Page 8 of 18
MI4.7-9 | Viral Hepatitis — SDL Guide
Learning Objectives
- Describe the epidemiology, etiopathogenesis, clinical features, and complications of viral hepatitis.
- Discuss modalities of laboratory diagnosis with special emphasis on viral markers and preventive strategies for viral hepatitis.
- Suggest the most appropriate laboratory test based on history and clinical presentation in a suspected case of viral hepatitis, and interpret the type and progress of viral hepatitis based on laboratory reports of viral markers.
INSTRUCTIONS
India carries the world's second-largest burden of hepatitis B (approximately 40 million chronically infected individuals) and is hyper-endemic for hepatitis E during monsoon floods. The ability to interpret a hepatitis serology panel—knowing which antibody means immunity, which means active infection, and which means chronicity—is an essential clinical skill that will follow you throughout your career.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 44 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old pregnant woman in her third trimester presents with jaundice, right upper quadrant pain, and dark urine. She lives in a flood-affected village in Bihar and has been drinking municipal tap water for the past month. Her husband, who shares the same water source, is asymptomatic. Three similar cases have arrived in the same week. Is this hepatitis A or E? And why does the answer matter dramatically for this woman—whose maternal mortality risk is 20–25% if it is hepatitis E in the third trimester?
WHY THIS MATTERS
Viral hepatitis spans the spectrum from self-limiting illness (A, E) to chronic infection progressing silently to cirrhosis and hepatocellular carcinoma (B, C, D). India has a dual burden: high faecal-oral transmission (A, E) and significant parenteral transmission (B, C). The hepatitis B vaccine is in India's national immunization schedule—understanding the serology helps you counsel patients about their vaccine status, screen blood donors, and manage the post-exposure prophylaxis pathway.
RECALL
Revisit these concepts before proceeding:
- Basic hepatocyte function: conjugation of bilirubin, albumin synthesis, clotting factor production.
- Difference between direct (conjugated) and indirect (unconjugated) bilirubin.
- Immunoglobulin classes: IgM (acute, early) vs. IgG (late, persistent, memory) responses.
- Concept of seroconversion and virological markers in HIV — the same principles apply to HBV.
Classification of Hepatitis Viruses
Classification of Hepatitis Viruses
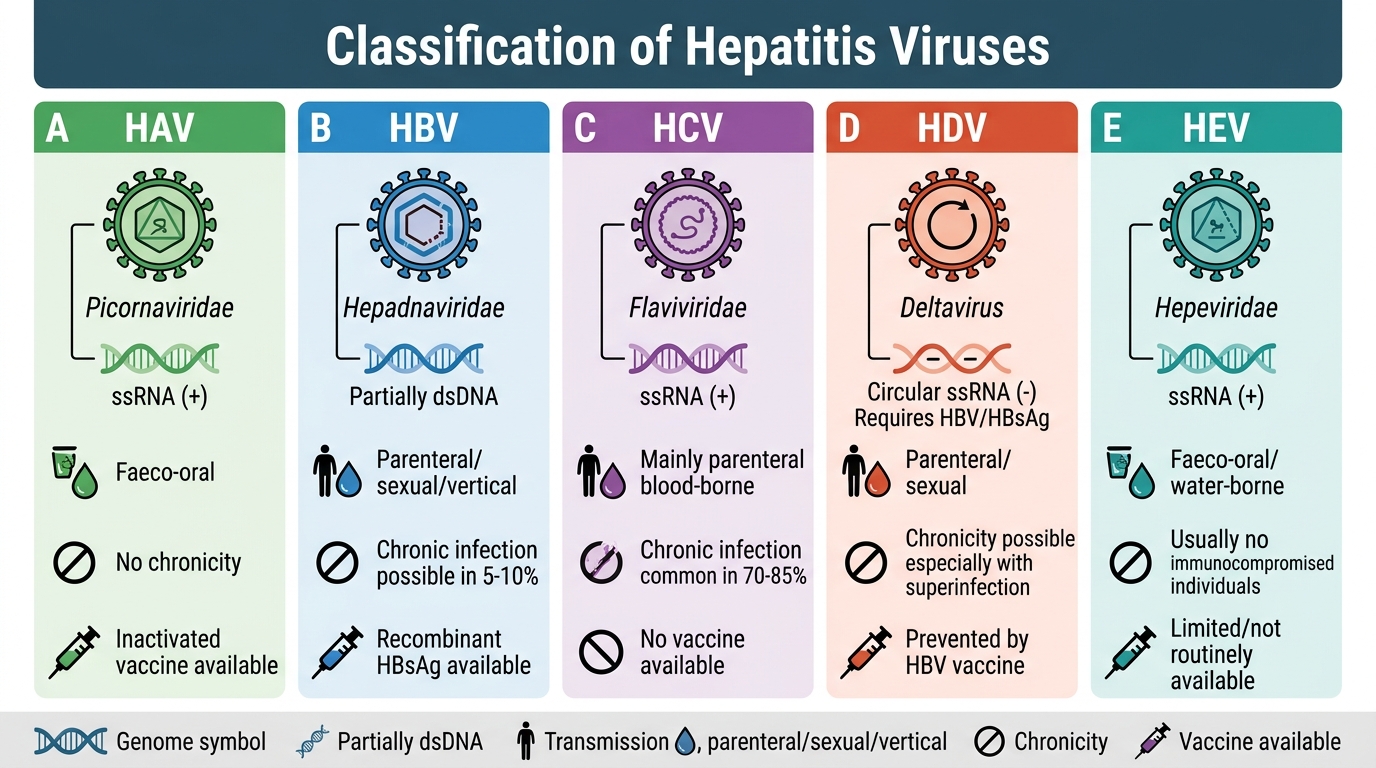
Five distinct viruses cause viral hepatitis; they differ in genome, transmission, and clinical outcome:
| Virus | Family | Genome | Transmission | Chronicity | Vaccine |
|---|---|---|---|---|---|
| HAV | Picornaviridae | ssRNA (+) | Faeco-oral | No | Yes (inactivated) |
| HBV | Hepadnaviridae | Partially dsDNA | Parenteral/sexual/vertical | Yes (5–10%) | Yes (recombinant HBsAg) |
| HCV | Flaviviridae | ssRNA (+) | Parenteral | Yes (70–85%) | No |
| HDV | Deltavirus | Circular ssRNA (−) | Parenteral; HBV co-infection essential | Variable | HBV vaccine prevents |
| HEV | Hepeviridae | ssRNA (+) | Faeco-oral | No (except genotype 3 in immunocompromised) | Yes (recombinant; not in India) |
Epidemiology in India:
- HAV: children, endemic; improving sanitation shifts peak age older
- HBV: 40 million carriers; vertical transmission in neonates accounts for 40% of chronic HBV
- HCV: 6–12 million; IV drug users, unsafe transfusions (pre-NAT era)
- HEV: major cause of epidemic jaundice in adults; floods, contaminated water
Hepatitis A Virus (HAV)
Hepatitis A Virus: Transmission, Pathogenesis, Diagnosis, and Prevention
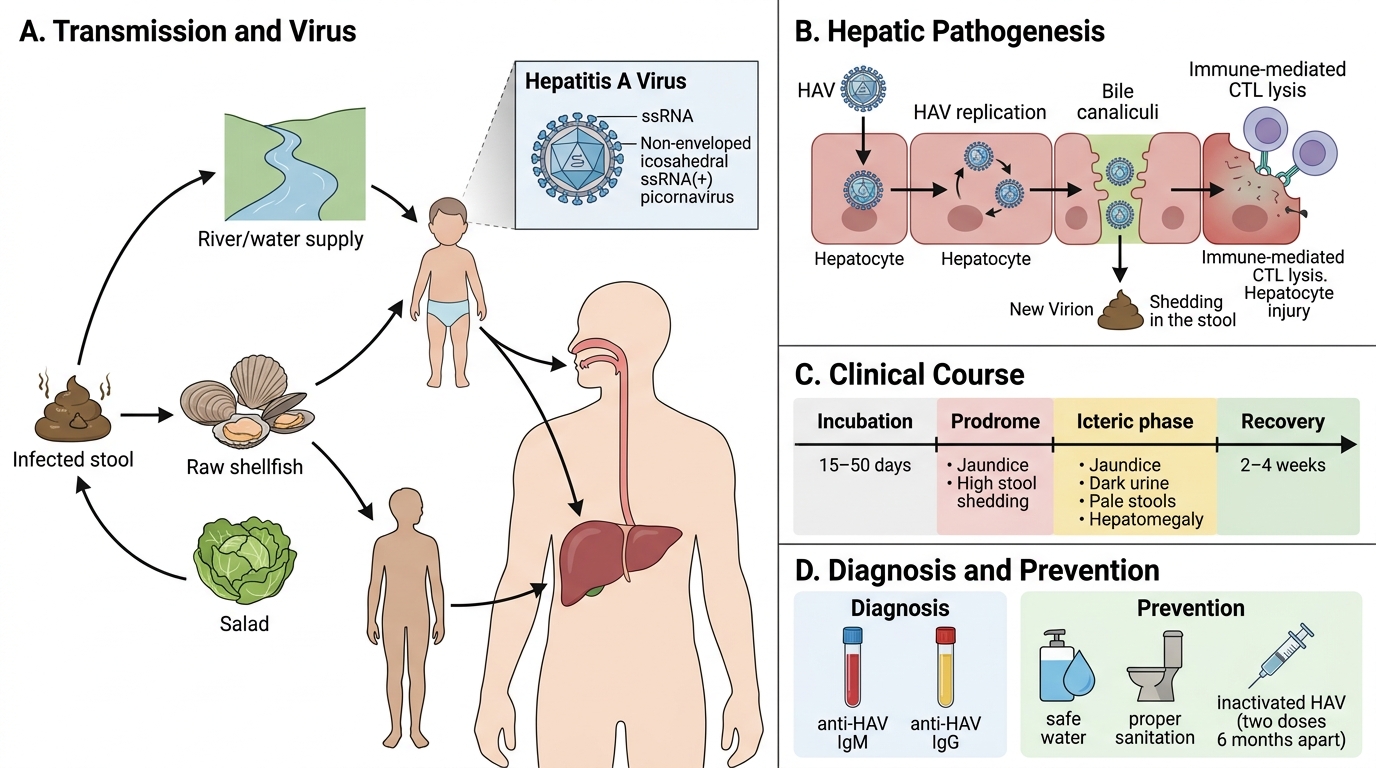
HAV is a non-enveloped, ssRNA(+) picornavirus. It replicates in hepatocytes, is excreted in bile, and shed in stool in large quantities during the prodromal phase (before jaundice appears).
Epidemiology: Faeco-oral; contaminated water, raw shellfish (bivalves concentrate virus), salads. Incubation 15–50 days. Highly endemic in India among children (seroprevalence >90% by age 10 in low-income settings).
Pathogenesis: Direct cytopathic effect is minimal; hepatocyte injury is largely immune-mediated (CTL lysis of infected cells). Self-limiting — no chronicity, no carrier state.
Clinical features:
- Prodrome: fever, malaise, anorexia, nausea, right upper quadrant pain
- Icteric phase: jaundice, dark urine (bilirubinuria), pale stools, hepatomegaly
- Recovery within 2–4 weeks
- Rarely: cholestatic hepatitis (prolonged jaundice) or fulminant hepatic failure (<1%)
Diagnosis: Anti-HAV IgM = acute infection; anti-HAV IgG = past infection or immunity (vaccine or natural).
Prevention: Improved water/sanitation; inactivated HAV vaccine (two doses, 6 months apart) for travellers and risk groups.
Hepatitis E Virus (HEV)
Hepatitis E Virus: Water-Borne Outbreaks and Pregnancy Risk
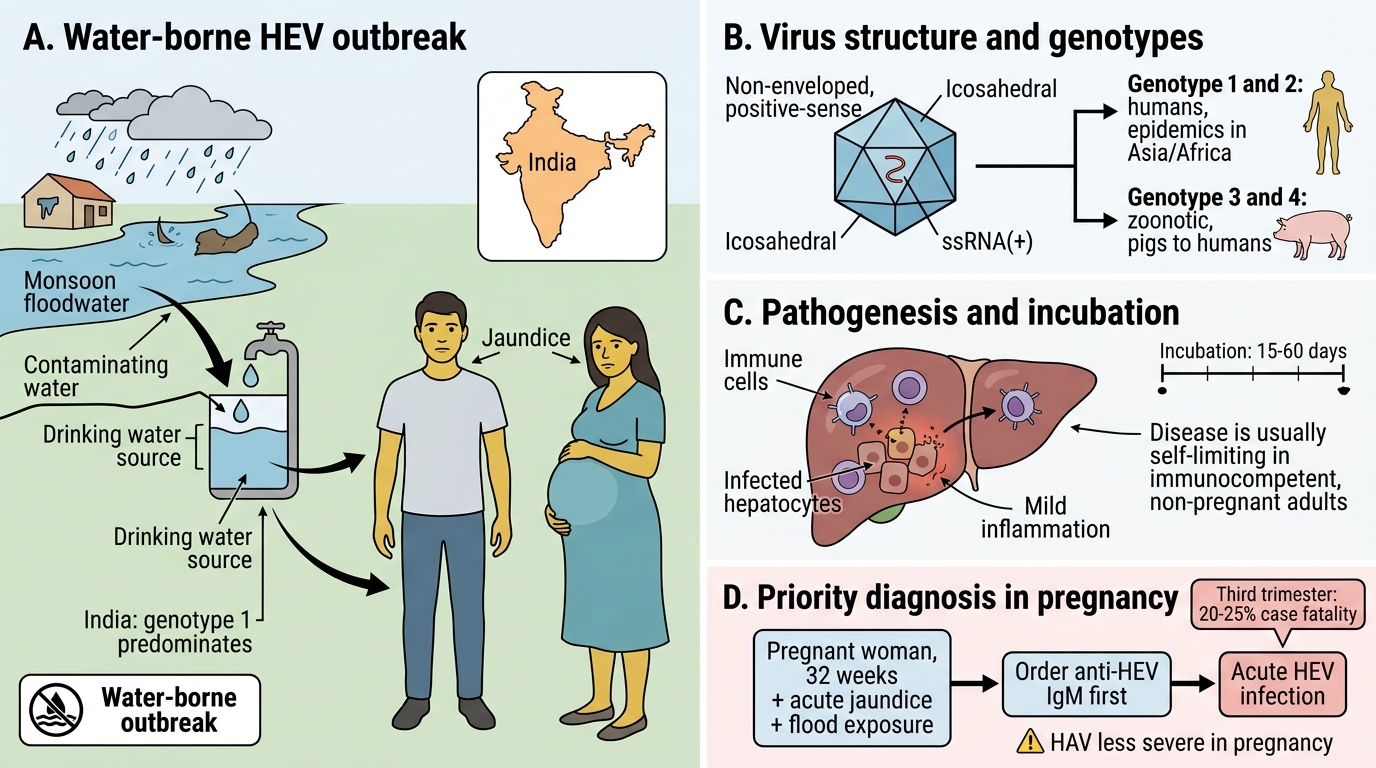
HEV is a non-enveloped, ssRNA(+) hepevirid. Four main genotypes: genotypes 1 and 2 are restricted to humans and cause epidemic hepatitis in Asia and Africa; genotype 3 and 4 infect humans zoonotically (pigs).
Epidemiology: Water-borne outbreaks in India (especially post-flood); genotype 1 predominates in India. Incubation 15–60 days. Young adults most affected (unlike HAV).
High-risk groups:
- Pregnant women: 20–25% case fatality rate in third trimester (highest of all viral hepatitis); mechanism unclear — hormonal, immunological, high viral load
- Patients with pre-existing chronic liver disease
Pathogenesis: Similar immune-mediated hepatocyte damage as HAV; primarily self-limiting in immunocompetent non-pregnant adults.
Diagnosis: Anti-HEV IgM = acute infection; anti-HEV IgG = past infection; HEV RNA by RT-PCR (acute phase viraemia).
Key clinical implication (MI4.9): In a pregnant woman with jaundice during a monsoon outbreak, HEV is the priority diagnosis; HAV is less severe in pregnancy. Test: anti-HEV IgM first.
SELF-CHECK
A 30-year-old pregnant woman (32 weeks gestation) from a flood-affected area presents with acute jaundice and elevated liver enzymes. Anti-HAV IgM is negative. Which test should be ordered next, and why?
A. HBsAg, because HBV is the commonest cause of jaundice in pregnancy in India
B. Anti-HEV IgM, because HEV genotype 1 causes epidemic hepatitis in India and carries 20–25% fatality in third trimester
C. HCV RNA, because HCV is the commonest cause of water-borne hepatitis
D. Anti-HAV IgG, to check for past immunity
Reveal Answer
Answer: B. Anti-HEV IgM, because HEV genotype 1 causes epidemic hepatitis in India and carries 20–25% fatality in third trimester
In flood/outbreak settings in India, hepatitis E (genotype 1) is the leading cause of epidemic jaundice in adults, and its mortality in the third trimester of pregnancy is 20–25%—the highest of any viral hepatitis. Anti-HEV IgM is the first-line acute-phase diagnostic test. HAV (option A context) is already negative here. HCV is parenteral, not waterborne. Anti-HAV IgG tests for past immunity, not acute disease.