Page 1 of 18
MI4.1-4 | Diarrhoea & Dysentery — SDL Guide
Learning Objectives
- Define and differentiate diarrhoea, dysentery, and food poisoning, listing the major microbial agents for each.
- Describe the epidemiology, morphology, pathogenesis, clinical features, and diagnostic modalities of bacterial, viral, parasitic, and fungal agents causing diarrhoea.
- Describe the epidemiology, morphology, pathogenesis, clinical features, and diagnostic modalities of agents causing dysentery.
- Identify common etiologic agents of diarrhoea and dysentery by stool microscopic examination.
INSTRUCTIONS
Diarrhoeal diseases kill nearly 500,000 children under five every year globally and remain one of the leading causes of morbidity and childhood mortality in India. Understanding the microbial spectrum—from cholera sweeping through flood-affected villages to amoebiasis presenting in a city clinic—is essential for every practicing clinician.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 27–28, 31 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A six-year-old boy from a peri-urban slum presents to casualty with eight episodes of watery stool in 12 hours, severe thirst, sunken eyes, and reduced skin turgor. His mother says three other children in the neighbourhood are similarly ill after attending a community feast the previous evening. What kills fastest here—the pathogen or the dehydration it causes? And how do you tell cholera from rotavirus from Entamoeba just by looking at the stool?
WHY THIS MATTERS
India bears a disproportionate global burden of diarrhoeal illness. In clinical practice you will encounter cholera outbreaks during monsoon floods, rotavirus-driven infant diarrhoea in winter, and amoebic dysentery year-round. The distinction between secretory and invasive diarrhoea—determined largely by the pathogen's mechanism—drives every triage and treatment decision you make.
RECALL
Before proceeding, recall the following from your Phase 1 studies:
- Basic stool examination: macroscopic (colour, consistency, blood/mucus) and microscopic (wet mount, iodine mount, concentration techniques).
- The gastrointestinal mucosa: columnar enterocytes, goblet cells, and the lamina propria.
- Concepts of toxin (exotoxin vs. endotoxin) and their general mechanisms of action.
- Structure of Gram-negative bacterial cell wall (lipopolysaccharide, outer membrane).
Definitions: Diarrhoea, Dysentery, and Food Poisoning
Diarrhoea, Dysentery, and Food Poisoning: Definitions and Key Distinctions
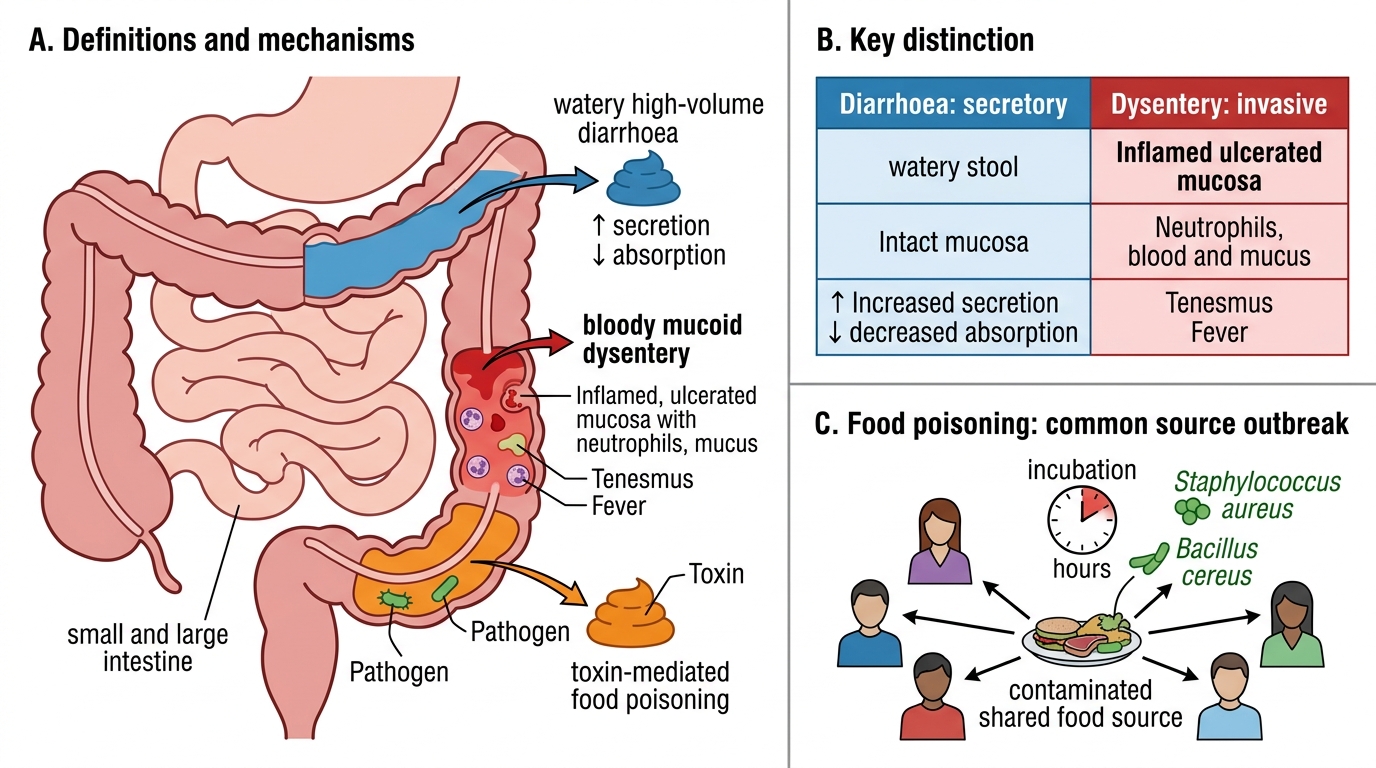
Diarrhoea is defined as the passage of three or more loose or liquid stools per day, or more frequently than is normal for the individual. It reflects increased intestinal water and electrolyte secretion or decreased absorption.
Dysentery is diarrhoea accompanied by blood and mucus in the stool, typically with tenesmus (painful straining) and often fever—indicating mucosal invasion and inflammation.
Food poisoning is illness resulting from ingestion of food contaminated with pathogens or their preformed toxins, characterised by a short incubation period (hours) and often affecting multiple persons from a common source.
Key distinction: diarrhoea is secretory (watery, large-volume, no blood); dysentery is invasive (small-volume, bloody, mucoid).
Major Microbial Agents — Overview
Major Microbial Agents in Diarrhoeal Disease
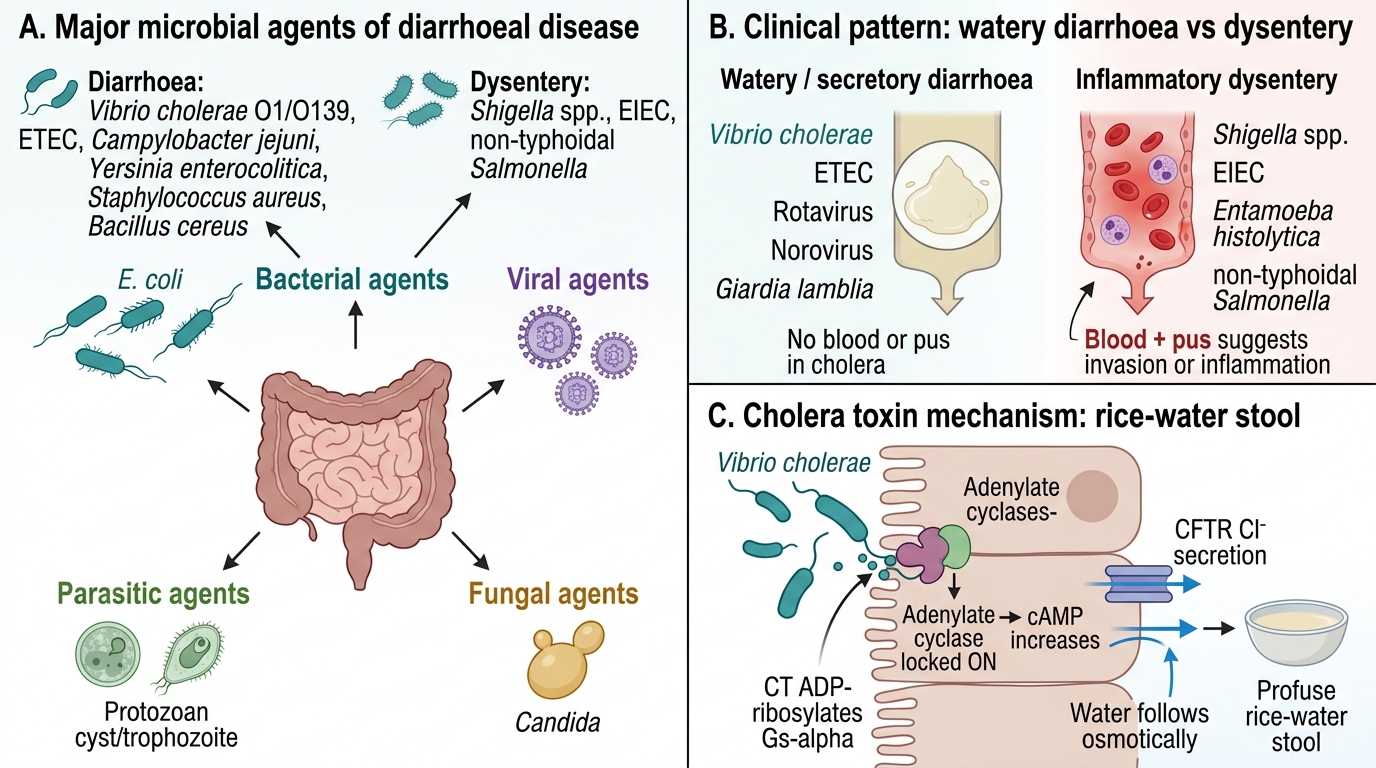
The aetiology of diarrhoeal disease spans all four kingdoms of pathogens:
Bacterial agents of diarrhoea:
- Vibrio cholerae O1/O139 — secretory, rice-water stools
- Enterotoxigenic E. coli (ETEC) — traveller's diarrhoea
- Campylobacter jejuni, Yersinia enterocolitica
- Staphylococcus aureus, Bacillus cereus — preformed toxin, rapid onset
Bacterial agents of dysentery:
- Shigella spp. — the classical cause of bacillary dysentery
- Entero-invasive E. coli (EIEC) — Shigella-like illness
- Salmonella spp. (non-typhoidal) — bloody diarrhoea, bacteraemia risk
Viral agents: Rotavirus (leading cause of infantile diarrhoea in India), Norovirus (outbreaks, all ages), Adenovirus 40/41, Astrovirus
Parasitic agents: Entamoeba histolytica (amoebic dysentery), Giardia lamblia (watery, malabsorptive), Cryptosporidium parvum (immunocompromised), Cyclospora cayetanensis, Balantidium coli
Fungal agents: Rare; Candida in immunocompromised or after heavy antibiotic use
CLINICAL PEARL
Rice-water stool is the hallmark of cholera — profuse, pale, almost odourless, resembling water in which rice has been washed. The mechanism is purely secretory: cholera toxin (CT) ADP-ribosylates Gs-alpha, locking adenylate cyclase in the ON position → massive cAMP → CFTR-mediated Cl⁻ secretion → water follows osmotically. There is no mucosal invasion, so the stool contains no blood or pus cells.
Vibrio cholerae — Pathogenesis & Diagnosis
Vibrio cholerae: Pathogenesis and Diagnosis
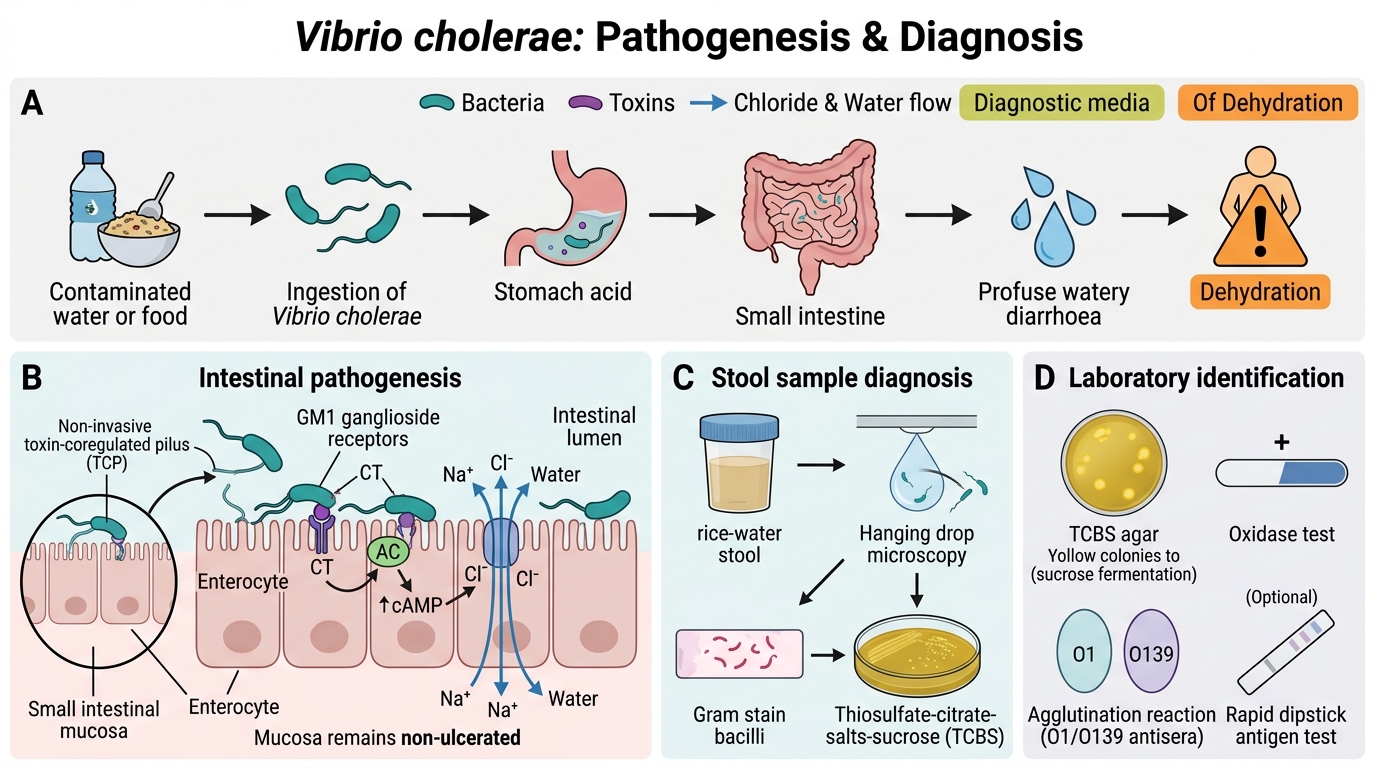
Vibrio cholerae is a comma-shaped, Gram-negative, oxidase-positive, highly motile (single polar flagellum) facultative anaerobe. It grows optimally at alkaline pH (pH 8.5–9) and on thiosulphate–citrate–bile salts–sucrose (TCBS) agar, where it produces yellow colonies.
Pathogenesis steps:
1. Ingestion of contaminated water (infective dose ~10⁸ organisms, reduced in hypochloridria)
2. Colonisation of small intestinal mucosa via TCP (toxin co-regulated pili) and OmpU adhesin
3. Secretion of cholera toxin (CT) — B subunits bind GM1 ganglioside → A subunit enters → ADP-ribosylation of Gs-alpha → ↑cAMP → Cl⁻ efflux + Na⁺ absorption blocked
4. Massive isotonic fluid loss (up to 1 L/hour in severe cases)
Diagnosis:
- Direct microscopy: motile vibrios in wet mount ('shooting star' motility), inhibited by anti-O1 serum (presumptive)
- Culture: TCBS agar (yellow colonies), alkaline peptone water enrichment
- Confirmation: slide agglutination with polyvalent O1/O139 antisera
- Rapid: Dipstick tests (Crystal VC) — field-level use

Vibrio cholerae: Wet Mount Motility and TCBS Culture