Page 2 of 10
MI1.{5-6,11} | Specimen Collection, Transport & Epidemiology of Infection — SDL Guide
Learning Objectives
- Discuss the appropriate method of collecting and transporting clinical specimens to detect microbial agents, including patient instructions before collection.
- Demonstrate correct technique for collecting and transporting common specimen types (blood, urine, sputum, CSF, stool, wound swab).
- Describe the epidemiological basis of infectious diseases and explain how epidemiological principles are applied to prevention and control.
INSTRUCTIONS
The best laboratory test is only as good as the specimen it analyses. A poorly collected blood culture or an improperly transported stool specimen can turn a curable infection into a diagnostic puzzle. This module bridges the clinical encounter — the moment you instruct a patient and collect a sample — to the laboratory bench, and then broadens the view to the epidemiology that determines why infections occur, spread, and persist at population level.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, 10th ed., Ch 11, Ch 57 (textbook)
- Park's Textbook of Preventive & Social Medicine, 26th ed., Ch 4 (Epidemiology of Communicable Diseases) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In an ICUS in Pune, three consecutive blood cultures from a patient with post-operative fever grew Staphylococcus epidermidis. The treating surgeon concluded this was a real bacteraemia and escalated to vancomycin. Three days later, the infection control nurse noticed that all three cultures had been drawn without adequate skin antisepsis through the same central line port — classic contamination. The 'pathogen' was a skin commensal. Correct specimen collection would have prevented unnecessary vancomycin exposure — and the subsequent C. difficile diarrhoea.
WHY THIS MATTERS
Clinicians — not laboratory technicians — are often the ones collecting blood cultures, instructing patients to collect midstream urine, or deciding which specimen to send from a wound. Getting this right determines whether the laboratory delivers actionable information or noise. Beyond the individual patient, understanding epidemiology tells you why infection struck this patient in this community at this time — and what interventions will prevent the next case.
RECALL
Recall from General Microbiology I:
- Normal flora of skin, oral cavity, GI tract, and genitourinary tract
- Difference between colonisation and infection
- Basic aseptic technique principles
From Community Medicine (Phase 1):
- Herd immunity and immunisation schedule
- Chain of infection: agent → host → environment
General Principles of Specimen Collection
Golden Rules of Specimen Collection
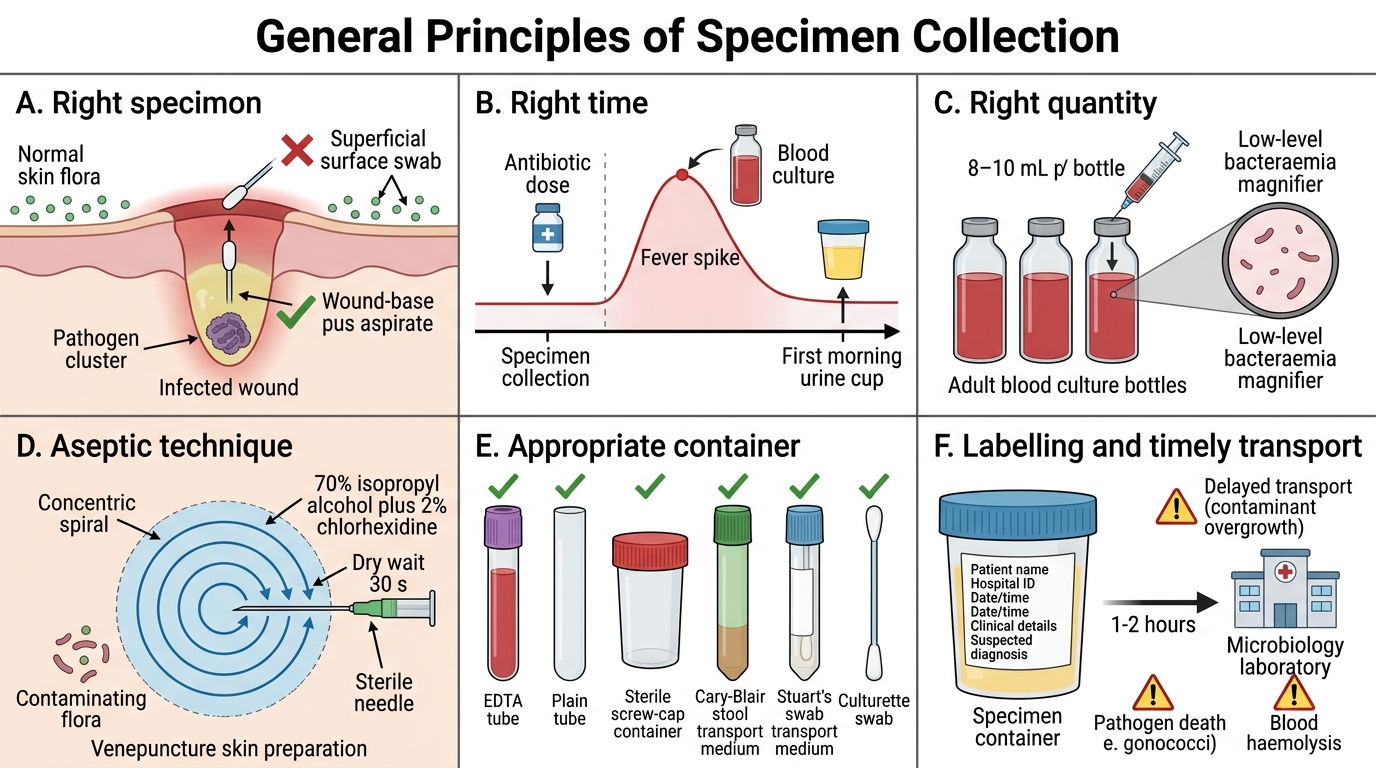
Golden rules applicable to every specimen:
- Right specimen: Collect from the actual site of infection. Pus from a wound surface is not the same as pus from the wound base — surface swabs reflect contaminating flora.
- Right time: Collect before antibiotic administration whenever possible. Blood cultures should be drawn at fever spike (bacteraemia peaks). Urine for culture: first morning void (highest bacterial concentration).
- Right quantity: Adequate volume is critical — blood cultures require 8–10 mL per bottle (adult) to detect low-level bacteraemia.
- Aseptic technique: Prevent contamination with normal flora or environmental organisms. Skin site for venepuncture must be cleaned with 70% isopropyl alcohol ± 2% chlorhexidine using a concentric spiral, allowed to dry completely (30 s).
- Appropriate container: Each specimen type has a designated container — EDTA tube, plain tube, transport media (Cary-Blair for stool, Stuart's for swabs), sterile screw-cap container, culturette swab.
- Labelling: Patient name, hospital ID, date and time of collection, clinical details, suspected diagnosis. Mislabelled specimens cause misdiagnosis.
- Timely transport: Most specimens should reach the laboratory within 1–2 hours. Delay allows overgrowth of contaminants, pathogen death (gonococci), or haemolysis (blood).
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Blood Culture Collection: Key Steps
Specimen-Specific Collection and Transport Guidelines
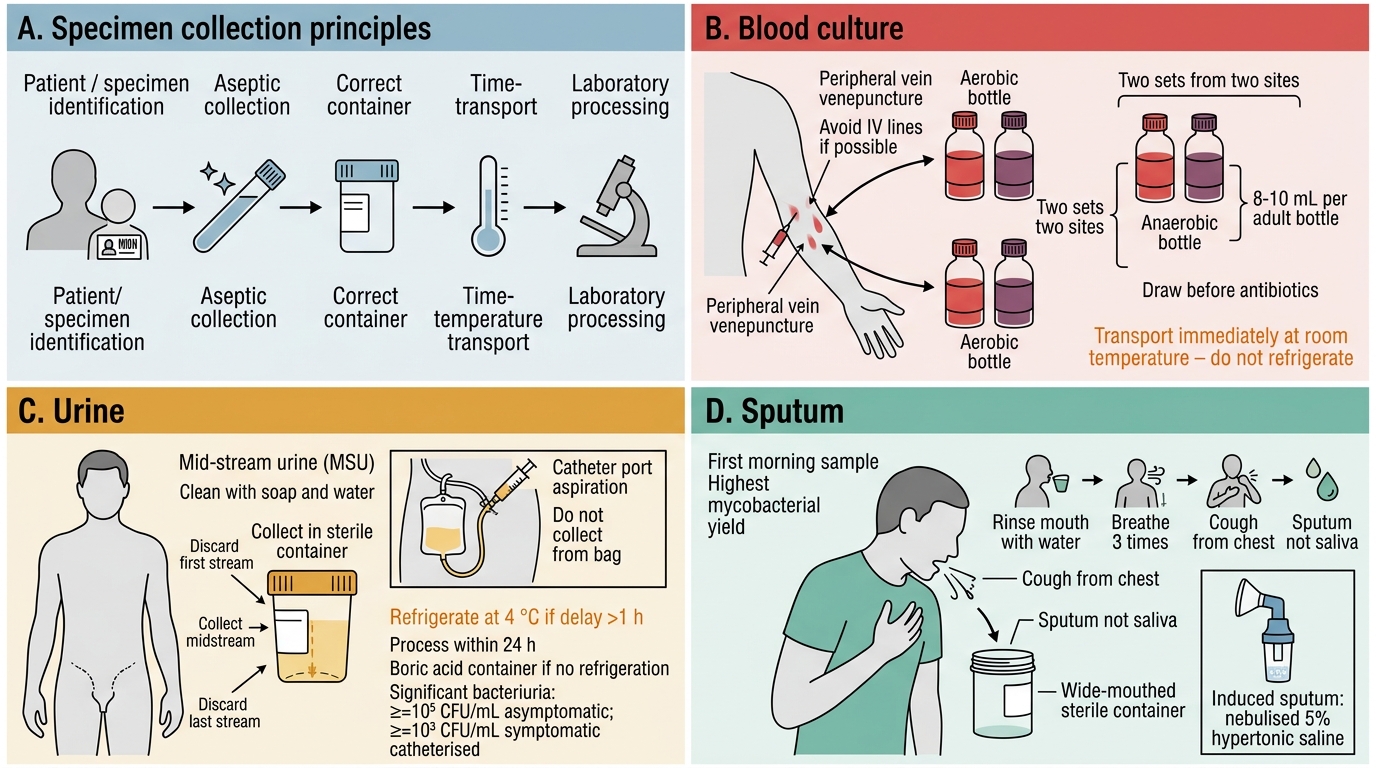
Specimen-Specific Collection and Transport Guidelines
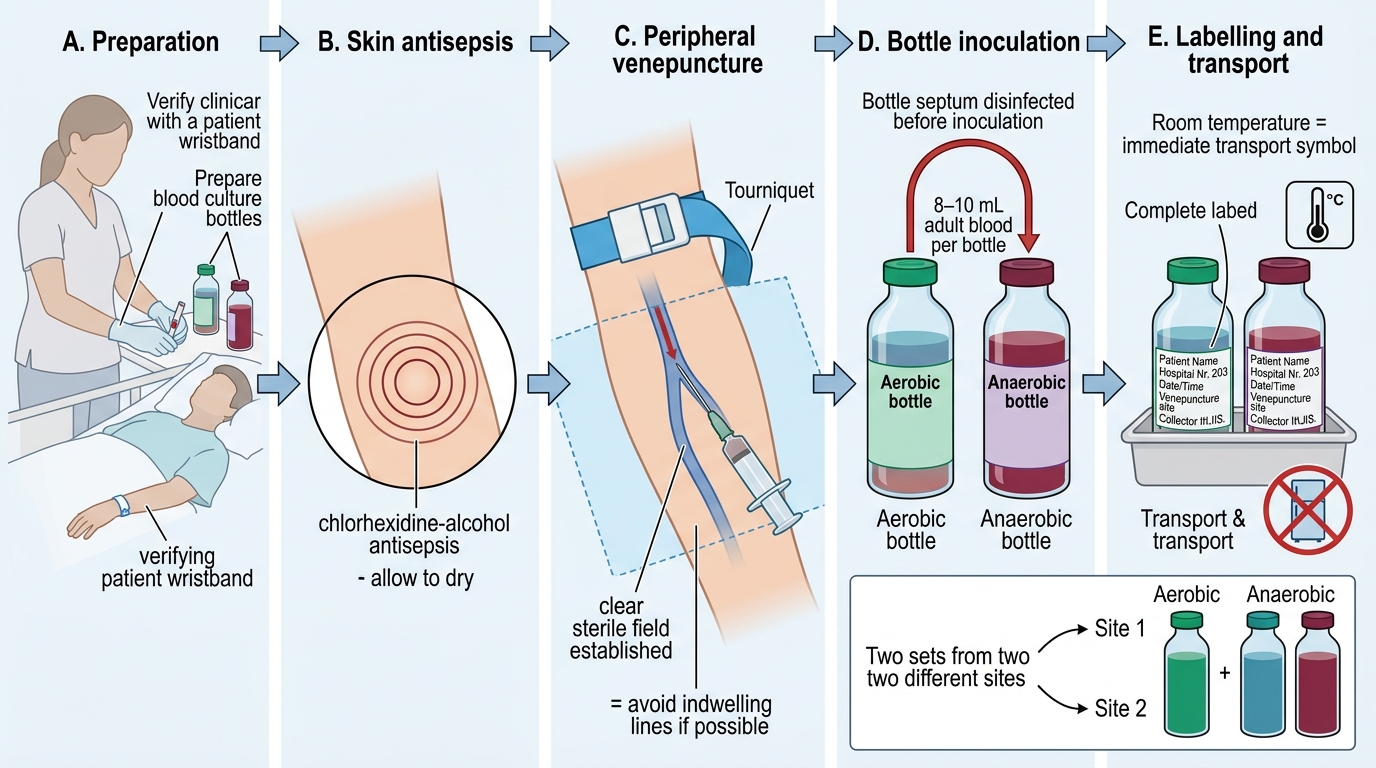
Blood Culture
- Peripheral vein venepuncture (avoid lines if possible — contamination risk)
- Two sets (each set = 1 aerobic + 1 anaerobic bottle) from two different sites
- Draw before antibiotic initiation; if already on antibiotics, draw at drug trough
- Volume: 8–10 mL/bottle adult; 1–3 mL/bottle paediatric
- Transport at room temperature immediately (incubator bottles must not be refrigerated)
- Patient instruction: Not applicable (clinician-performed)
Urine
- Mid-stream urine (MSU) — most common
- Patient instruction (written and verbal): retract foreskin/labia, clean with soap and water, discard first and last stream, collect midstream in sterile container
- Catheter specimen: aseptic aspiration from catheter port with a needle (not from bag)
- Transport: refrigerate at 4 °C if delay >1 h; processed within 24 h; use boric acid container to prevent growth during transport if no refrigeration
- Significant bacteriuria: ≥10⁵ CFU/mL of a single organism in asymptomatic patient; ≥10³ CFU/mL in symptomatic catheterised patient
Sputum
- Collect first morning sample — highest mycobacterial yield (pooled overnight secretions)
- Instruct patient: rinse mouth with water (reduces saliva contamination), breathe deeply 3 times, cough from chest, spit sputum (not saliva) into wide-mouthed sterile container
- Induced sputum (for TB): nebulised 5% hypertonic saline — useful when patient cannot expectorate
- Minimum acceptable volume: ≥2 mL
- For routine culture: transport within 2 h; for AFB: can be refrigerated up to 24 h in screw-cap container
Stool
- Fresh stool (walnut-sized, ~5 g) in clean container for routine culture; within 1–2 h
- For transport >2 h: Cary-Blair transport medium (preserves Salmonella, Shigella, Campylobacter)
- Avoid contamination with urine or water
- Rectal swab: only if patient cannot produce stool (neonates); insert 2–3 cm past anal sphincter
- For Clostridium difficile: collect formed stool is NOT acceptable — only liquid stool meets collection criteria
Cerebrospinal Fluid (CSF)
- Collected by physician via lumbar puncture under full sterile technique
- Three sequential numbered tubes: tube 1 (cell count — most likely to be bloody from traumatic tap), tube 2 (glucose/protein), tube 3 (microbiology culture — least chance of skin contamination)
- Volume: minimum 1 mL for culture; more if fungal/AFB suspected (5–10 mL)
- Transport IMMEDIATELY at 37 °C (warm, not refrigerated) — Neisseria meningitidis is exquisitely temperature-sensitive and autolytic; cold kills it in minutes
Wound/Pus
- Aspirate pus with needle and syringe (preferable) rather than swab — larger volume, anaerobes survive better without air exposure
- Surface swab: appropriate for superficial wounds only; clean wound surface first
- Deep tissue biopsy: best specimen for osteomyelitis, deep abscess
- Transport: anaerobic transport system if anaerobes suspected; swab in Stuart's medium within 1–2 h
Throat/Nasopharyngeal Swab
- Depress tongue, rotate swab firmly over both tonsillar fossae and posterior pharynx — avoid saliva, teeth, tongue
- For nasopharyngeal aspirate (viral): insert fine catheter into nasopharynx, aspirate or wash with 1–2 mL saline
- Transport in viral transport medium (for viruses) or Stuart's/Amies (for bacteria)
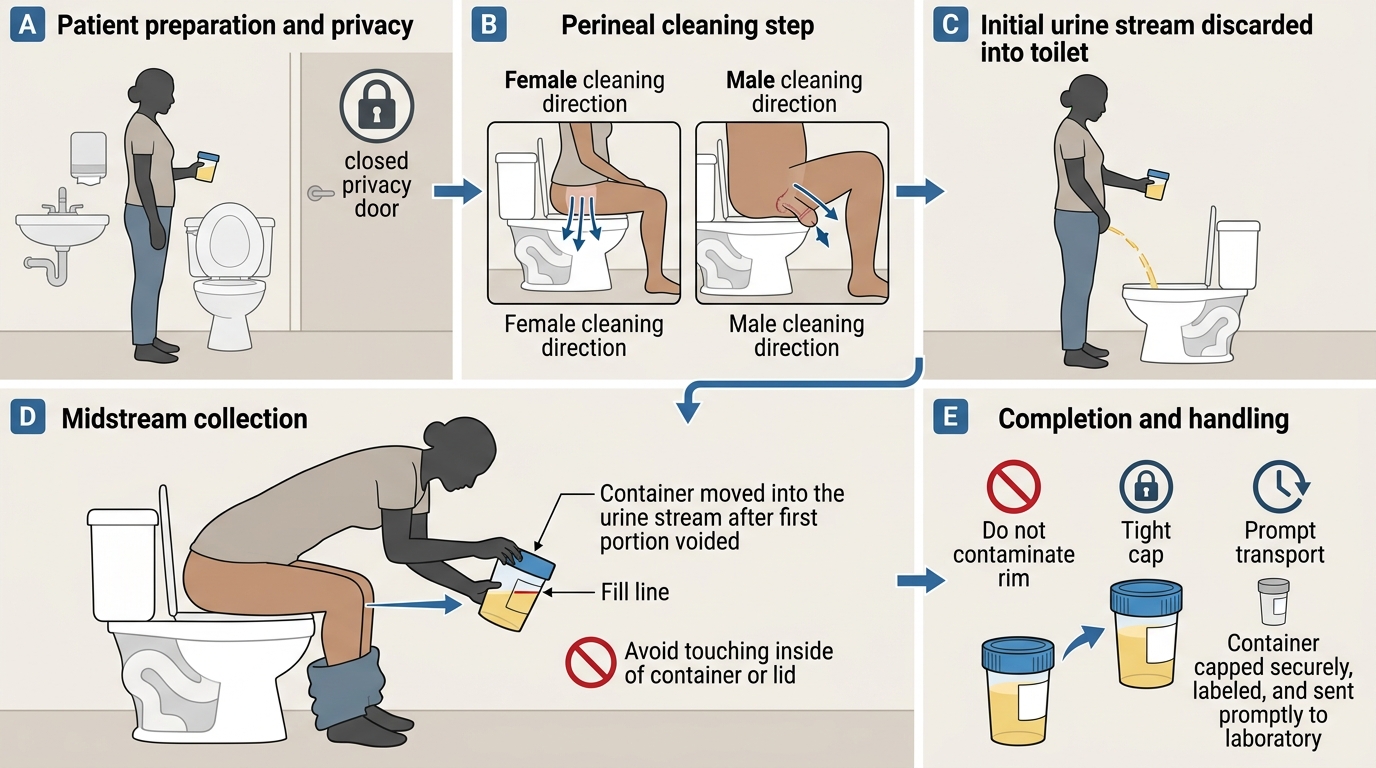
Midstream Clean-Catch Urine Collection Technique

Transport Media Containers and CSF Transport Rule
SELF-CHECK
A patient with suspected meningitis has CSF collected via lumbar puncture. Three tubes are collected. Which tube should be sent for microbiology culture, and at what temperature should it be transported?
A. Tube 1, transported at 4°C to prevent overgrowth
B. Tube 2, transported at room temperature
C. Tube 3, transported immediately at 37°C or room temperature (never refrigerated)
D. Any tube, transported at 4°C in a cold chain
Reveal Answer
Answer: C. Tube 3, transported immediately at 37°C or room temperature (never refrigerated)
Tube 3 is sent for microbiology because it is least likely to be contaminated by skin organisms from the traumatic needle pass (tube 1 picks up the most skin flora and is most likely blood-tinged). CSF must NEVER be refrigerated — Neisseria meningitidis is highly temperature-sensitive and autolytic; cold kills it rapidly, leading to false-negative culture. Transport at 37°C (body temperature in a warm pocket) or at room temperature immediately is the standard.
Epidemiological Basis of Infectious Diseases
Epidemiological Basis of Infectious Diseases
Epidemiology is the study of distribution and determinants of disease in populations. For infectious diseases, it provides the framework to understand why outbreaks occur, who is at risk, and how to intervene.
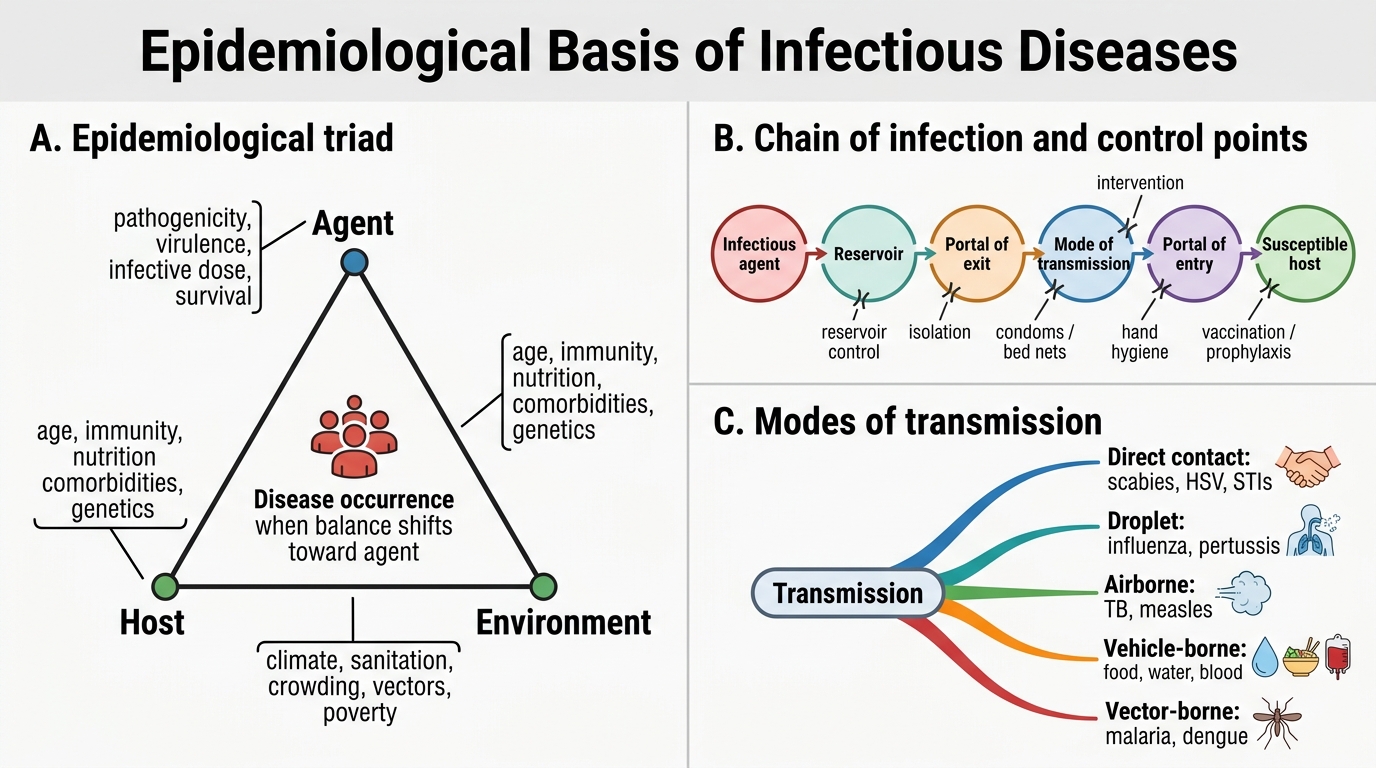
1. The Epidemiological Triad
Three interacting elements determine whether infection occurs:
- Agent: microorganism characteristics — pathogenicity, virulence, infective dose, environmental survival
- Host: susceptibility factors — age, immune status, nutritional status, comorbidities, genetics (HLA type, sickle cell trait)
- Environment: physical (climate, sanitation, overcrowding), biological (vector presence), social (poverty, war, migration)
Disease occurs when the triad is imbalanced in favour of the agent.
2. Chain of Infection
The chain must be unbroken for transmission to occur:
> Infectious Agent → Reservoir → Portal of Exit → Mode of Transmission → Portal of Entry → Susceptible Host
Intervention can break the chain at any link:
- Eliminate reservoir (rodent control for leptospirosis)
- Block portal of exit (isolate infectious TB patient)
- Interrupt transmission (condoms for HIV, bed nets for malaria)
- Close portal of entry (handwashing for faeco-oral diseases)
- Reduce host susceptibility (vaccination, prophylaxis)
3. Modes of Transmission
| Mode | Examples |
|---|---|
| Direct contact | Scabies, herpes simplex, sexually transmitted infections |
| Droplet (>5 µm, <1 m) | Influenza, meningococcal meningitis, pertussis |
| Airborne (<5 µm, long distance) | Pulmonary TB, measles, chickenpox |
| Faeco-oral / vehicle-borne | Typhoid, cholera, hepatitis A, polio |
| Vector-borne | Malaria (Anopheles), dengue (Aedes), plague (Xenopsylla) |
| Blood-borne | HIV, HBV, HCV |
| Vertical (mother to child) | HIV, HBV, rubella, syphilis, CMV |
| Healthcare-associated | MRSA, CRKP — contact transmission within hospitals |
4. Key Epidemiological Measures
- Incidence rate: new cases per population per unit time — measures disease risk
- Prevalence: all existing cases at a point in time — measures disease burden
- Attack rate: proportion of exposed persons who become ill — used in outbreak investigation
- Secondary attack rate: proportion of household contacts who develop disease — measures transmissibility
- Basic reproduction number (R₀): average number of secondary cases from one primary case in a fully susceptible population
- R₀ <1 → epidemic dies out; R₀ >1 → epidemic grows
- Measles R₀ ~12–18; COVID-19 original strain ~2–3; seasonal influenza ~1.2–1.4
5. Herd Immunity and Critical Coverage
When sufficient proportion of a population is immune (by vaccination or prior infection), chain of transmission breaks even for susceptible individuals.
Critical immunisation coverage = 1 − 1/R₀
For measles (R₀ = 15): coverage needed = 1 − 1/15 ≈ 93% — explains why even small gaps in vaccination allow outbreaks.
6. Types of Epidemics
- Common-source outbreak: single exposure event — epidemic curve shows sharp peak, rapid fall (e.g., cholera from contaminated well)
- Propagated (person-to-person) outbreak: gradual rise over successive generations of cases (e.g., measles in a school)
- Zoonotic spillover: animal reservoir → human (H5N1, Nipah, Hendra)
- Endemic: disease consistently present at baseline level in a population (malaria in eastern India)
- Pandemic: worldwide epidemic crossing continental boundaries (COVID-19, 1918 influenza)
7. Outbreak Investigation — Steps (Shoe-leather Epidemiology)
- Confirm the diagnosis
- Confirm the outbreak (compare to baseline)
- Define a case definition
- Count cases and collect descriptive data (person, place, time)
- Identify the source and mode of transmission
- Implement control measures
- Report findings

Epidemic Curves: Common-Source vs Propagated Outbreaks
CLINICAL PEARL
India-specific epidemiology point: India carries the world's highest TB burden (~2.6 million incident cases/year). TB transmission is airborne — a single smear-positive patient may infect 10–15 contacts per year in overcrowded urban settings. This is why sputum collection technique and prompt transport matter at scale: every smear-positive case diagnosed and treated early interrupts dozens of future transmission events.
SELF-CHECK
A food poisoning outbreak affects 80 of 120 people who ate at a community wedding feast. The epidemic curve shows a sharp peak 6 hours after the meal and falls to zero within 24 hours. No secondary cases occur in household contacts of the ill persons. This pattern is most consistent with:
A. A propagated person-to-person outbreak caused by norovirus
B. A common-source outbreak from a contaminated food item at the feast
C. A zoonotic spillover from animals at the feast venue
D. An endemic baseline elevation of food-borne illness in this community
Reveal Answer
Answer: B. A common-source outbreak from a contaminated food item at the feast
The sharp single-peak epidemic curve with incubation of ~6 hours (consistent with Staphylococcal enterotoxin or Bacillus cereus emetic toxin), rapid resolution, and absence of secondary cases in contacts all define a common-source (point-source) outbreak. Propagated outbreaks show successive waves corresponding to serial incubation periods and DO produce secondary cases among household contacts. The attack rate of 67% (80/120) is calculated from exposure at a single shared source.
REFLECT
You are posted in a rural CHC when five children from the same village present within one week with acute watery diarrhoea. Two require IV fluids.
- What specimens would you collect from the children, and how?
- What epidemiological questions would you ask the family to identify the source?
- If the village uses an open well shared by 200 families, what immediate public health action would you initiate?
Consider how your role as a clinician, microbiologist, and public health practitioner overlap in this scenario.
KEY TAKEAWAYS
Key takeaways:
- Specimen quality is non-negotiable — wrong site, inadequate volume, improper transport, or delayed processing can generate false results with direct therapeutic consequences.
- Patient instruction is a clinical skill — written and verbal instructions for midstream urine, sputum collection, and stool sampling reduce pre-analytical errors dramatically.
- Temperature matters at transport — CSF goes warm (gonococci/meningococci die in cold), urine goes cold (bacteria overgrow at room temperature), anaerobic specimens travel in sealed anaerobic transport systems.
- Epidemiology explains the 'why' — the triad of agent, host, and environment determines who gets infected; interventions target weak links in the chain of transmission.
- R₀ and herd immunity thresholds guide vaccination coverage targets — understanding them helps you explain vaccine hesitancy consequences to communities.
- Outbreak investigation is systematic — descriptive epidemiology (person, place, time) and epidemic curve shape distinguish common-source from propagated outbreaks and guide the public health response.