Page 1 of 10
MI1.3-4 | Laboratory Diagnosis & Molecular Methods — SDL Guide
Learning Objectives
- Describe the basic principles of molecular biology relevant to clinical microbiology, including DNA replication, transcription, and translation.
- Explain the concept and significance of molecular genetics in understanding microbial pathogenicity and drug resistance.
- Discuss key molecular techniques — PCR, nucleic acid hybridisation, sequencing, and CRISPR-based diagnostics — applied to clinical diagnosis.
- Describe conventional and automated laboratory methods used to detect causative agents of infectious diseases, including microscopy, culture, serology, and antigen detection.
INSTRUCTIONS
Accurate laboratory diagnosis is the backbone of rational antimicrobial therapy and infection control. In Indian hospitals, where tuberculosis, enteric fever, dengue, and multi-drug-resistant organisms are endemic, choosing the right test at the right time saves lives and stewardship budgets. Work through this module with your clinical reasoning active — ask yourself why each method exists and when you would reach for it.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, 10th ed., Ch 8–10 (textbook)
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th ed., Ch 3–4 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 19-year-old engineering student from Chennai presents with 12 days of fever, relative bradycardia, and rose spots on the trunk. Blood culture on day 8 grew gram-negative bacilli — but the result arrived only after three days. His family asks: 'Couldn't you have diagnosed this faster?' The answer lies in understanding how our laboratory methods have evolved — from a single drop of blood on a slide to a molecular test that delivers a result in under two hours.
WHY THIS MATTERS
As a future clinician, you will order laboratory tests daily. Understanding how each test works helps you interpret results correctly, recognise false positives/negatives, and select the most cost-effective method — especially important in resource-constrained Indian settings where over- and under-testing are both common. Molecular methods are rapidly entering district-hospital laboratories through NTEP's CBNAAT network and ICMR-funded platforms, so fluency with these tests is no longer optional.
RECALL
Before proceeding, recall from your Phase 1 Biochemistry:
- The central dogma: DNA → RNA → Protein
- The structure of the DNA double helix and complementary base pairing (A-T, G-C)
- The principle of enzyme-substrate specificity (relevant to restriction enzymes and polymerases)
- The difference between gram-positive and gram-negative bacterial cell walls (from General Microbiology I)
Principles of Molecular Biology in Clinical Microbiology
Molecular Biology Principles in Clinical Microbiology
Molecular biology applies the chemistry of nucleic acids to identify pathogens with precision impossible by conventional morphology alone.
Key concepts:
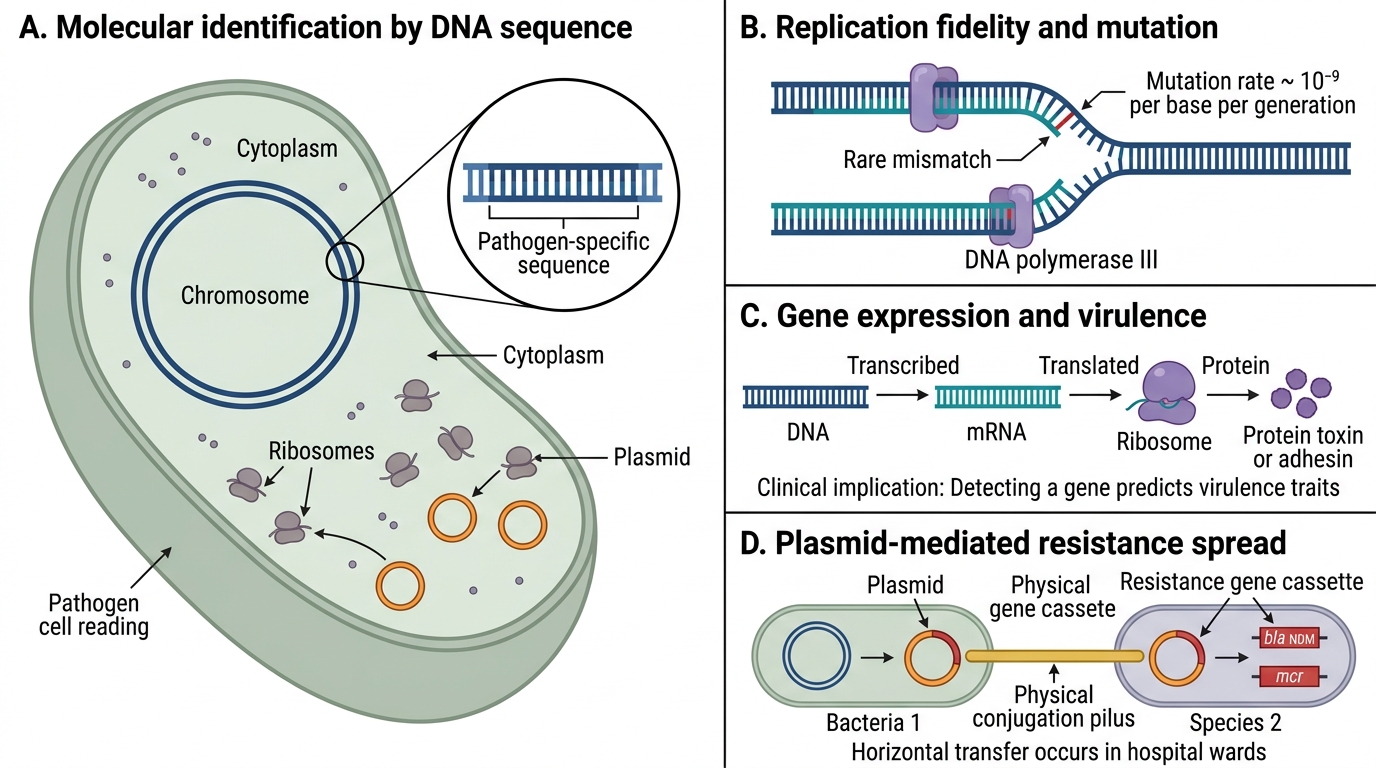
- DNA as genetic information: Every organism carries a unique genomic sequence. Detecting pathogen-specific sequences confirms identity without the need for viable organisms or specific antibody responses.
- Replication fidelity and error: Bacterial DNA replication uses high-fidelity DNA polymerase III. Mutations accumulate at ~10⁻⁹ per base per generation — slow enough for sequence conservation within a species, but fast enough for drug-resistance mutations to emerge under antibiotic pressure.
- Transcription & translation: Gene expression converts DNA → mRNA → protein. Many virulence factors (toxins, adhesins, capsule proteins) are gene products; detecting the encoding gene predicts pathogen behaviour.
- Plasmids and mobile genetic elements: Resistance genes (e.g., blaNDM, mcr) are often carried on plasmids — circular extra-chromosomal DNA that transfers between bacteria by conjugation. This is why resistance spreads rapidly across unrelated species in hospital wards.

R Plasmid, Integron, and Conjugative Transfer
5. Molecular genetics significance: Studying microbial genomes reveals:
- Phylogenetic relationships (outbreak tracing)
- Mechanisms of drug resistance (targeted therapy)
- Virulence gene profiles (predicting disease severity)
- Novel antigens for vaccine development
Molecular Diagnostic Techniques
PCR and Clinical Molecular Diagnostic Techniques
1. Polymerase Chain Reaction (PCR)
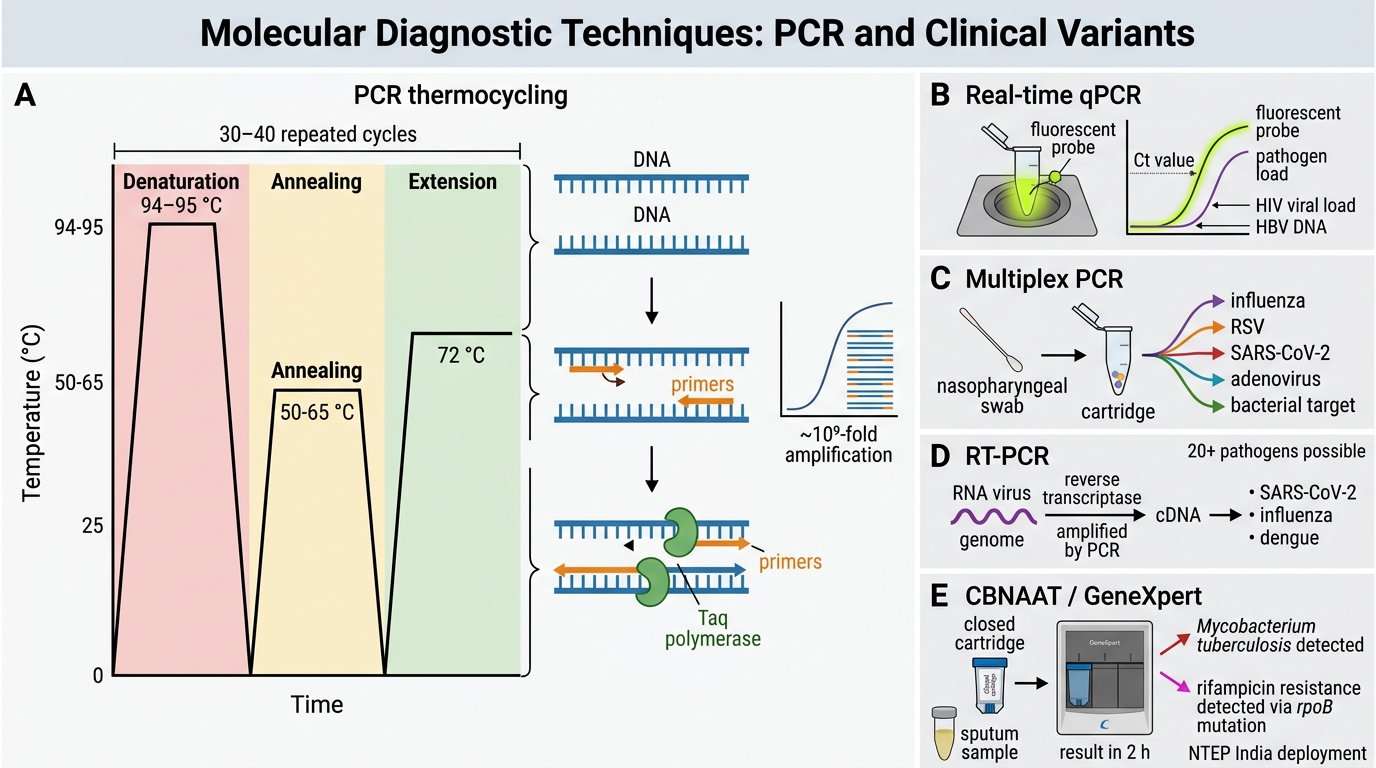
PCR is the amplification of a target DNA sequence using thermocycling with a thermostable DNA polymerase (Taq polymerase).
Three steps per cycle:
- Denaturation (94–95 °C): double-stranded DNA melts
- Annealing (50–65 °C): primers bind to complementary sequences flanking the target
- Extension (72 °C): Taq polymerase synthesises new DNA from each primer
30–40 cycles amplify target DNA ~10⁹-fold from a starting copy.
Clinical variants:
- Real-time (qPCR): quantifies pathogen load (HIV viral load, HBV DNA) using fluorescent probes; result in 2–4 h
- Multiplex PCR: detects multiple targets simultaneously (e.g., FilmArray Respiratory Panel identifies 20+ pathogens from one nasopharyngeal swab)
- Reverse-transcription PCR (RT-PCR): first converts RNA → cDNA (for RNA viruses: SARS-CoV-2, influenza, dengue)
- CBNAAT / GeneXpert: integrated real-time PCR in a cartridge system — detects Mycobacterium tuberculosis AND rifampicin resistance (rpoB mutations) in 2 h; widely deployed under NTEP across India

PCR Thermocycling Steps
2. Nucleic Acid Hybridisation
Single-stranded probe DNA with a known sequence binds (hybridises) to complementary target sequences. Detection signal: fluorescent or chemiluminescent label.
- DNA probes: used for Mycoplasma, Legionella, gonorrhoea confirmation
- In situ hybridisation (ISH): localises pathogen nucleic acid within tissue sections — useful for EBV in lymphoma biopsy
- DNA microarrays: thousands of probes on a chip — simultaneous typing of HPV genotypes or respiratory viruses
3. DNA Sequencing
- Sanger sequencing: gold standard for confirming resistance mutations (e.g., rpoB, katG in MTB); ~24–48 h, targeted
- Next-Generation Sequencing (NGS) / Whole Genome Sequencing (WGS): sequences the entire pathogen genome; used in outbreak investigation (molecular epidemiology), metagenomic pathogen identification in sterile-site samples where culture is negative
4. CRISPR-Based Diagnostics (SHERLOCK, DETECTR)
CRISPR-Cas enzymes recognise and cleave specific nucleic acid sequences, triggering a reporter signal. These platforms are nucleic-acid-amplification tests (NAATs) comparable in sensitivity to PCR but designed for low-resource field deployment. Research platforms; not yet standard in Indian district hospitals, but included in current curricula.
5. Loop-Mediated Isothermal Amplification (LAMP)
LAMP amplifies DNA at a single temperature (60–65 °C) — no thermocycler required. Result visible by turbidity or colour change in 30–60 min. Used for point-of-care dengue NS1 RNA and MTB detection.
CLINICAL PEARL
PCR does not distinguish live from dead organisms. A patient treated for pulmonary TB may remain PCR-positive for weeks after successful therapy because dead mycobacterial DNA persists. Always correlate molecular results with clinical improvement and, where available, culture viability data. Similarly, a positive SARS-CoV-2 PCR beyond day 10 in a non-immunocompromised patient rarely indicates infectiousness.
Conventional Laboratory Methods for Detection of Infectious Agents
Conventional Microscopy Methods for Infectious Agent Detection
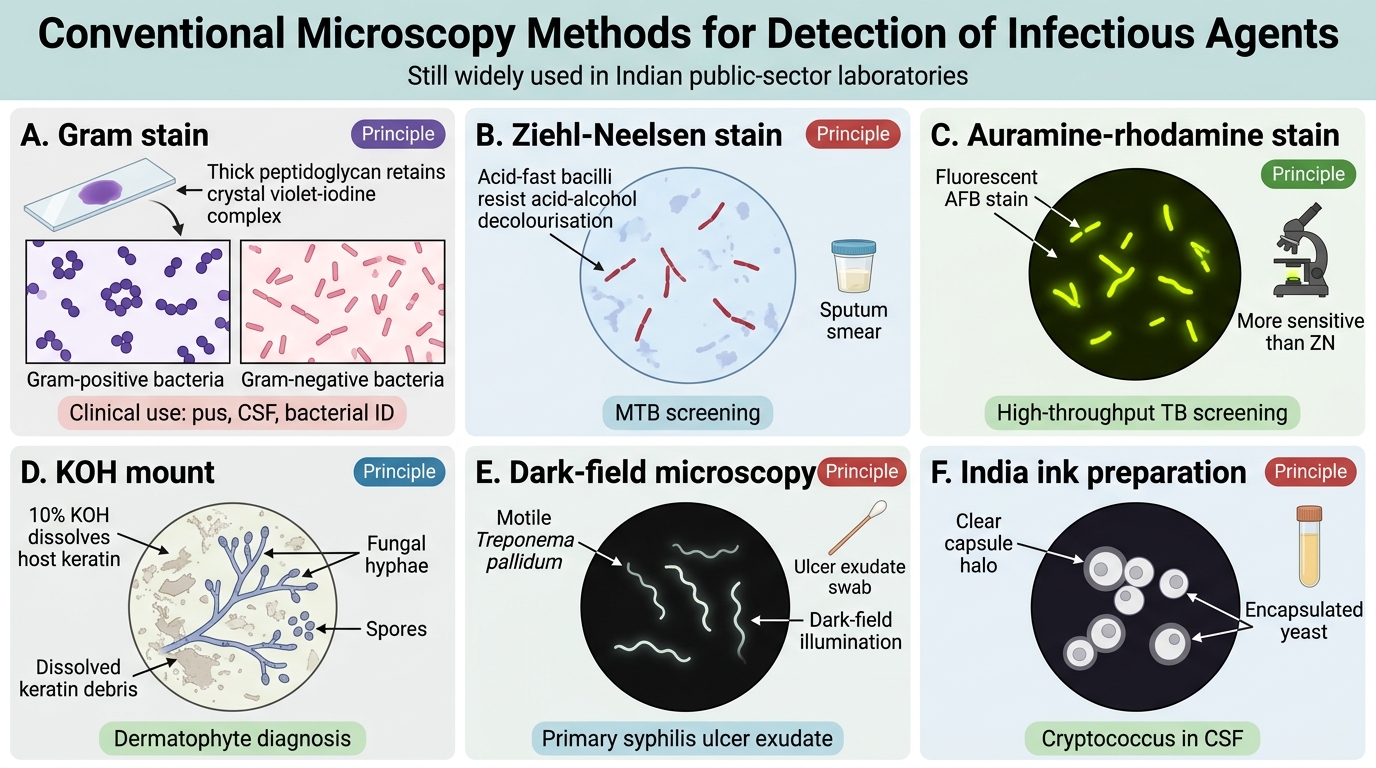
Despite the excitement of molecular methods, conventional techniques remain the most widely used in Indian public-sector laboratories.
1. Microscopy
| Technique | Principle | Key Application |
|---|---|---|
| Gram stain | Crystal violet-iodine complex retained by thick peptidoglycan (gram+) | Rapid bacterial ID from pus, CSF |
| Ziehl-Neelsen (ZN) stain | Acid-fast bacilli resist decolourisation with acid-alcohol | Sputum smear for MTB |
| Auramine-rhodamine | Fluorescent stain for AFB; more sensitive than ZN | High-throughput TB screening |
| KOH mount | Alkali dissolves host keratin; reveals fungal hyphae/spores | Skin scrapings for dermatophytes |
| Dark-field microscopy | Visualises motile Treponema pallidum | Primary syphilis ulcer exudate |
| India ink preparation | Reveals capsule of Cryptococcus neoformans | CSF in HIV/AIDS patients |

Laboratory Diagnosis: Smear Microscopy, Culture and Antigen Detection
2. Culture
Culture remains the gold standard — it provides viable organisms for susceptibility testing and definitive identification.
- Nutrient broth/agar: non-selective (most aerobes)
- MacConkey agar: selective for gram-negatives; differentiates lactose fermenters (pink) from non-fermenters (colourless) — critical for enteric diagnosis
- Blood agar: supports fastidious organisms; beta-haemolysis identifies Streptococcus pyogenes
- Chocolate agar (VCAT): for Neisseria gonorrhoeae, Haemophilus
- Löwenstein-Jensen (LJ) medium: slow-growing M. tuberculosis visible in 3–8 weeks; BACTEC MGIT (liquid) reduces this to 10–14 days
- Sabouraud dextrose agar (SDA): low pH, high glucose — selective for fungi
Biochemical identification panels (e.g., API 20E for Enterobacteriaceae) characterise isolates by metabolic reactions; automated systems (VITEK 2, BD Phoenix) do this in 4–8 h and simultaneously report MIC-based susceptibility.
3. Antigen Detection
Detects pathogen-derived molecules directly in clinical specimens.
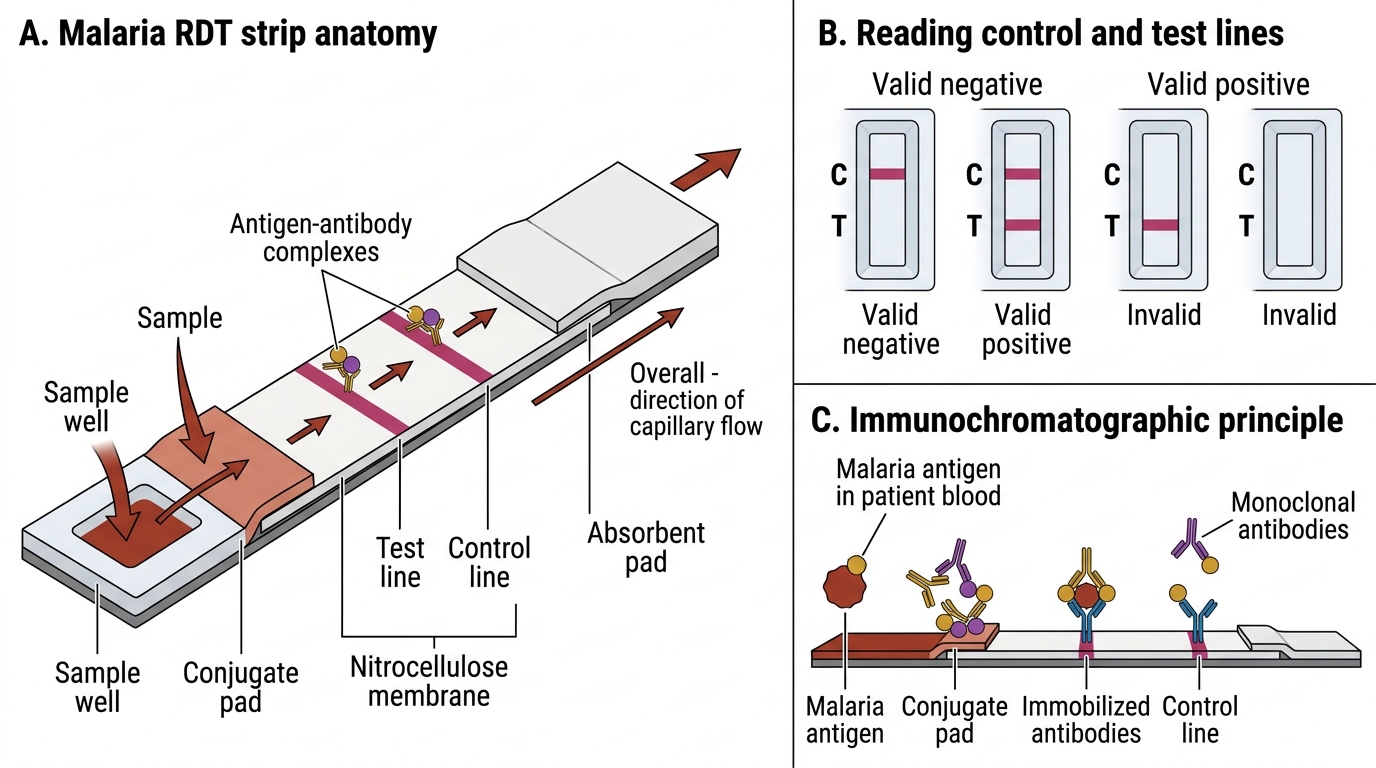
- Lateral flow immunochromatographic assay (LFIA): rapid, bedside — malaria RDT (HRP-2 antigen), dengue NS1, COVID-19 Ag, streptococcal Ag from throat swab
- ELISA (enzyme-linked immunosorbent assay): quantitative; widely used for hepatitis B surface antigen (HBsAg), HIV Ag/Ab combo 4th-generation test
- Immunofluorescence (direct DFA): fluorescent antibody labels pathogen in smear — Pneumocystis jirovecii, rabies virus in corneal/brain tissue
4. Serology (Antibody Detection)
Detects host antibody response — useful when pathogen is difficult to culture or present in low numbers.
- IgM vs IgG: IgM = recent/acute infection; IgG = past infection or immunity
- Widal test: agglutination for Salmonella Typhi/Paratyphi — limited specificity in endemic India (endemic baseline titres); O antigen titre ≥1:160 meaningful in febrile patient with compatible history
- ELISA: dengue IgM/IgG, leptospira IgM, scrub typhus IgM (Weil-Felix as backup)
- Western blot / immunoblot: confirmatory test for HIV (after reactive ELISA), Lyme disease
- Complement fixation test (CFT): older technique; still used for Mycoplasma, rickettsial serology in some reference labs
Malaria Rapid Diagnostic Test: Lateral Flow Immunochromatographic Assay
5. Automated & Rapid Systems
- MALDI-TOF MS (Matrix-Assisted Laser Desorption/Ionisation – Time of Flight Mass Spectrometry): Protein fingerprinting of bacterial/fungal colonies; species identification in seconds; increasingly available in Indian tertiary centres
- Automated blood culture systems (BACTEC, BacT/ALERT): continuous fluorescent monitoring of CO₂ production; flags positivity in median 12–24 h instead of 3 days with manual subculture
- Molecular point-of-care (POCT): GeneXpert, Abbott ID NOW — near-patient testing in 10–45 min
SELF-CHECK
A 35-year-old man presents with fever, productive cough, and night sweats for 6 weeks. Sputum ZN smear is negative. Which single investigation would provide both pathogen identification AND rifampicin resistance data within 2 hours?
A. Löwenstein-Jensen culture
B. GeneXpert MTB/RIF (CBNAAT)
C. Sputum ELISA for anti-TB antibodies
D. Auramine-rhodamine fluorescent smear
Reveal Answer
Answer: B. GeneXpert MTB/RIF (CBNAAT)
GeneXpert MTB/RIF (CBNAAT) is a cartridge-based real-time PCR system that simultaneously detects M. tuberculosis DNA and rpoB mutations (conferring rifampicin resistance) in approximately 2 hours. LJ culture takes 3–8 weeks. Serological tests for TB have poor sensitivity and specificity and are banned from routine use by ICMR. Auramine smear is more sensitive than ZN but still cannot detect rifampicin resistance.
Choosing the Right Method — A Clinical Framework
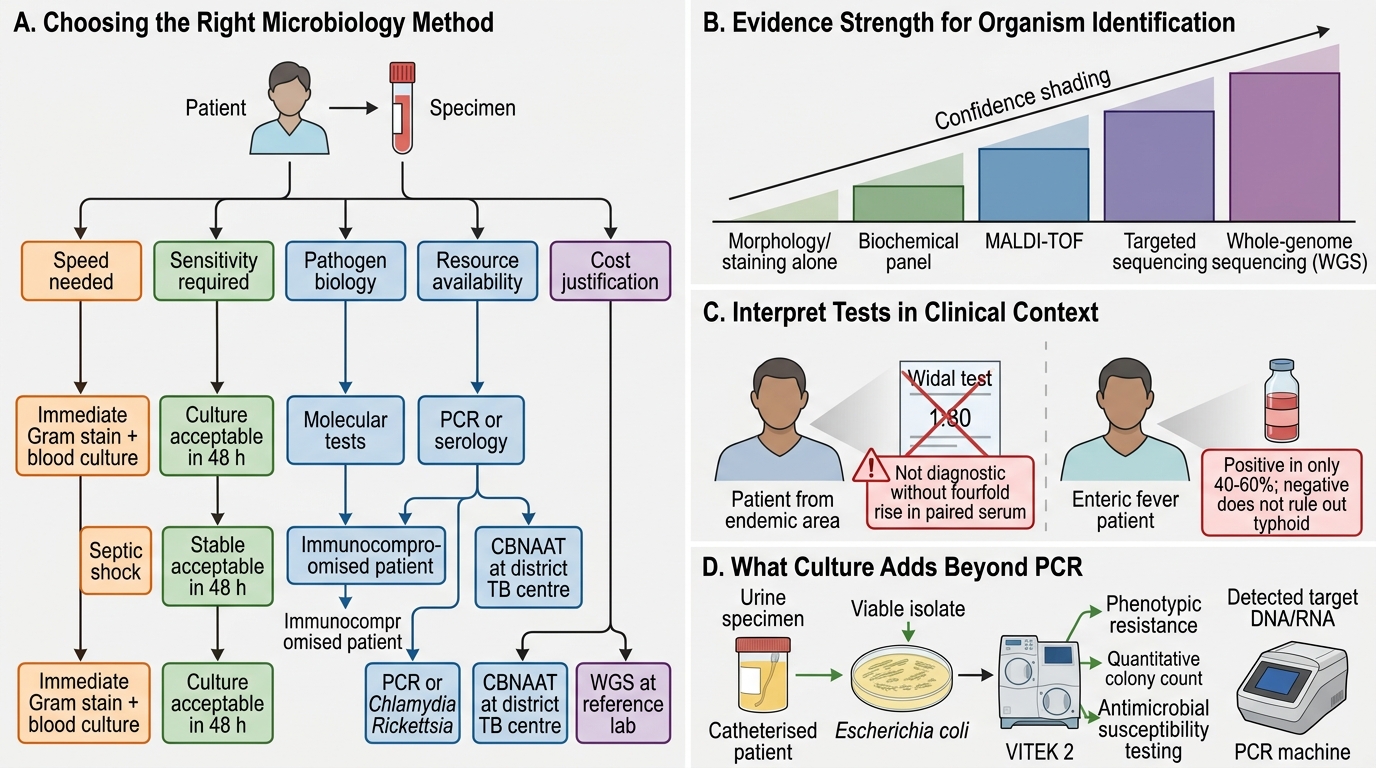
Choosing the Right Microbiology Diagnostic Method
No single test suits every scenario. Selection depends on:
- Speed needed: septic shock → immediate gram stain + blood culture + broad empirical therapy; stable outpatient → culture result acceptable in 48 h
- Sensitivity required: immunocompromised patient — molecular > culture > serology
- Pathogen biology: obligate intracellular organisms (Chlamydia, Rickettsia) cannot be cultured on standard media → PCR or serology mandatory
- Resource availability: CBNAAT available at district TB centre; WGS only at reference laboratories (NCDC, CMC Vellore)
- Cost: single PCR vs. culture with VITEK 2 — justify to the patient or insurance payer
Hierarchy of evidence for organism identification:
> WGS > targeted sequencing > MALDI-TOF > biochemical panel > morphology/staining alone
CLINICAL PEARL
'Treat the patient, not the test.' A Widal test of 1:80 in a patient from an endemic area is meaningless without a fourfold rise in paired serum. Conversely, blood culture is positive in only 40–60% of enteric fever cases — a negative culture does not rule out typhoid. Always interpret laboratory results in the context of clinical presentation, travel/exposure history, and the pre-test probability of disease.
SELF-CHECK
A urine culture from a catheterised patient grows Escherichia coli. The automated VITEK 2 system reports the result in 6 hours. What additional critical information does culture provide that a PCR-based test alone cannot?
A. Species identification
B. Gram-reaction of the organism
C. Minimum inhibitory concentrations (MICs) for antibiotic selection
D. Presence of the organism's DNA in the sample
Reveal Answer
Answer: C. Minimum inhibitory concentrations (MICs) for antibiotic selection
Culture provides viable organisms from which antimicrobial susceptibility testing (AST) — reporting Minimum Inhibitory Concentrations (MICs) or zone diameters — can be performed. This directly guides antibiotic selection and dose. PCR can identify the species and some resistance genes, but cannot replace phenotypic AST for determining the full susceptibility profile, especially for emerging or unusual resistance patterns. Species ID and gram reaction can be inferred from PCR or MALDI-TOF as well.
REFLECT
Consider a rural PHC in Maharashtra with limited infrastructure. A febrile child arrives with suspected meningitis. The laboratory has gram staining, CSF culture, and a latex agglutination antigen detection kit.
- Which test do you order first, and why?
- If gram stain shows gram-positive diplococci, does the child still need culture? What would culture add?
- The district hospital has a GeneXpert machine for TB. Could it help if bacterial meningitis is suspected? Why or why not?
Reflect on how resource constraints shape — but need not paralyse — laboratory-based clinical decision-making.
KEY TAKEAWAYS
Key takeaways:
- Molecular biology provides the conceptual framework for PCR, hybridisation, sequencing, and CRISPR diagnostics — all exploiting unique nucleic acid sequences to identify pathogens precisely.
- PCR (especially qPCR/CBNAAT) is the fastest high-sensitivity method for pathogens that are difficult to culture (MTB, viruses) or where resistance genotyping is clinically urgent.
- Culture remains the gold standard because it provides live organisms for phenotypic AST — indispensable for guiding targeted antibiotic therapy.
- Antigen and antibody detection (ELISA, LFIA) serve different windows of infection: antigen early in illness; IgM appears ~5–7 days post-onset; IgG indicates past exposure or immunity.
- MALDI-TOF and automated blood culture systems have transformed turnaround times in well-resourced laboratories.
- Method selection integrates clinical urgency, pathogen biology, local test availability, sensitivity/specificity trade-offs, and cost — skills built iteratively through clinical rotations.