Page 9 of 18
MI4.7-9 | Viral Hepatitis — SDL Guide (Part 2)
Hepatitis B Virus (HBV) — Structure & Markers
HBV Structure and Serological Markers
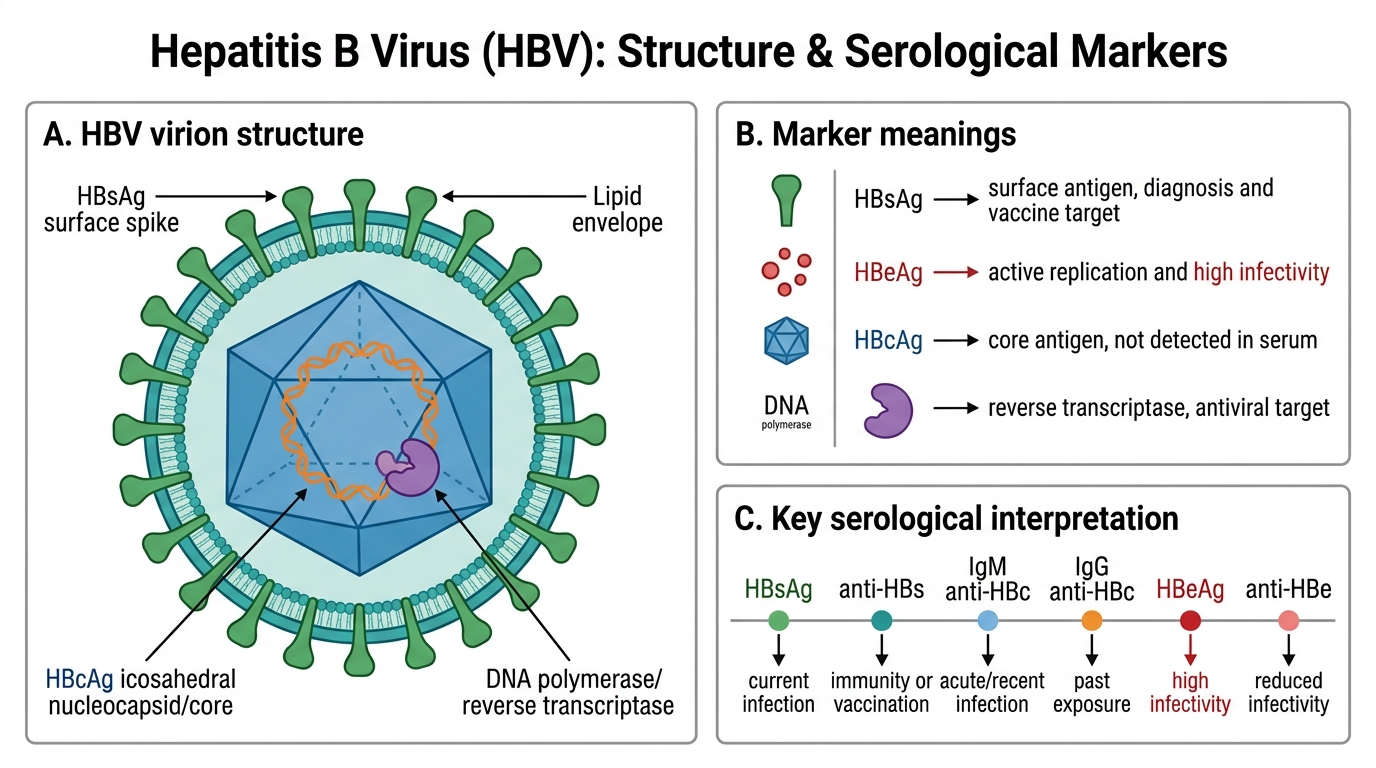
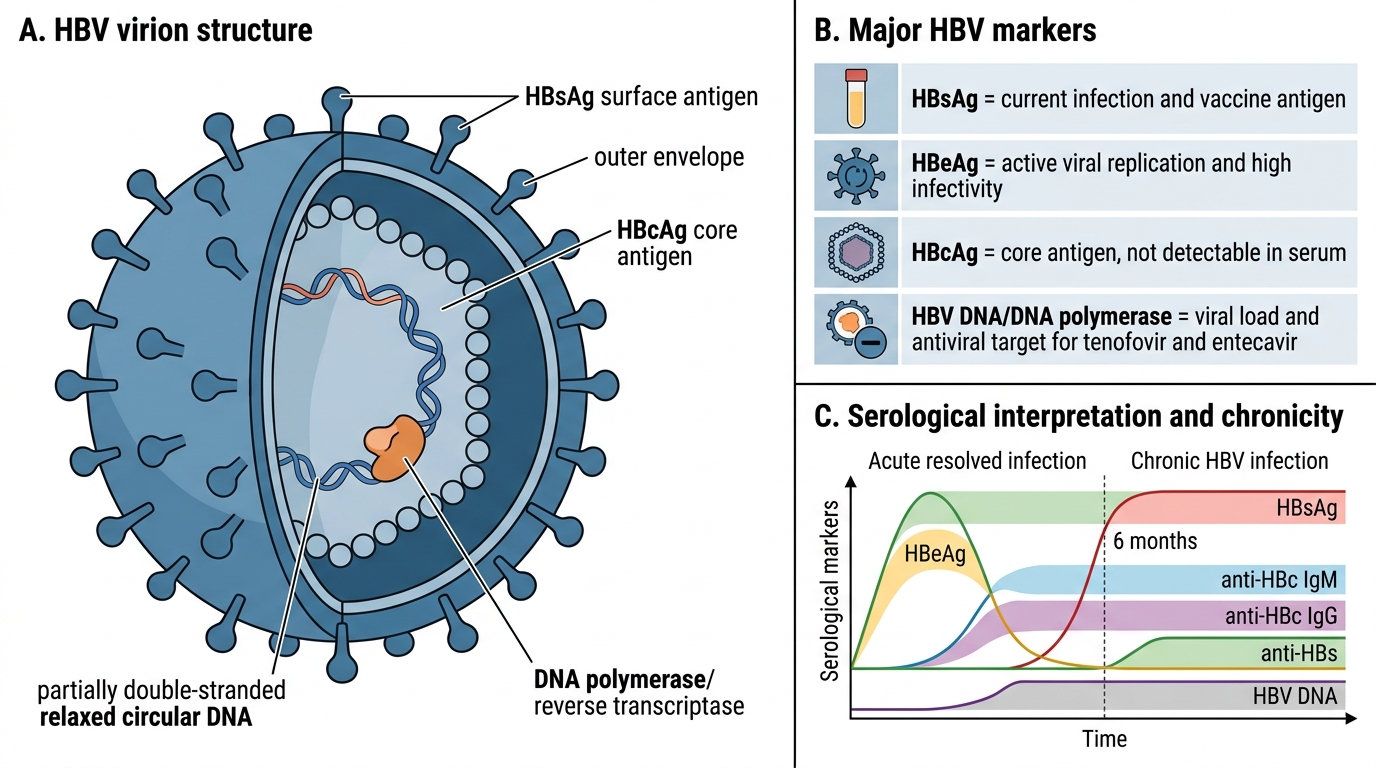
HBV is a partially double-stranded DNA hepadnavirus with a complex structure:
- Outer envelope: contains HBsAg (surface antigen) — the basis of both diagnosis and vaccine
- Core: HBcAg (core antigen, not detectable in serum); HBeAg (soluble secreted form — marker of active replication and high infectivity)
- DNA polymerase (reverse transcriptase activity) — target for antivirals (tenofovir, entecavir)
Key serological markers:
| Marker | What it means |
|---|---|
| HBsAg | Active infection (acute or chronic); carrier state |
| Anti-HBs (HBsAb) | Immunity (vaccination or recovery) |
| Anti-HBc IgM | Acute HBV infection ('window period' marker) |
| Anti-HBc IgG | Past infection or chronic carrier |
| HBeAg | Active viral replication, high infectivity |
| Anti-HBe | Declining replication (seroconversion — good sign) |
| HBV DNA | Gold standard for viral load; guides antiviral therapy |

Serological Timeline of Acute HBV Infection
HBV Pathogenesis & Chronicity
HBV Structure and Serological Markers
Transmission: Parenteral (blood, needles), sexual, vertical (mother-to-neonate) — most important route in India; neonates infected at birth have 90% risk of chronicity.
Pathogenesis: HBV itself is not directly cytopathic; injury is CTL-mediated (CD8+ T cells kill infected hepatocytes). In chronic infection, immune tolerance → insufficient CTL response → persistent viraemia without adequate clearance.
Natural history:
1. Acute HBV (adults): 90–95% recover fully with seroconversion; 5–10% become chronic
2. Chronic HBV phases:
- Immune tolerance (high HBeAg, high DNA, minimal inflammation)
- Immune clearance (HBeAg positive hepatitis — active necroinflammation)
- Immune control (HBeAg seroconversion → anti-HBe; low DNA; inactive carrier)
- Immune escape (HBeAg-negative hepatitis — pre-core mutations)
3. Complications: Cirrhosis (20%), hepatocellular carcinoma (risk 100× higher than general population)
Treatment: Oral antivirals — tenofovir or entecavir (suppress HBV DNA; rarely achieve cure = HBsAg clearance)
Hepatitis C & D — Key Points
Hepatitis C and D: Key Points
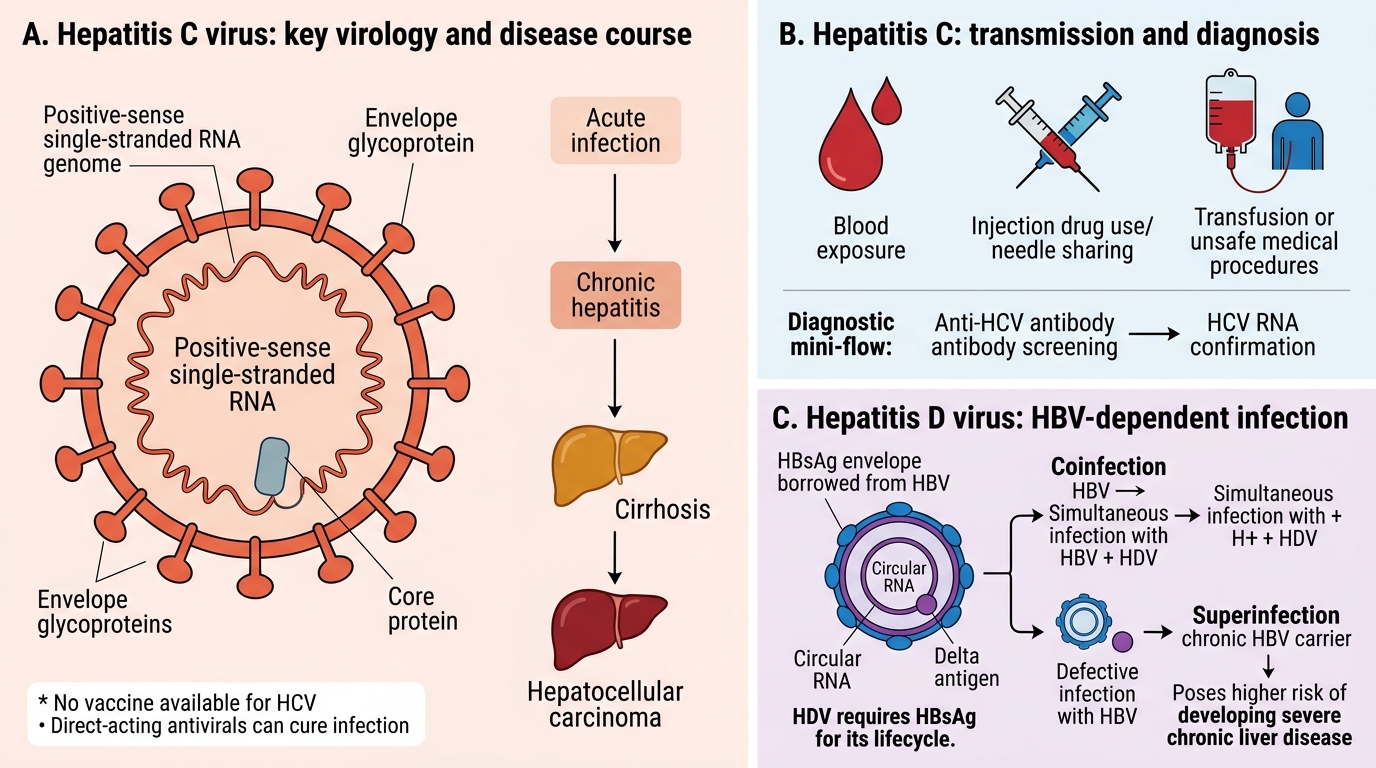
Hepatitis C (HCV):
- Enveloped ssRNA(+) flavivirus; 6 major genotypes; genotype 1 dominant globally, genotype 3 common in India
- Parenteral only: IV drug use (#1 risk in India), unsafe injections, transfusions (pre-NAT screening), needlestick, sexual (lower risk)
- Chronicity: 70–85% — HCV is the most likely hepatitis virus to become chronic
- No vaccine available; NS5B RNA polymerase and NS3 protease are antiviral targets
- Treatment revolution: Direct-acting antivirals (DAAs — sofosbuvir, ledipasvir/sofosbuvir) → >95% cure rates, 12-week oral regimens
- Diagnosis: Anti-HCV ELISA (screening) → HCV RNA PCR (confirmatory + quantitative)
Hepatitis D (HDV):
- Unique 'virusoid' — defective virus requiring HBsAg as its envelope; cannot infect without HBV
- Two patterns:
- Co-infection (simultaneous HDV + HBV): fulminant hepatitis risk high; but both resolve together
- Super-infection (HDV in chronic HBV carrier): rapidly accelerates cirrhosis
- Prevention: HBV vaccination prevents HDV
- Diagnosis: Anti-HDV antibodies; HDV RNA PCR
SELF-CHECK
A blood donor's sample tests positive for HBsAg. Further testing shows: Anti-HBc IgM negative, Anti-HBc IgG positive, HBeAg negative, Anti-HBe positive, HBV DNA 500 IU/mL. What is the most likely interpretation?
A. Acute HBV infection
B. Inactive HBV carrier state (past seroconversion from HBeAg to anti-HBe)
C. Vaccinated individual (anti-HBs positive)
D. Window period of acute HBV infection
Reveal Answer
Answer: B. Inactive HBV carrier state (past seroconversion from HBeAg to anti-HBe)
This pattern — HBsAg positive, anti-HBc IgG positive (past/chronic), anti-HBc IgM negative (not acute), HBeAg negative, anti-HBe positive (seroconverted), low HBV DNA — is classic for an inactive HBsAg carrier (previously called healthy carrier). This person had HBeAg-positive chronic HBV but has seroconverted and now has suppressed viral replication. Window period would show anti-HBc IgM positive; vaccination shows anti-HBs but NOT anti-HBc (no natural infection).