Page 3 of 10
MI1.7-9 | Professionalism: Ethics, Communication & Confidentiality in the Lab — SDL Guide
Learning Objectives
- Demonstrate respectful attitudes and behaviours toward patient samples sent to the microbiology laboratory.
- Demonstrate effective communication skills with patients, relatives, and clinicians during specimen collection and pre/post-test counselling.
- Demonstrate confidentiality of patient identity in laboratory results, including appropriate information-sharing practices.
INSTRUCTIONS
Microbiology is not just about organisms and tests — it is about people. Every specimen you receive carries a patient's identity, anxiety, and trust. How you handle that specimen, how you speak to the patient and their family, and how you share results defines the ethical core of your professional identity. This module uses scenario-based learning to develop attitudes and behaviours that cannot be acquired from textbooks alone. Approach each scenario honestly, not as an exercise in giving the 'correct' answer, but as a rehearsal for who you wish to be as a clinician.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, 10th ed., Ch 11 (Specimen handling, professional aspects) (textbook)
- NMC Attitude, Ethics & Communication (AETCOM) Module 1.1–1.5 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A first-year resident in a busy government hospital in Kolkata receives a urine specimen. The request form reads: 'HIV positive — please test for UTI.' Another resident overhears and calls across the ward: 'Hey, the HIV patient's urine — did you send it?' The patient's wife, seated two metres away, hears every word. She did not know her husband's diagnosis.
In this moment, three unprofessional acts have occurred. Can you name them? And what would the right response look like — before the specimen was even collected?
WHY THIS MATTERS
The attitudes and behaviours you cultivate now will shape thousands of patient interactions across your career. In clinical microbiology, you interact with specimens that are — in law and ethics — extensions of the patient's body and identity. Breaches of dignity and confidentiality in the laboratory cause lasting harm: stigma, family breakdown, employment discrimination, and, in extreme cases, violence against the patient. The NMC AETCOM framework requires demonstrable professional attitudes, not merely stated ones — the clinical microbiology posting is one of the earliest formal assessments of these.
RECALL
From the AETCOM module in Phase 1:
- The doctor-patient relationship is founded on trust, respect, and confidentiality
- Informed consent: the patient has the right to know what tests are being performed and why
- Professional behaviour includes behaviour toward colleagues, support staff, and specimens in the absence of the patient
From General Microbiology I:
- Normal flora vs pathogen: a result only has meaning when interpreted with clinical context — a positive culture without context can harm rather than help
Respect for Patient Samples: Attitudes and Behaviours in the Laboratory
Respectful Handling of Patient Specimens
MI1.7 — Respectful handling of patient specimens
A laboratory specimen is not an anonymous biological material. It is an extension of a person with a name, a family, fears, and dignity.
Behaviours that demonstrate respect:
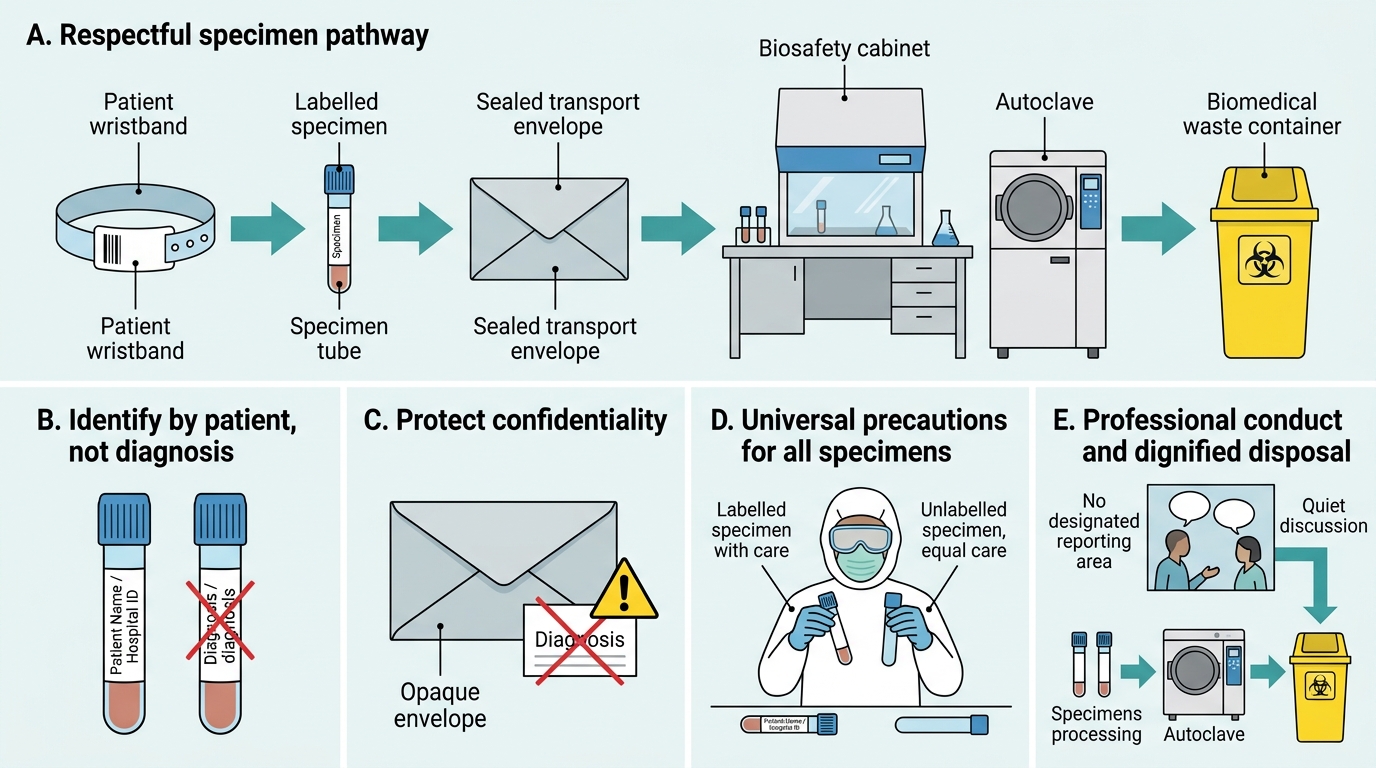
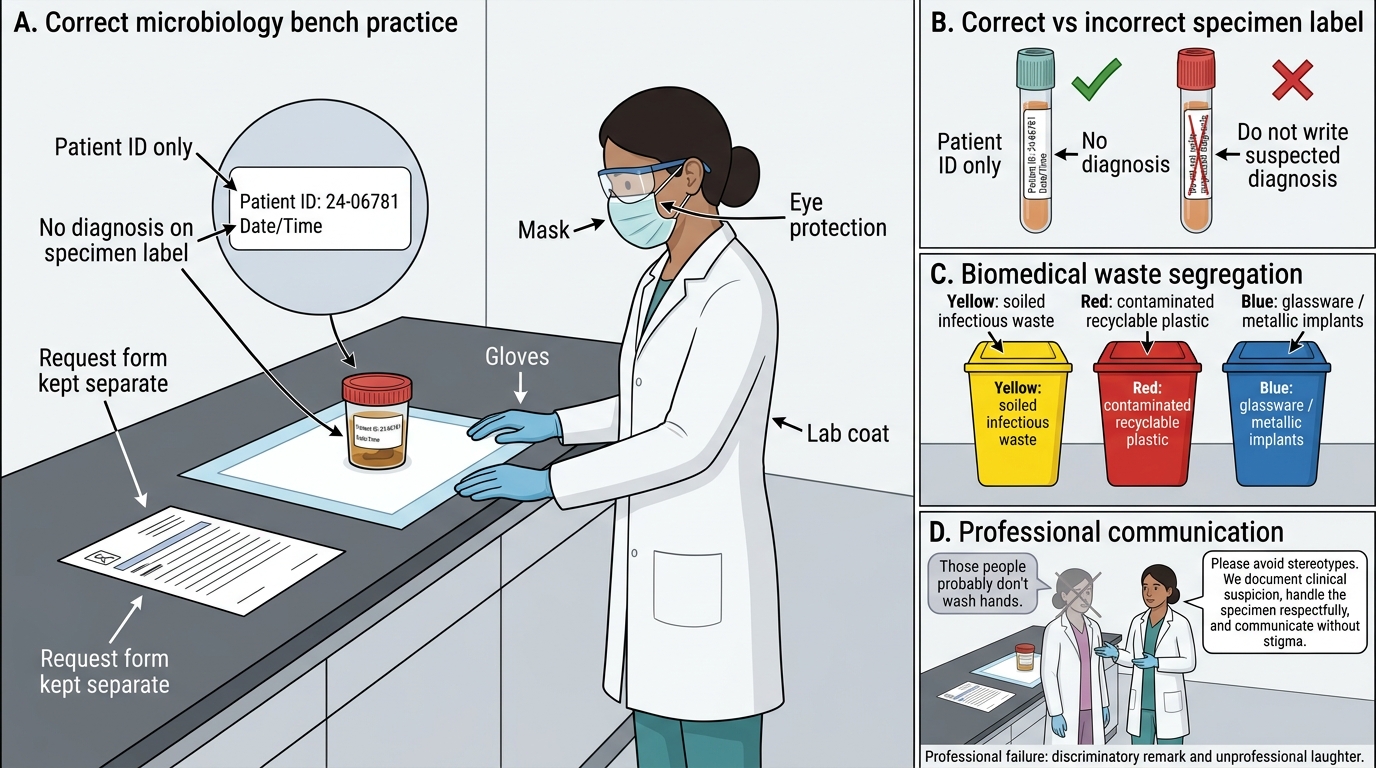
- Use patient identifier, not diagnosis, to refer to specimens. Never 'the HIV swab' or 'the leprosy blood' — always Patient Name / ID. Diagnostic labels on specimens outside sealed envelopes risk disclosure to third parties.
- Handle every specimen with the same care regardless of the diagnosis. A specimen labelled 'HIV positive' or 'Hepatitis B' should not receive slower processing, rough handling, or dismissive comments. Every specimen deserves standard-of-care processing.
- Universal precautions apply universally — not selectively. Wearing gloves and following biosafety protocols for an HIV-labelled specimen but not for an unlabelled one is both medically irrational (any specimen can carry blood-borne pathogens) and ethically discriminatory.
- Verbal conduct in the laboratory. Discussing a patient's specimen loudly in shared spaces, making comments about the patient's lifestyle or diagnosis, or sharing specimen findings informally among staff not involved in the patient's care are all breaches of professional conduct.
- Disposal with dignity. Used specimens must be autoclaved and disposed of as biomedical waste per CPCB Biomedical Waste Rules 2016 — not discarded carelessly, not stored beyond required retention periods.
Specimen Labelling, PPE, Waste Segregation, and Professionalism
Scenario for reflection:
Dr Priya receives a stool specimen from a 70-year-old woman. The request form notes 'suspected cholera — from slum relocation camp.' A colleague says, 'Those people probably don't wash hands.' Dr Priya laughs.
What professional failure has occurred? What should Dr Priya have said instead?
Effective Communication: Patients, Relatives, and Clinicians
Effective Communication During Specimen Collection
MI1.8 — Communication during specimen collection and counselling
Effective communication in the microbiology context occurs at three junctions:
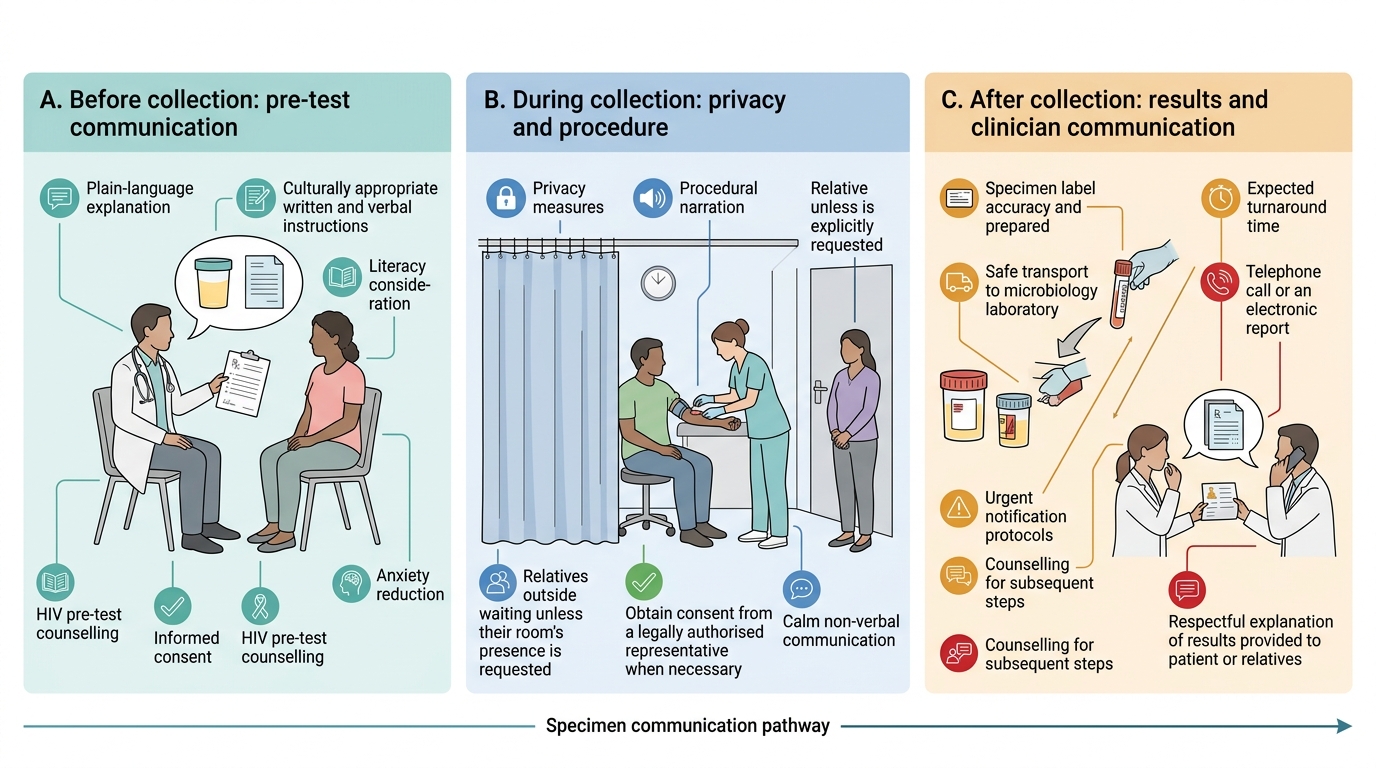
A. Before specimen collection (pre-test communication)
- Explain the purpose of the test in plain language: 'This test will check whether there is a bacterial infection in your urine. The result will help us choose the right medicine.'
- Give clear, culturally appropriate specimen collection instructions (written + verbal; consider literacy level).
- Obtain informed consent where required (HIV testing always requires pre-test counselling per NACO guidelines).
- Address patient anxiety: 'Many patients feel nervous about this — it is a routine test and completely safe.'
B. During specimen collection
- Maintain privacy: draw curtains, close doors, ask accompanying persons to step out unless the patient requests otherwise.
- Communicate procedurally: 'I'm going to clean your arm now. You will feel a small prick. Please stay still for 30 seconds.' Narrating reduces anxiety and unexpected movement.
- Respect bodily autonomy: never collect a specimen from an unconscious or confused patient without the legally authorised representative's consent, except in a genuine medical emergency.
- Non-verbal communication matters: calm body language, avoidance of grimacing at difficult sites or unpleasant specimens.
C. After specimen collection / result communication (post-test counselling)
- Communicate results to the clinician first — unless the patient has direct access to their results through a patient portal, or is independently accessing care.
- When communicating results directly (e.g., in an outpatient rapid-test setting): choose a private space; sit at the same level as the patient; use plain language ('The test shows there is a bacterial infection — the good news is it responds to a common antibiotic').
- HIV post-test counselling: national NACO protocol mandates structured counselling for reactive results — disclosure, partner notification, linkage to ART. As a microbiology resident, you may be present at this disclosure. Never disclose reactive HIV results casually or in public.
- If the patient becomes distressed: pause, offer water, allow silence, and arrange for a counsellor or support person.
Communicating with clinicians:
- Call the clinician immediately for critical values: blood culture positive (first positivity), CSF gram stain positive in suspected meningitis, pandrug-resistant organism detected.
- Use structured communication: SBAR (Situation → Background → Assessment → Recommendation). 'Dr Singh, blood culture from ward 4, Patient Ramesh, bed 12 — grew gram-negative rods flagging as positive at 9 hours. Gram stain shows gram-negative bacilli. Requesting urgent AST and review of empirical cover.'
- Avoid jargon when communicating with paramedical staff collecting specimens.

Confidential HIV Result Counselling and Specimen Labelling
SELF-CHECK
A nurse collects blood from a patient for culture and hands the bottle to the ward helper to deliver to the laboratory. The helper notices the label says 'HIV+ patient — blood culture.' While waiting for the lift, he mentions the patient's name and status to another ward helper. Which ethical principle has been violated, and who bears the primary professional responsibility?
A. Beneficence — the ward helper is primarily responsible
B. Confidentiality — the nurse who wrote the diagnosis on the public label bears primary responsibility
C. Non-maleficence — the laboratory is primarily responsible for not using coded labels
D. Autonomy — the patient is responsible for not requesting a private label
Reveal Answer
Answer: B. Confidentiality — the nurse who wrote the diagnosis on the public label bears primary responsibility
Writing the patient's HIV status on the external label of a specimen bottle — which may be handled by non-clinical staff, visible to others in corridors — is a direct breach of confidentiality. The nurse (or the clinician who completed the request form) bears primary professional responsibility for this disclosure, which was the root cause of the breach. The ward helper's gossip is wrong but secondary. Specimen labels should carry patient ID (name, number) and clinical information needed for laboratory processing — not diagnostic labels that could stigmatise if seen by third parties.
Confidentiality in Laboratory Results
Confidentiality in Laboratory Results
MI1.9 — Protecting patient identity in laboratory results
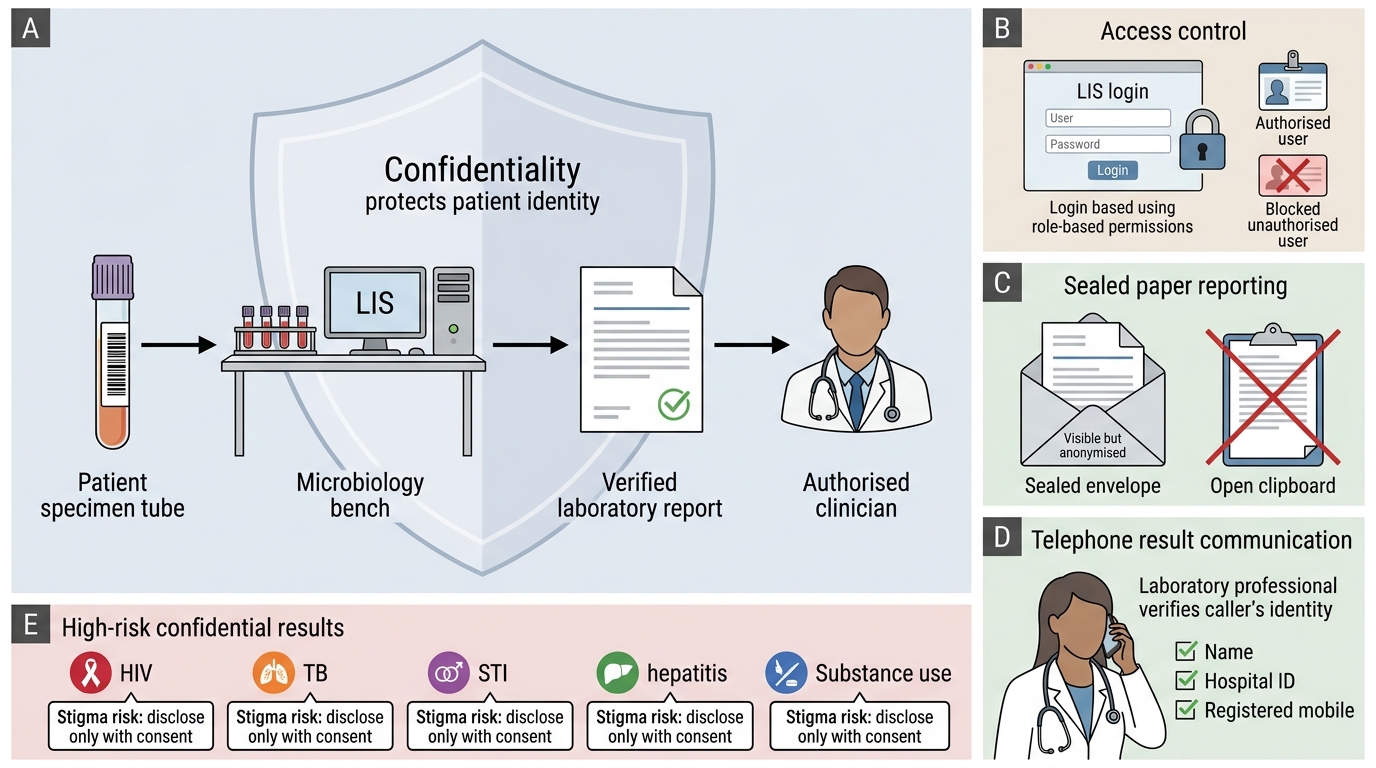
Confidentiality is the obligation to protect identifiable patient information from disclosure without consent. In laboratory medicine, breaches are uniquely dangerous because results often carry stigmatising diagnoses (HIV, TB, STI, hepatitis, substance use).
Legal and regulatory framework in India:
- HIV and AIDS (Prevention and Control) Act, 2017: makes disclosure of HIV status without consent a criminal offence punishable by imprisonment up to 2 years and/or fine.
- Information Technology Act, 2000 (Section 43A): protects sensitive personal data including medical records.
- NMC Code of Ethics 2002 (and revised draft): Clause 7 — 'Secrecy and Confidentiality' — physician must maintain strict secrecy.
- Patient Rights Charter (MoHFW 2019): patients have the right to confidentiality of their health information.
Practical confidentiality protocols in the microbiology laboratory:
- Access control to results: Laboratory information systems (LIS) should restrict result access to authorised users only. Paper results must be placed in sealed envelopes.
- Telephone result communication: Verify caller identity before giving any result over the phone. Use the patient's registered mobile number as secondary verification.
- Electronic reporting: Secure encrypted channels; patient portal access with password protection.
- Physical space: Workstations with patient data should not face common corridors; computers should auto-lock after 2 minutes.
- Incidental findings: If a laboratory test reveals an unexpected stigmatising diagnosis (e.g., a specimen sent for culture grows organisms suggesting an STI the clinician did not suspect), the result goes to the ordering clinician — not to family members, employers, or insurance companies, regardless of who requests it.
- Research and teaching: Patient identifiers must be removed before specimens or results are used for teaching, audit, or research unless informed written consent was obtained.
Exceptions to confidentiality (mandatory reporting):
India's Integrated Disease Surveillance Programme (IDSP) mandates notification of certain communicable diseases:
- Immediate notification: cholera, plague, yellow fever, viral haemorrhagic fevers (within 24 h)
- Weekly notification: dengue, malaria, typhoid, acute hepatitis, pneumonia, diarrhoea
- This statutory obligation overrides individual confidentiality — but reporting goes to public health authorities, not to the general public or patient's employer.
IMPORTANT: Even mandatory reporting should share only the minimum necessary information — name, age, address, diagnosis — not full medical history or other identifiers.

Decision Pathway for Sharing Laboratory Results
CLINICAL PEARL
The 'minimum necessary' principle: When sharing patient information — whether with a consultant, a public health officer, or a medical audit committee — share only the minimum information necessary to achieve the legitimate purpose. Confidentiality is not an absolute barrier (statutory reporting is an exception) but its breaches must always be proportionate, justified, and documented. If in doubt, consult your institution's medical ethics committee or senior consultant before disclosing.
SELF-CHECK
A patient's sputum culture confirms pulmonary tuberculosis. His employer (a school principal) calls the laboratory directly and insists on knowing 'whether this teacher is safe to be around children.' As the laboratory resident on duty, what is the correct action?
A. Confirm the TB diagnosis to the employer since TB is a notifiable disease and the employer has a responsibility to protect children
B. Decline to give any information to the employer and advise them to speak with the patient's treating physician
C. Give the employer a non-identifiable answer: 'All TB patients on treatment are non-infectious after 2 weeks'
D. Ask the employer to submit a written request so the laboratory can decide after consultation
Reveal Answer
Answer: B. Decline to give any information to the employer and advise them to speak with the patient's treating physician
The employer has no legal right to the patient's specific diagnosis. The laboratory must decline to release identifiable diagnostic information to any third party — including employers — without the patient's explicit written consent. TB notification goes to public health authorities (NTEP/IDSP), not employers. The treating physician manages contact tracing and occupational fitness decisions through proper channels. Option C might seem helpful but still risks revealing information indirectly. The correct answer is a courteous but firm refusal and redirection to the treating physician.
REFLECT
Reflect on the following scenario:
You are a second-year resident completing a microbiology posting. A senior colleague asks you to photograph a patient's positive HIV rapid test result card 'for a teaching case.' The result card has the patient's name visible.
- What are the ethical issues?
- What would you do in this moment?
- If you refused and were pressured by the senior colleague, what options do you have?
Now consider: if a photograph was needed for teaching, how could it be obtained ethically?
This scenario has no single correct answer — it asks you to practice ethical reasoning under social pressure, which is a core professional competency.
KEY TAKEAWAYS
Key takeaways:
- Specimens are patients. Every tube, swab, and container in your laboratory represents a person — handle, process, and discuss accordingly.
- Respect means universal precautions universally applied — not just for specimens labelled with stigmatising diagnoses, which is both discriminatory and irrational.
- Communication is a clinical skill. Structured pre-test counselling, procedural narration, and SBAR-style clinician communication reduce errors, build trust, and reduce patient anxiety.
- Confidentiality is legally enforceable in India — especially for HIV (HIV Act 2017), and for all sensitive personal health data (IT Act 2000). Breaches are professional and criminal offences.
- Mandatory reporting is the only legal exception to confidentiality — and only the minimum necessary information goes to statutory public health authorities, not to employers, families, or the public.
- Ethical reasoning under pressure is a lifelong professional practice. When in doubt: pause, consult, document. The minimum necessary principle guides information sharing.