Page 2 of 18
MI4.1-4 | Diarrhoea & Dysentery — SDL Guide (Part 2)
Shigella — Bacillary Dysentery
Shigella Bacillary Dysentery: Transmission, Pathogenesis, and Diagnosis
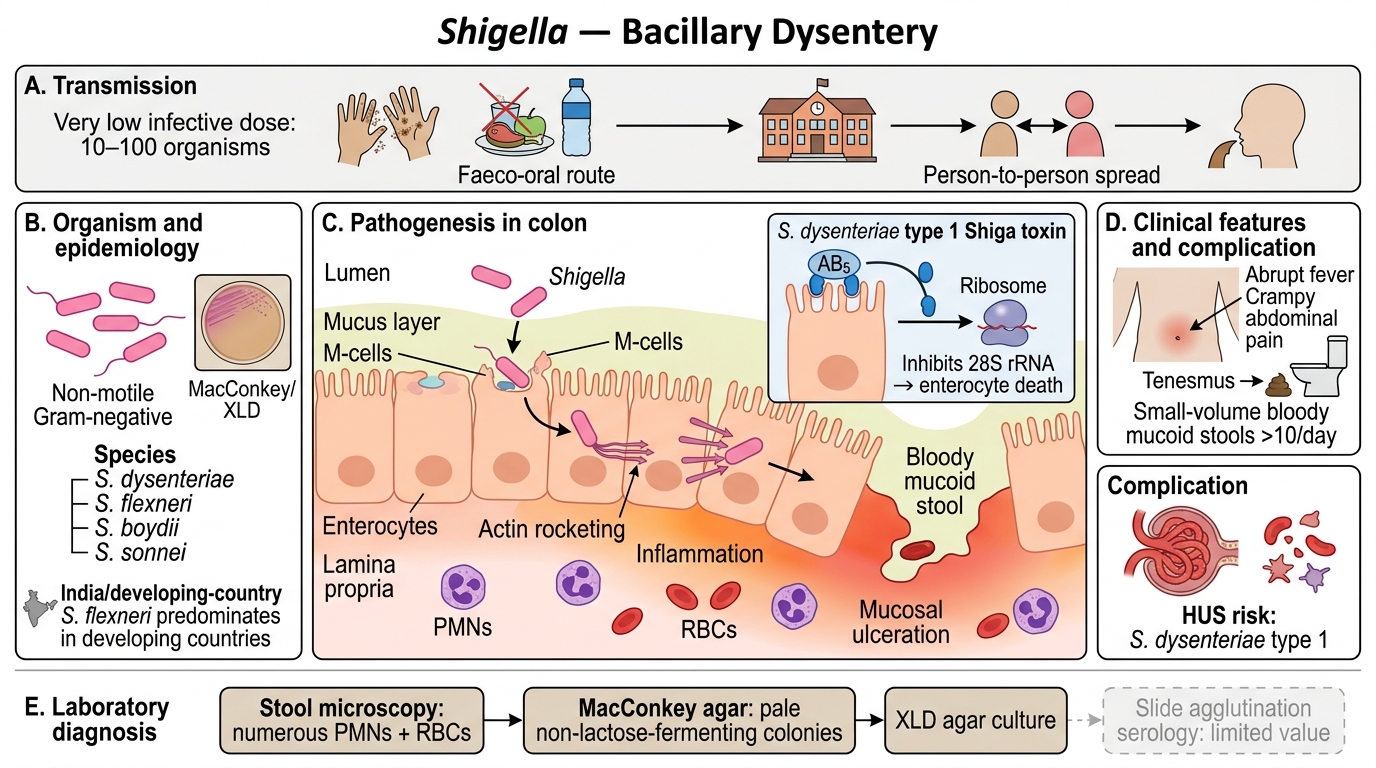
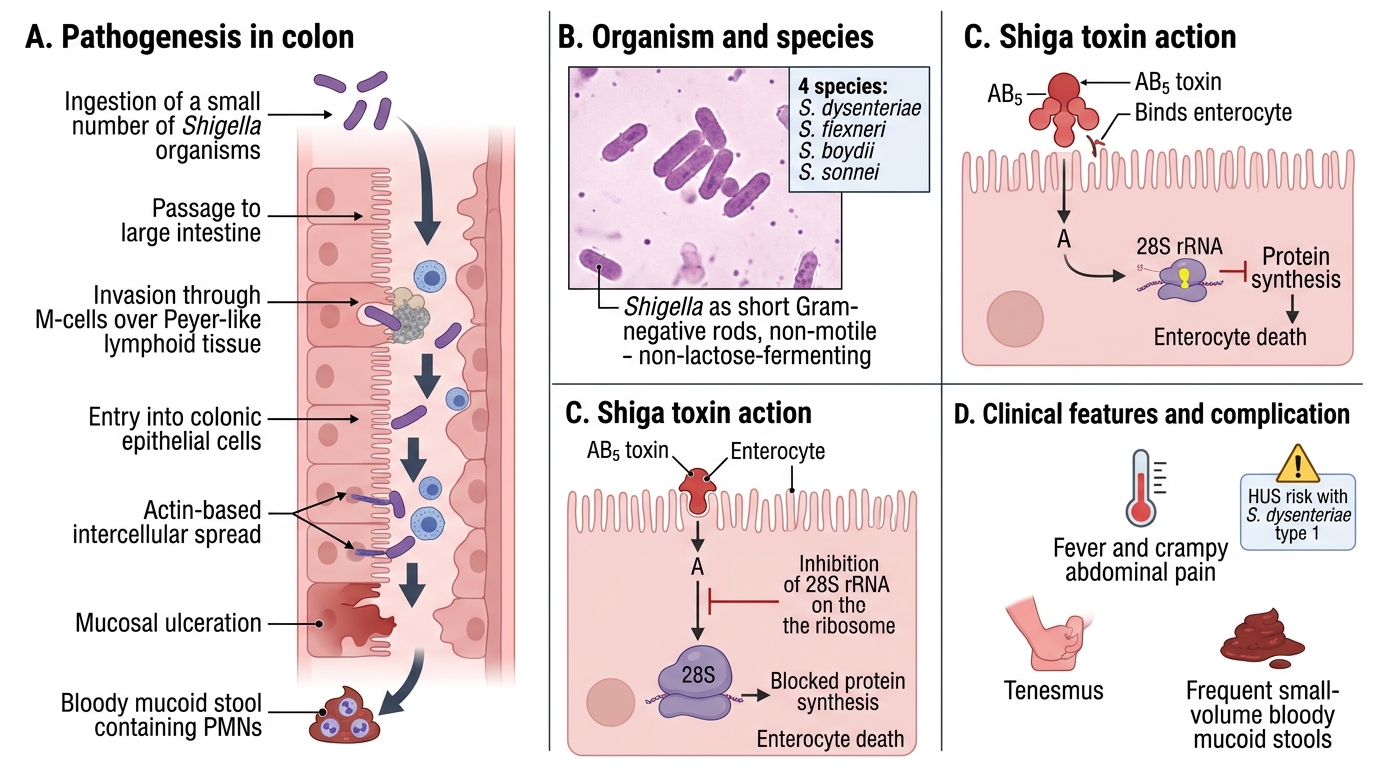
Shigella spp. (four species: S. dysenteriae, S. flexneri, S. boydii, S. sonnei) are non-motile, non-lactose-fermenting Gram-negative rods. S. dysenteriae type 1 produces Shiga toxin (AB5 structure → inhibits 28S rRNA → kills enterocytes).
Pathogenesis:
1. Very low infective dose (~10–100 organisms) — faeco-oral, person-to-person
2. Invasion of colonic epithelium via M-cells → intercellular spread (actin rocketing)
3. Mucosal ulceration → bloody mucoid stool with PMNs
Epidemiology in India: S. flexneri predominates in developing countries; S. sonnei in developed. Outbreaks in schools, crowded institutions.
Clinical features: Abrupt onset fever, crampy abdominal pain, tenesmus, passage of small-volume bloody mucoid stools (>10/day). May progress to HUS with S. dysenteriae type 1.
Diagnosis:
- Stool microscopy: numerous PMNs, RBCs
- Culture: MacConkey agar (non-lactose fermenter, pale colonies), XLD agar
- Serology: Widal-type slide agglutination — limited value
Entamoeba histolytica — Amoebic Dysentery
Entamoeba histolytica: Amoebic Dysentery and Diagnosis
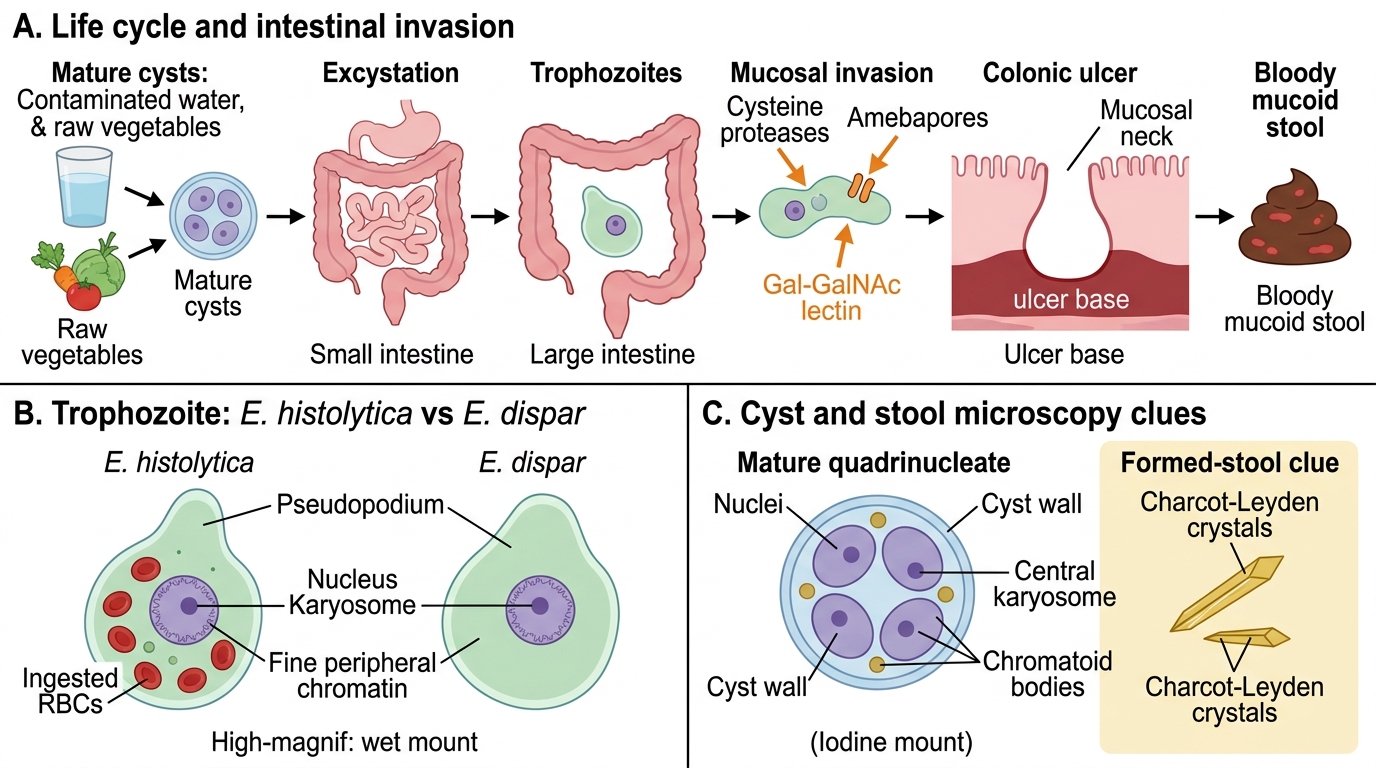
Entamoeba histolytica exists in two forms: the trophozoite (invasive, 20–40 µm, single nucleus with central karyosome) and the cyst (infective, 10–20 µm, 4 nuclei in mature form, chromatoid bodies).
Life cycle: Cysts ingested (contaminated water/raw vegetables) → excystation in small intestine → trophozoites in large intestine → invasion via cysteine proteases (amebapores, Gal/GalNAc lectins) → flask-shaped ulcers in mucosa → bloody mucoid dysentery
Distinction from E. dispar: E. histolytica trophozoites ingest RBCs (erythrophagocytosis) — E. dispar does not. Morphologically identical; differentiate by PCR, antigen EIA, or isoenzyme analysis.
Microscopy (MI4.4):
- Fresh stool (within 30 min): motile trophozoites with ingested RBCs = active invasive amoebiasis
- Cysts in formed stool: iodine mount shows 4 nuclei, chromatoid bars
- Charcot–Leyden crystals (eosinophil membrane fragments) are seen

Stool Microscopy of Protozoal Intestinal Parasites
SELF-CHECK
A 35-year-old woman presents with three weeks of foul-smelling, greasy, non-bloody diarrhoea and significant weight loss after returning from a trek in Uttarakhand. Stool microscopy shows oval cysts with a 'falling-leaf' motility of trophozoites. What is the most likely diagnosis?
A. Entamoeba histolytica infection
B. Giardia lamblia infection
C. Cryptosporidium parvum infection
D. Balantidium coli infection
Reveal Answer
Answer: B. Giardia lamblia infection
Giardia lamblia causes a malabsorptive, non-bloody diarrhoea with fatty, foul-smelling stools ('steatorrhoea') and the characteristic 'falling-leaf' or 'tumbling leaf' motility of trophozoites. Cysts are oval with 4 nuclei and a central axostyle. Entamoeba causes bloody dysentery. Cryptosporidium causes watery diarrhoea, particularly severe in HIV. Balantidium is rare and causes a ciliate-type dysentery.
Viral Diarrhoea — Rotavirus & Others
Shigella Bacillary Dysentery: Pathogenesis and Clinical Correlation
Rotavirus (family Reoviridae) is the single most important cause of severe dehydrating diarrhoea in Indian children under 5 years.
- Structure: Non-enveloped, dsRNA virus with characteristic triple-layered icosahedral capsid ('wheel-like' on EM); 11 RNA segments
- Epidemiology: Winter peak in temperate India; peak age 6 months–2 years; faeco-oral route
- Pathogenesis: Infects villous tip enterocytes of small intestine → NSP4 enterotoxin activates Ca²⁺-mediated Cl⁻ secretion + structural damage → malabsorptive + secretory diarrhoea
- Diagnosis: Antigen ELISA on stool (gold standard for field use); RT-PCR for genotyping; EM ('cartwheel')
- Vaccine: Two oral rotavirus vaccines in India (Rotavac, Rotasiil) — in National Immunization Schedule
Norovirus (Norwalk virus): Non-enveloped, ssRNA (+) virus; calicivirus family. Causes outbreaks in schools, hospitals, cruise ships. Short incubation (24–48 h), projectile vomiting + diarrhoea, self-limiting. Diagnosed by RT-PCR stool.
Adenovirus 40/41: Second most common viral cause in children; year-round; longer duration (~10 days).