Page 2 of 9
MI10.3-4 | Biomedical Waste, PPE & Microbial Surveillance — SDL Guide
Learning Objectives
- Demonstrate hand washing, donning and doffing of PPE and segregation of biomedical waste according to Indian guidelines
- Describe the methods used and significance of assessing microbial contamination of food, water and air in hospital surveillance settings
INSTRUCTIONS
Biomedical waste management and PPE use are not bureaucratic checklists — they are the practical expression of everything you have learned in infection control. India's Biomedical Waste Management Rules 2016 have legal teeth: hospitals face penalties for non-compliance. This SDL prepares you for the OSPE station that will test your ability to actually demonstrate hand hygiene, PPE donning/doffing and waste segregation.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 14 (Sterilisation, Disinfection and Infection Control) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
During the COVID-19 pandemic, a tertiary care hospital in Chennai experienced an outbreak of COVID-19 among its own nursing staff. Investigation found that many nurses were removing their N95 masks before fully leaving the patient's room, and PPE kits were being shared between shifts. Three nurses were hospitalised. What PPE errors occurred? What is the correct sequence for removing PPE (doffing) to prevent self-contamination? How could this outbreak have been prevented with proper training?
WHY THIS MATTERS
Each year in India, ~3 million healthcare workers sustain needle-stick injuries — 30% leading to HBV, 3% to HCV and 0.3% to HIV transmission. Improper biomedical waste (BMW) disposal in India leads to thousands of infections annually among rag-pickers, municipal waste workers and community members. The Biomedical Waste Management Rules 2016 (amended 2018, 2019) impose criminal liability on healthcare institutions and workers. As an intern and future clinician, you will be responsible for your own compliance.
RECALL
Before proceeding, recall: (1) Hierarchy of controls for infectious exposure risk: Elimination → Substitution → Engineering controls → Administrative controls → PPE (last resort, but most visible). (2) Principle of sequential PPE removal (doffing): Remove most contaminated items first (gloves, gown) before least contaminated (mask, eye protection). (3) BMW Rule 2016: BMW is classified into 10 categories with specific bag colour-coding for segregation at the point of generation. (4) Standard precautions: PPE is part of standard precautions — not just for infectious patients.
Hand Hygiene — Technique and When-to-Wash (MI10.3)
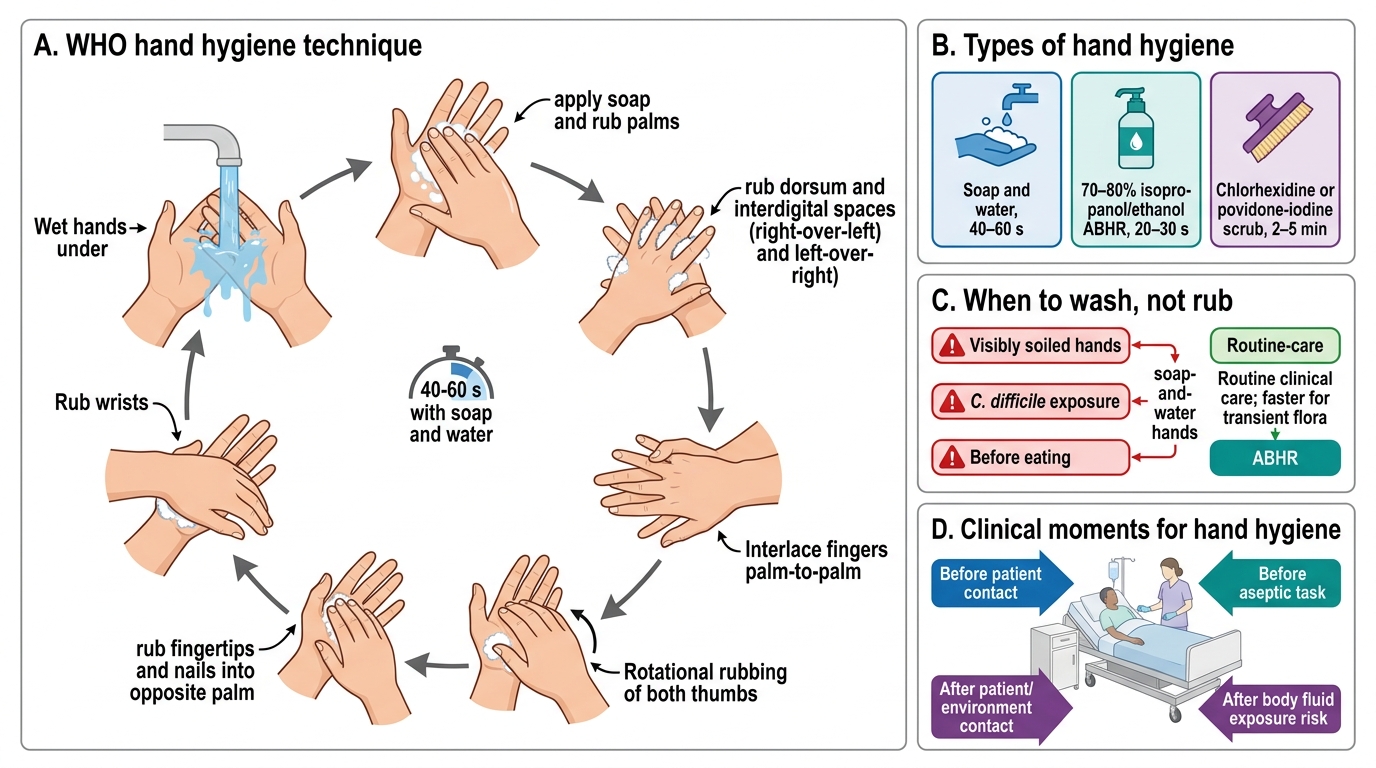
Hand Hygiene Technique and When-to-Wash
Hand hygiene types:
| Type | Method | Duration | When Used |
|---|---|---|---|
| Hand washing | Soap and water | 40–60 seconds | Visibly soiled hands; C. difficile exposure; before eating |
| Alcohol-based hand rub (ABHR) | 70–80% isopropanol/ethanol | 20–30 seconds | Routine clinical care (faster, more effective for transient flora) |
| Surgical hand antisepsis | Chlorhexidine or povidone-iodine scrub | 2–5 minutes | Before any surgical/invasive procedure |
WHO 11-step handwashing technique (adapted for clinical practice):
1. Wet hands under running water
2. Apply soap; rub palms together
3. Rub backs of hands and interdigital spaces (right over left; left over right)
4. Rub interlaced fingers (both directions)
5. Rub thumbs (rotational, both)
6. Rub fingertips and nails into opposite palm
7. Rub wrists
8. Rinse thoroughly under running water
9. Dry with single-use paper towel
10. Use towel to turn off tap (avoid recontamination)
Critical points: Remove jewellery and watches before hand hygiene. Artificial nails and chipped nail polish harbour more transient organisms and are prohibited in clinical areas. Gloves do NOT replace hand hygiene — gloves can tear or become contaminated externally.
Personal Protective Equipment (PPE) — Donning and Doffing
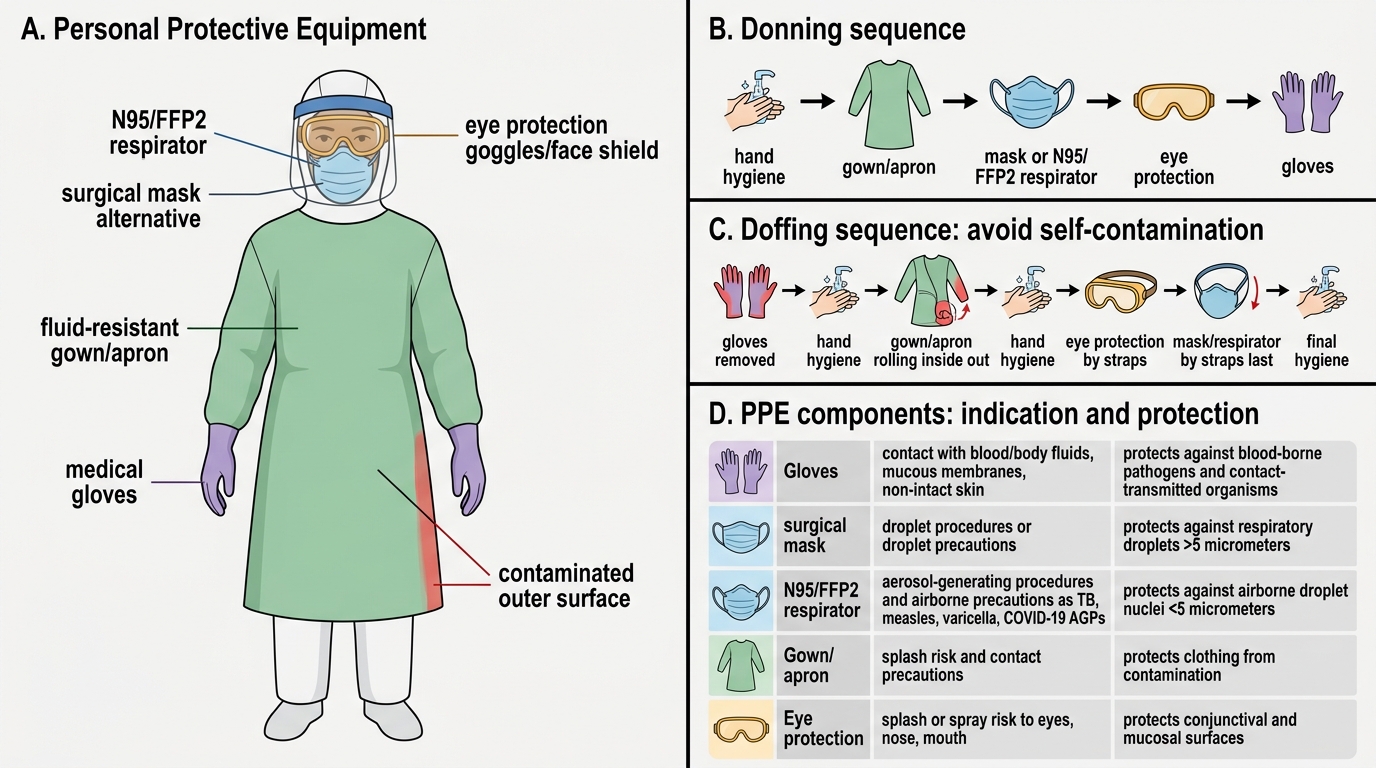
PPE Components, Indications, Donning and Doffing
Standard PPE components and indication:
| Component | Indication | Protects against |
|---|---|---|
| Gloves | Contact with blood/body fluids, mucous membranes, non-intact skin | Blood-borne pathogens, contact-transmitted organisms |
| Surgical mask | Droplet-generating procedures, droplet precautions | Respiratory droplets >5 µm |
| N95/FFP2 respirator | Aerosol-generating procedures (AGPs); airborne precautions (TB, measles, varicella, COVID-19 AGPs) | Airborne droplet nuclei <5 µm |
| Gown/apron | Splash risk; contact precautions | Contamination of clothing |
| Eye protection (goggles/face shield) | Splash/spray risk to eyes, nose, mouth | Conjunctival/mucosal exposure |
DONNING order (put on): Hand hygiene → Gown → Mask/respirator (fit check for N95) → Eye protection → Gloves (glove cuffs over gown cuffs)
DOFFING order (remove) — critical sequence to prevent self-contamination:
1. Gloves — outside of gloves is contaminated; remove by 'glove-into-glove' technique; hand hygiene
2. Eye protection — handle by ear-pieces or headband (outside is contaminated)
3. Gown — unfasten ties; roll inside-out; avoid contact with outer surface
4. Mask/respirator — handle by ties/ear loops only; do NOT touch front face piece; hand hygiene
5. Final hand hygiene

PPE Donning, Doffing, and Exposure Safety
N95 Fit Check:
- Positive pressure check: Block exhalation valve and exhale gently; mask should bulge without air leaking
- Negative pressure check: Block inhalation ports and inhale gently; mask should collapse without air leaking
- Fit testing (quantitative/qualitative) — mandatory annually for HCWs using respirators in high-exposure settings
CLINICAL PEARL
Needle-stick injury protocol (Post-Exposure Prophylaxis — PEP):
1. Immediately squeeze wound to bleed; wash with soap and water for 10 minutes; do NOT suck the wound
2. Report to Occupational Health / Infection Control Nurse within 1 hour
3. Assess source patient's HIV/HBV/HCV status
4. If HIV risk: Start triple-drug ART PEP within 2 hours (ideally), no later than 72 hours; 28-day course
5. If HBV risk (unvaccinated recipient): HBIG + HBV vaccine within 7 days
6. Document; follow up at 6 weeks, 3 months, 6 months
In India, this is covered under the NACP PEP guidelines. HCWs must be vaccinated against HBV (3-dose course) before starting clinical postings — this is a national mandate.
Biomedical Waste (BMW) Management — Indian Guidelines (MI10.3)
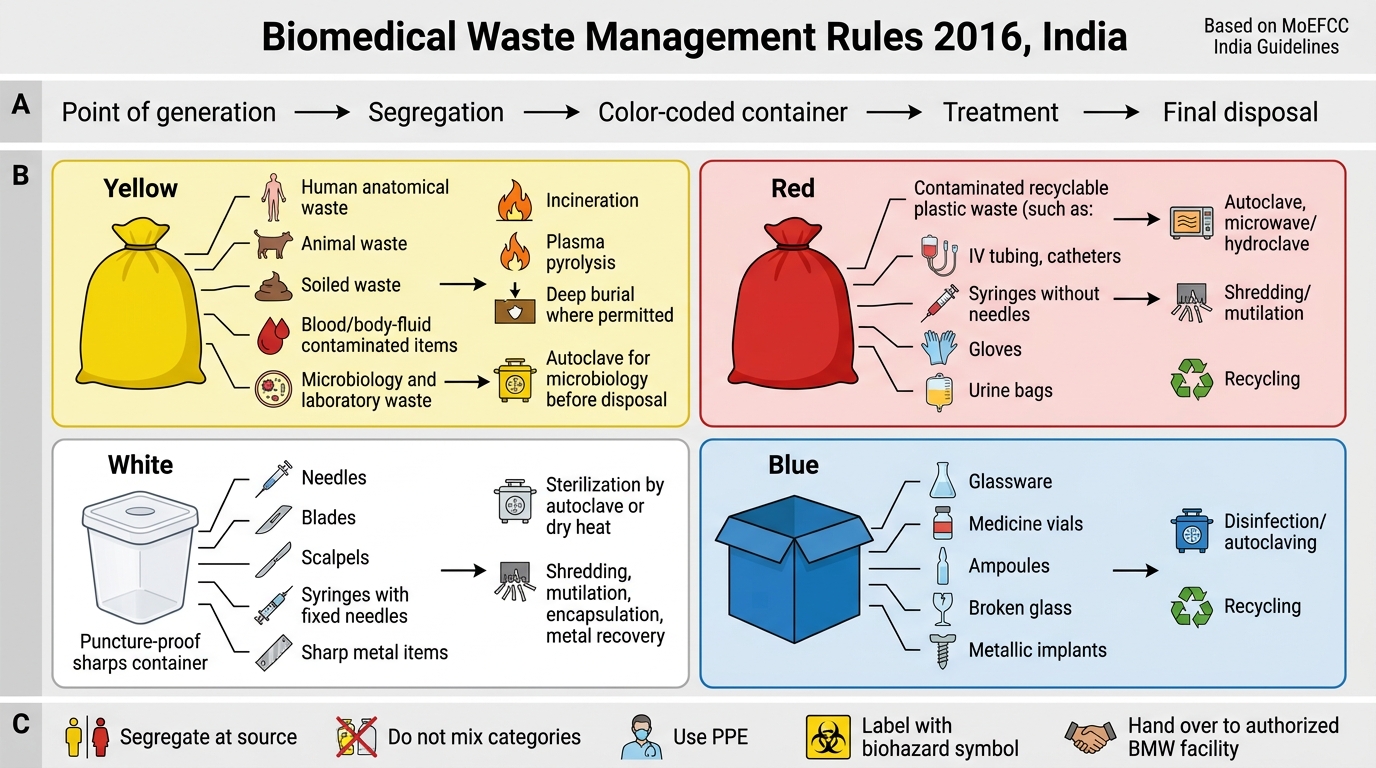
Biomedical Waste Management: Indian BMW Rules 2016
Biomedical Waste Management Rules 2016 (BMW Rules 2016), MoEFCC, India:
BMW is classified into 4 categories (post-2016 revision) with corresponding bag colours:
| Category | Waste Type | Bag/Container Colour | Treatment/Disposal |
|---|---|---|---|
| Category 1 | Human anatomical waste (body parts, organs, tissues); animal waste | Yellow bag | Incineration |
| Category 2 | Soiled waste — blood-soaked items, dressings, linen; body fluid items; laboratory waste (cultures, blood); isolation waste | Yellow bag | Incineration or autoclave + shredding + burial |
| Category 3 | Sharps — needles, syringes, blades, broken glass with sharp edges | White translucent puncture-proof container (sharps bin) | Autoclaving/dry heat + shredding + encapsulation |
| Category 4 | Discarded/expired medicines (cytotoxic in yellow, pharmaceuticals in blue) | Blue bag (non-cytotoxic); Yellow bag (cytotoxic) | Return to manufacturer or incineration (cytotoxic) |
Additional waste streams:
- General solid waste (Category 5/MSW-like): Packaging, wrappers, kitchen waste → Black bag (municipal solid waste)
- Chemical/liquid waste: Disinfectants, lab reagents → ETP (Effluent Treatment Plant)
- Radioactive waste: Separate protocol under AERB
Key principles:
- Segregation at the point of generation — the treating doctor/nurse is responsible
- Do NOT overfill bags beyond 3/4 capacity
- Double-bag highly infectious material
- Label all containers (name, ward, date)
- Never recap needles (use one-hand scoop technique if unavoidable)
- Authorised treatment facility (CBWTF) — licensed Central Biomedical Waste Treatment Facility must be used; most hospitals use outsourced CBWTF
- Bar coding of BMW bags (2019 amendment) for tracking
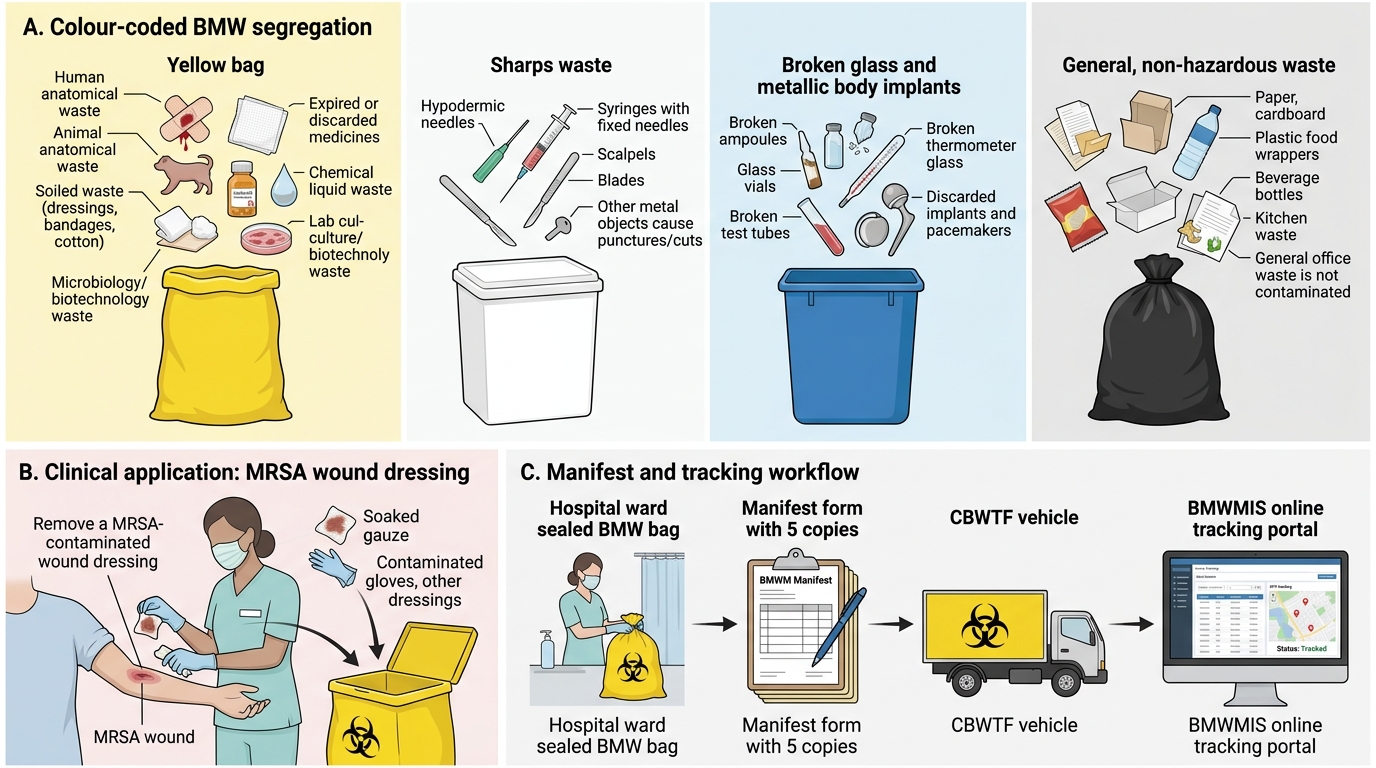
Colour-Coded BMW Segregation and Manifest Workflow
Biomedical Waste Manifest:
Every consignment of BMW to CBWTF must be accompanied by a manifest form — 5 copies; tracked online (Bio-Medical Waste Management Information System — BMWMIS portal).
SELF-CHECK
A nurse finishes changing a wound dressing on a patient with a MRSA surgical site infection. The used dressing, soaked gauze and gloves should be disposed of in which colour of BMW bag?
A. Black bag (general solid waste)
B. Blue bag (pharmaceutical waste)
C. Yellow bag (soiled/infectious waste — Category 2)
D. White puncture-proof container (sharps)
Reveal Answer
Answer: C. Yellow bag (soiled/infectious waste — Category 2)
Blood/body fluid-soaked items, used dressings, gauze and gloves contaminated with infectious material (including MRSA) fall under BMW Category 2 (soiled waste). These go into the YELLOW bag for incineration or autoclave + shredding. Black bags are for general non-infectious waste; sharps go into white puncture-proof containers; blue bags are for pharmaceutical waste.
Microbial Surveillance of Food, Water and Air (MI10.4)
Microbial Surveillance of Hospital Food, Water and Air
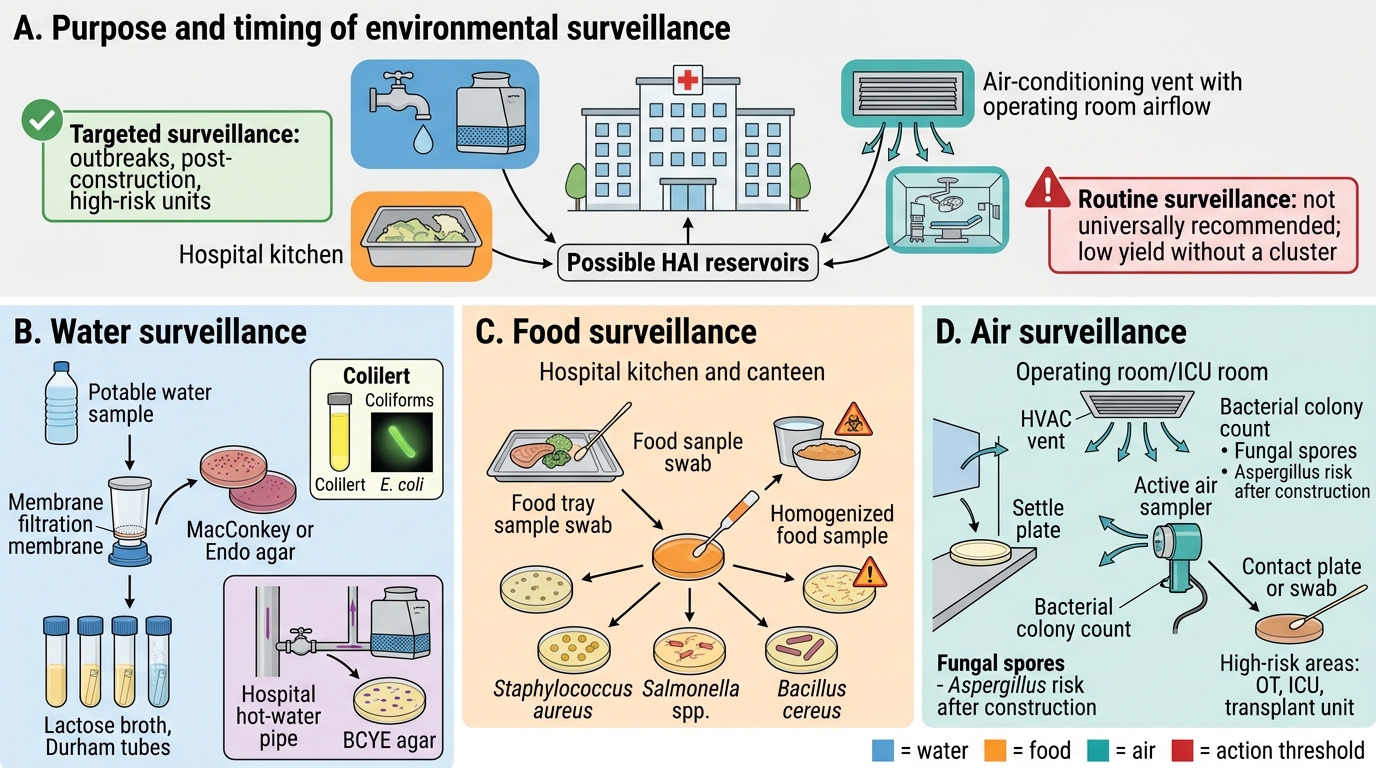
Purpose of hospital environmental surveillance:
To detect unsuspected reservoirs of HAI-related organisms, verify decontamination efficacy, and investigate outbreaks. Routine environmental surveillance is NOT universally recommended (low yield without a cluster); targeted surveillance during outbreaks or post-construction is evidence-based.
1. Water Surveillance:
Potable water (drinking):
- Indicator organisms: Escherichia coli and total coliforms (indicate faecal contamination)
- Methods:
- Membrane filtration (most sensitive): Water filtered through 0.45 µm membrane; membrane placed on selective agar (MacConkey/Endo); count colonies
- Multiple Tube Fermentation (Most Probable Number — MPN): Serial dilutions in lactose broth; gas production in Durham tube = presumptive positive; confirmed by subculture
- Whirlpool procedure (Colilert): Chromogenic ONPG/MUG media — yellow = coliform; fluorescent = E. coli
- Standard (BIS/WHO): Zero E. coli / 100 mL (drinking water)
Legionella in hospital water (cooling towers, hot water systems):
- Culture on BCYE agar (buffered charcoal yeast extract); water sample + pre-treatment (acid wash or heat)
- PCR for Legionella pneumophila
- Action level: >1,000 CFU/L in non-clinical areas; >100 CFU/L in clinical areas
2. Food Surveillance:
- Purpose: Detect foodborne pathogen contamination in hospital kitchen/canteen
- Organisms tested: Total plate count, coliforms, S. aureus, Salmonella, Bacillus cereus
- Methods:
- Dilute food sample in peptone water → plated on selective/non-selective agar
- S. aureus on Baird-Parker agar (black shiny colonies with opaque halo)
- Salmonella/Shigella on MacConkey + XLD agar; confirmed by biochemical + serology
- B. cereus on PEMBA agar (purple/peacock blue colonies)
- Stool culture from food handlers — mandatory if a foodborne outbreak is suspected; carriers of Salmonella typhi must be removed from food handling duties
3. Air Surveillance:
Settle plate method (passive — most widely used in India):
- 90 mm blood agar/nutrient agar plates exposed for a defined period (5–15 min) at height 1 m
- Colony count after 24–48 hr incubation
- Interpretation: <5 CFU/plate (clean area); <1 CFU/plate (laminar flow OT)
Active air sampling (impaction method):
- RCS centrifugal sampler or Anderson cascade impactor — draws known volume of air; organisms impacted on nutrient agar
- Expressed as CFU/m³
Standards:
- Operating theatre (OT): <10 CFU/m³ (air-conditioned conventional) or <1 CFU/m³ (ultraclean laminar flow OT for orthopaedics/transplant)
- ICU: <35 CFU/m³
- HEPA filtration and UV germicidal irradiation used to reduce airborne contamination
Organisms of concern in hospital air:
- Aspergillus spores — construction/renovation activates soil spores → invasive aspergillosis in neutropenic patients (major outbreak risk)
- Staphylococcus aureus — shed from colonised HCWs
- Mycobacterium tuberculosis — negative pressure rooms must be verified by air sampling if outbreak is suspected
SELF-CHECK
A 55-year-old patient undergoing bone marrow transplantation develops fever and right upper lobe pulmonary infiltrates 2 weeks post-transplant. The hospital has been undergoing renovation works adjacent to the transplant unit. Which environmental surveillance method is most relevant to investigate the likely source?
A. Water culture for Legionella in cooling towers
B. Stool cultures from cafeteria workers
C. Air sampling for fungal spores (settle plate or active impaction sampling)
D. Surface swabs from ICU bedside rails
Reveal Answer
Answer: C. Air sampling for fungal spores (settle plate or active impaction sampling)
Construction/renovation near immunocompromised wards is a well-recognised risk factor for invasive pulmonary aspergillosis. Disturbed soil and construction dust release Aspergillus fumigatus spores into hospital air. Air sampling (settle plates or active impaction sampling using RCS/Anderson samplers) is the relevant investigation to quantify airborne fungal spore burden and confirm the source. HEPA-filtered positive-pressure rooms during construction and sealing of ventilation ducts are mandatory protective measures.
REFLECT
You are the intern on duty in the surgical ward when you realise that all the BMW bags in the dressing trolley room are overflowing — yellow, black and white containers are intermixed, with sharps visible in a yellow bag. The ward ayah says she was not trained on segregation. What do you do immediately? What are your responsibilities as a healthcare team member? How does this connect to the legal framework of BMW Rules 2016?
KEY TAKEAWAYS
Hand hygiene (WHO 11-step technique, 40–60 sec with soap or 20–30 sec with ABHR at the 5 Moments) is the single most effective HAI prevention measure — alcohol-based hand rub is standard; soap-and-water mandatory for C. difficile. PPE donning/doffing follows a defined sequence: Gown → Mask → Eyes → Gloves (on); Gloves → Eyes → Gown → Mask (off) — touching only the non-contaminated surfaces during removal. BMW Management Rules 2016 mandates colour-coded segregation at the point of generation: Yellow (anatomical + soiled + infectious), White translucent puncture-proof (sharps), Blue (pharmaceutical), Black (general MSW). Hospital environmental surveillance targets food (MPN/membrane filtration for coliforms), water (coliform culture, Legionella on BCYE), and air (settle plates, active impaction sampling — especially for Aspergillus in construction settings affecting immunocompromised patients). These are not passive administrative tasks — they are active, skills-based, legally mandated clinical competencies.