Page 5 of 18
MI4.5-6 | Food Poisoning & Acid-Peptic Disease (H. pylori) — SDL Guide
Learning Objectives
- Enumerate bacterial, viral, parasitic, and fungal agents of food poisoning and discuss their pathogenesis, clinical course, and laboratory diagnosis.
- Describe the infective aetiology, pathogenesis, and clinical course of acid-peptic disease (APD), and discuss the laboratory diagnosis and management of its causative agent.
INSTRUCTIONS
Food poisoning and peptic ulcer disease together account for enormous morbidity in India—from banquet-related outbreaks of staphylococcal toxin illness to the near-universal Helicobacter pylori colonisation of adult Indians. Recognising the short incubation pattern of preformed-toxin illness versus the longer incubation of invasive food-borne illness saves lives and guides therapy.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 28, 33 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Fourteen guests at a wedding reception in Chennai all develop violent vomiting and cramping abdominal pain within two hours of eating cream-filled pastries. No fever, no diarrhoea, resolution in six hours. The caterer insists the food was freshly made. What pathogen fits this picture—and does it matter if you culture the food or the patients? Separately, a 45-year-old teacher has been on multiple antacid courses for epigastric burning for five years, with endoscopy showing a prepyloric ulcer. His symptoms return every time he stops medication. What is the definitive treatment that the antacid cannot provide?
WHY THIS MATTERS
India's rapidly expanding food-service industry creates ideal conditions for mass food poisoning outbreaks. Understanding which pathogens produce preformed toxins (rapid onset, no fever, culture-independent diagnosis) versus those that must multiply in vivo (slower onset, fever, requires culture) is critical for outbreak investigation and public health notification. H. pylori, infecting ~60% of Indian adults, is the most important preventable cause of peptic ulcer disease and gastric cancer—making its diagnosis and eradication a core clinical skill.
RECALL
Refresh the following concepts before reading on:
- Normal gastric physiology: parietal cell H⁺/K⁺-ATPase, gastrin, mucus-bicarbonate barrier.
- Exotoxin vs. endotoxin: heat stability, protein vs. LPS, modes of action.
- Basic concepts of urease enzyme activity and ammonia production.
- CLO test principle (colour change from urease activity).
Classification of Food Poisoning
Classification of Food Poisoning
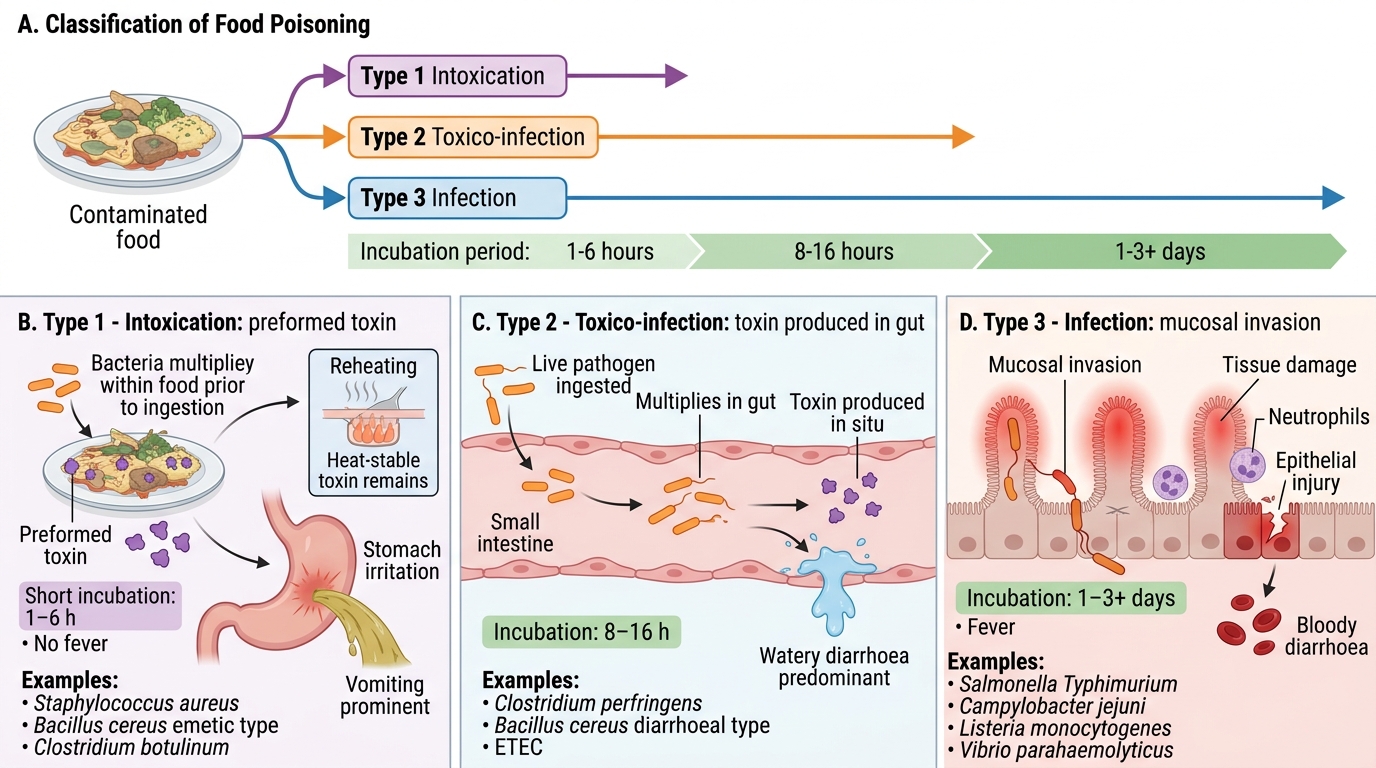
Food poisoning is an illness caused by ingesting contaminated food; it may be:
Type 1 — Intoxication (preformed toxin):
- Pathogen multiplied in food before ingestion, releasing toxin; ingestion of toxin alone causes illness
- Short incubation: 1–6 hours
- No fever (toxin acts, not live pathogen)
- Vomiting prominent
- Examples: Staphylococcus aureus, Bacillus cereus (emetic type), Clostridium botulinum
Type 2 — Toxico-infection (in vivo toxin production):
- Pathogen ingested → multiplies in gut → produces toxin in situ
- Longer incubation: 8–16 hours
- Watery diarrhoea predominant
- Examples: Clostridium perfringens, Bacillus cereus (diarrhoeal type), ETEC
Type 3 — Infection:
- Pathogen invades mucosa; illness due to tissue damage
- Longer incubation: 1–3+ days
- Fever, bloody diarrhoea
- Examples: Salmonella Typhimurium, Campylobacter jejuni, Listeria monocytogenes, Vibrio parahaemolyticus
Staphylococcal Food Poisoning
Staphylococcal Food Poisoning: Heat-Stable Enterotoxin Disease
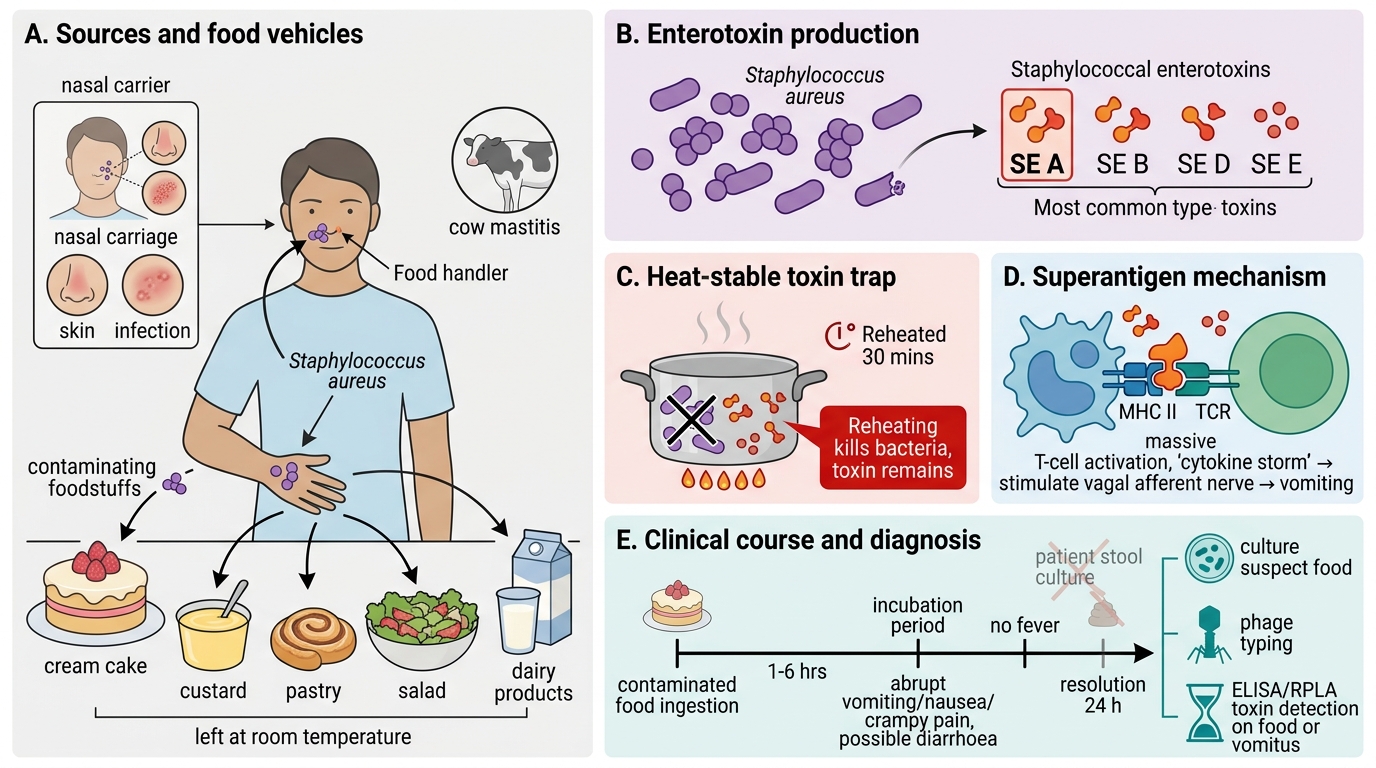
Staphylococcus aureus is the commonest cause of explosive vomiting-type food poisoning worldwide.
Source: Nasal carriers (food handlers), skin infections, mastitis in cows (dairy products). Cream cakes, custards, pastries, salads left at room temperature.
Toxin: Staphylococcal enterotoxins (SE) — SE A to SE E (A most common in outbreaks). Key properties:
- Heat-stable: 100°C for 30 minutes does NOT inactivate them; re-heating kills the organism but the toxin remains
- Super-antigen: binds MHC II outside the antigen-binding groove → massive T-cell activation → cytokine storm → vomiting through vagal afferents
Clinical course: Incubation 1–6 hours. Abrupt vomiting, nausea, crampy pain. Diarrhoea may follow. No fever. Resolution in 24 hours. Rarely fatal (dehydration risk in elderly/infants).
Diagnosis: Culture food (not patient — organism may be absent from stool); phage typing of isolate; SE detection by ELISA or reversed passive latex agglutination (RPLA) on food/vomitus.
CLINICAL PEARL
Heat-stable toxin trap: The most common error in food poisoning outbreak investigation is concluding food is safe because re-heating was done. With S. aureus, re-heating kills all bacteria but leaves SE A fully active. Culture of suspect food may yield no S. aureus (killed by heat) yet toxin is detectable by ELISA. Always test for toxin directly in high-volume/cream food items.
Other Bacterial Food Poisoning Agents
Other Bacterial Food Poisoning Agents
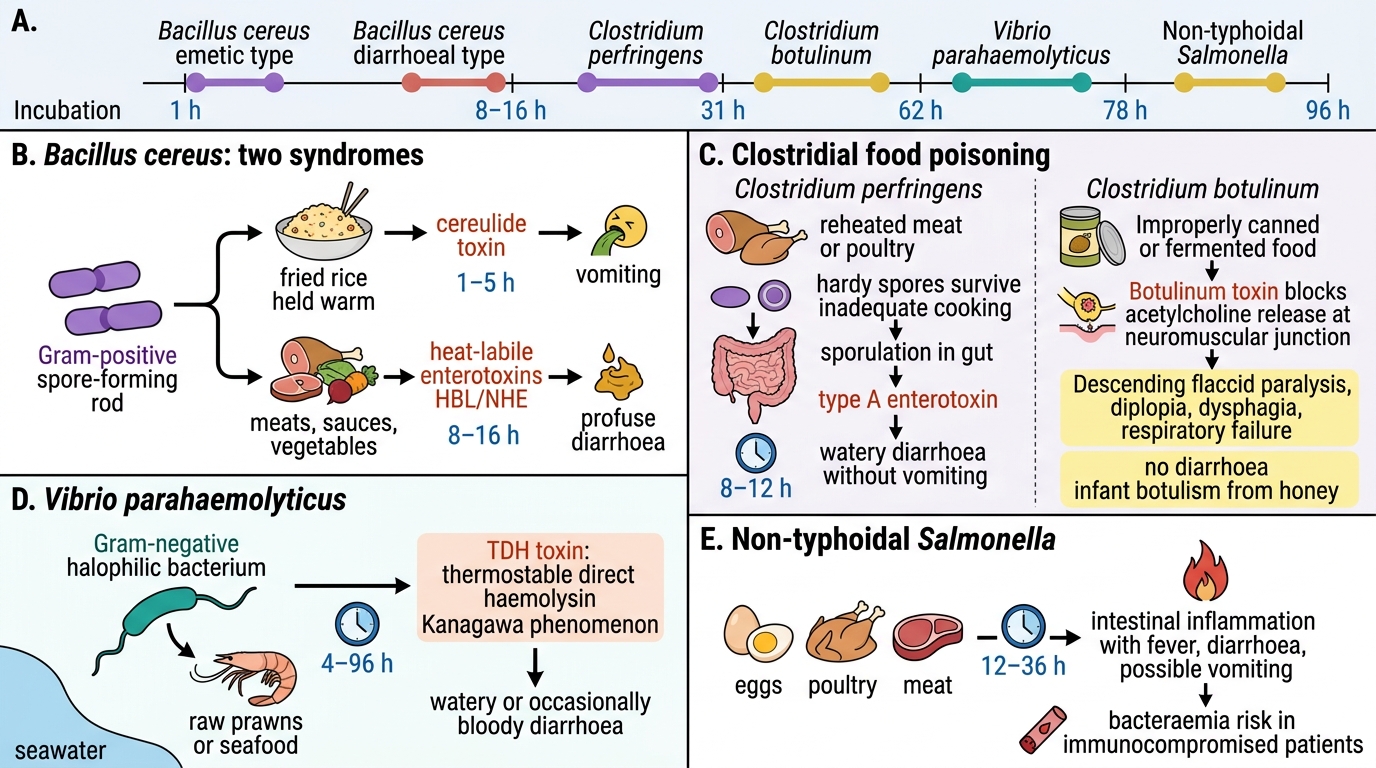
Bacillus cereus — Gram-positive spore-forming rod; two distinct syndromes:
- Emetic type: cereulide (heat-stable cyclic peptide) in fried rice held warm; incubation 1–5 h; vomiting → resembles S. aureus poisoning
- Diarrhoeal type: heat-labile enterotoxin (HBL, NHE) produced in gut; incubation 8–16 h; profuse diarrhoea; implicated foods: meats, sauces, vegetables
Clostridium perfringens — Gram-positive anaerobic spore-former; ingestion of heavily contaminated meat/poultry (>10⁵ organisms); type A enterotoxin produced during sporulation in gut; incubation 8–12 h; watery diarrhoea, no vomiting, self-limiting in 24 h. Hardy spores survive inadequate cooking.
Clostridium botulinum — Produces botulinum toxin (most potent biological toxin; ~1 ng/kg lethal dose); preformed in improperly canned/fermented foods. Toxin blocks Ach release at NMJ → flaccid descending paralysis, diplopia, dysphagia, respiratory failure. No diarrhoea. Diagnosis: mouse inoculation test; toxin ELISA. Infant botulism: honey ingestion → toxin produced in gut.
Vibrio parahaemolyticus — Marine Gram-negative halophile; raw/undercooked seafood (especially prawns); thermostable direct haemolysin (TDH = Kanagawa phenomenon); watery diarrhoea, occasionally bloody; incubation 4–96 h.
Salmonella (non-typhoidal) — S. Typhimurium, Enteritidis; poultry, eggs, meat; 12–36 h incubation; fever + diarrhoea ± vomiting; bacteraemia in immunocompromised.
SELF-CHECK
Four people become ill with vomiting 2 hours after eating reheated fried rice at a canteen. There is no fever and symptoms resolve by evening. Which organism is the most likely cause, and what property of its toxin explains the failure of reheating to prevent illness?
A. Clostridium perfringens — spores survive reheating
B. Bacillus cereus — cereulide is heat-stable and preformed in food
C. Staphylococcus aureus — enterotoxin is heat-stable and preformed in food
D. Salmonella Typhimurium — heat-resistant lipopolysaccharide
Reveal Answer
Answer: B. Bacillus cereus — cereulide is heat-stable and preformed in food
The emetic syndrome of Bacillus cereus is classically linked to fried rice that is cooked and then held warm, allowing spore germination and cereulide production. Cereulide is a heat-stable cyclic peptide that survives reheating at 126°C for 90 minutes. Both S. aureus (option C) and B. cereus emetic type can cause rapid-onset vomiting from preformed heat-stable toxin. In a fried rice context with 2-hour onset, B. cereus (emetic type) is the textbook answer. S. aureus is the classic answer for cream pastries/custards.