed (600–700 μm); nuclei absent in tail tip (distinguishes from Brugia malayi which has nuclei in tail tip)
Transmission: Culex quinquefasciatus mosquito (urban) in India; nocturnal periodicity — microfilariae peak in peripheral blood between 10 PM–2 AM (correlates with Culex peak biting time)
Pathogenesis: Infective L3 larvae → lymphatics → adult worms (live 5–10 years) → lymphatic obstruction → chronic lymphoedema → elephantiasis (of legs, scrotum); adult worms release microfilariae into bloodstream
Laboratory diagnosis:
- Nocturnal blood smear: Collect blood between 10 PM–2 AM; thick film, Giemsa stain — microfilariae identified by sheath + nuclear column morphology
- Knott's concentration technique: 1 mL blood + 9 mL 2% formalin → centrifuge → stain sediment
- Immunochromatographic test (ICT card test): Detects filarial antigen; no need for nocturnal blood sample
- Ultrasound: 'Filarial dance sign' — adult worms moving in dilated lymphatics
Prevention: Annual mass drug administration (MDA) with diethylcarbamazine (DEC) + albendazole (National Filaria Control Programme)
Haematological significance: Tropical pulmonary eosinophilia (TPE) — occult filarial infection with high IgE, eosinophilia, and pulmonary infiltrates — microfilariae absent in blood (trapped in lung)
SELF-CHECK
A patient from Bihar presents with 3 weeks of fever, massive splenomegaly, and progressive weight loss. His bone marrow aspirate stained with Leishman's stain shows oval, 2–3 μm organisms with a nucleus and kinetoplast inside macrophages. Which test is MOST useful for rapid field diagnosis without a microscope?
A. Widal test (tube agglutination)
B. Aldehyde (formol-gel) test
C. rK39 rapid immunochromatographic strip test
D. Nocturnal peripheral blood smear for microfilariae
Reveal Answer
Answer: C. rK39 rapid immunochromatographic strip test
The rK39 strip test detects antibodies against the rK39 antigen of Leishmania donovani and has >95% sensitivity and specificity in the Indian subcontinent. It is rapid, requires no equipment, and is WHO-recommended for field diagnosis of kala-azar. The Widal test is for typhoid; the aldehyde test is non-specific (elevated globulins) and historical; nocturnal blood smear detects filarial microfilariae, not Leishmania. Bone marrow aspirate showing LD bodies is the gold standard but requires a procedure.
SELF-CHECK
A district health worker wants to screen for lymphatic filariasis in a rural Maharashtra population. Blood samples are collected at 11 PM. Which morphological feature on the Giemsa-stained thick film specifically identifies Wuchereria bancrofti microfilariae compared to Brugia malayi?
A. Presence of a sheath around the microfilaria
B. Absence of nuclei in the tail tip of W. bancrofti (vs. nuclei present in B. malayi tail tip)
C. Larger size of W. bancrofti (>800 μm) compared to B. malayi
D. W. bancrofti microfilariae are unsheathed, unlike B. malayi
Reveal Answer
Answer: B. Absence of nuclei in the tail tip of W. bancrofti (vs. nuclei present in B. malayi tail tip)
Both W. bancrofti and B. malayi microfilariae are sheathed — this feature distinguishes them from unsheathed species (Loa loa is sheathed; Mansonella are unsheathed). The key differentiator between W. bancrofti and B. malayi is the TAIL TIP nuclei: W. bancrofti = no nuclei in tail tip; B. malayi = two distinct nuclei in tail tip. Both are collected on nocturnal blood films (peak at 10 PM–2 AM). W. bancrofti is larger than B. malayi, but this is not the standard diagnostic criterion.