Page 1 of 9
MI10.{1-2,5} | HAI: Types, Causative Agents & Infection Control — SDL Guide
Learning Objectives
- Define HAI and enumerate different causative agents and types of Healthcare-Associated Infections
- Describe the chain of HAI transmission and its role in prevention
- Describe standard and transmission-based precautions for infection control and the role of the Hospital Infection Control Committee (HICC)
- Describe the mechanisms of evolution, spread and control of antimicrobial drug resistance in hospitalised patients
INSTRUCTIONS
Healthcare-Associated Infections (HAIs) are acquired by patients during the process of receiving healthcare, and they represent a global crisis — killing ~1.4 million people daily worldwide. In India, HAI rates in ICUs can be 3–5 times higher than in high-income countries. Every doctor contributes to infection control — this is not just an infectious disease specialty topic.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 12 (Hospital Infections, Antimicrobial Resistance), Ch 14 (Disinfection and Sterilisation) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 62-year-old patient admitted to the ICU for cardiac surgery develops fever and rigors on day 5 post-operatively. Blood culture grows a Gram-negative rod that is resistant to carbapenems. The infection control nurse notes that 3 other ICU patients developed similar infections in the same week from a shared ventilator circuit. The hospital's HICC convenes an emergency meeting. What organism is most likely? What is the chain of transmission in this outbreak? What immediate measures should the HICC order?
WHY THIS MATTERS
HAIs increase hospital stay by 5–10 days, double mortality risk, and add enormous financial burden. In Indian tertiary care ICUs, Ventilator-Associated Pneumonia (VAP) occurs at rates of 10–25 per 1,000 ventilator days — far above global benchmarks. Antimicrobial-resistant organisms (MRSA, carbapenem-resistant Klebsiella, Acinetobacter) make HAIs nearly untreatable. As a future clinician, your hand hygiene and aseptic technique compliance are the single most cost-effective infection control interventions available.
RECALL
Before proceeding, recall: (1) Definition: HAI = an infection that was not present or incubating at the time of admission, and develops ≥48 hours after hospital admission (or within 30 days of a surgical procedure). (2) The chain of infection: Infectious agent → Reservoir → Portal of exit → Mode of transmission → Portal of entry → Susceptible host. (3) Nosocomial is a synonym for healthcare-associated. (4) Normal flora vs transient flora on hands — transient flora (Staphylococcus, Gram-negatives acquired during patient contact) is the main HAI transmission vehicle.
Types of HAI and Their Causative Agents (MI10.1)
Major Healthcare-Associated Infections and Causative Agents
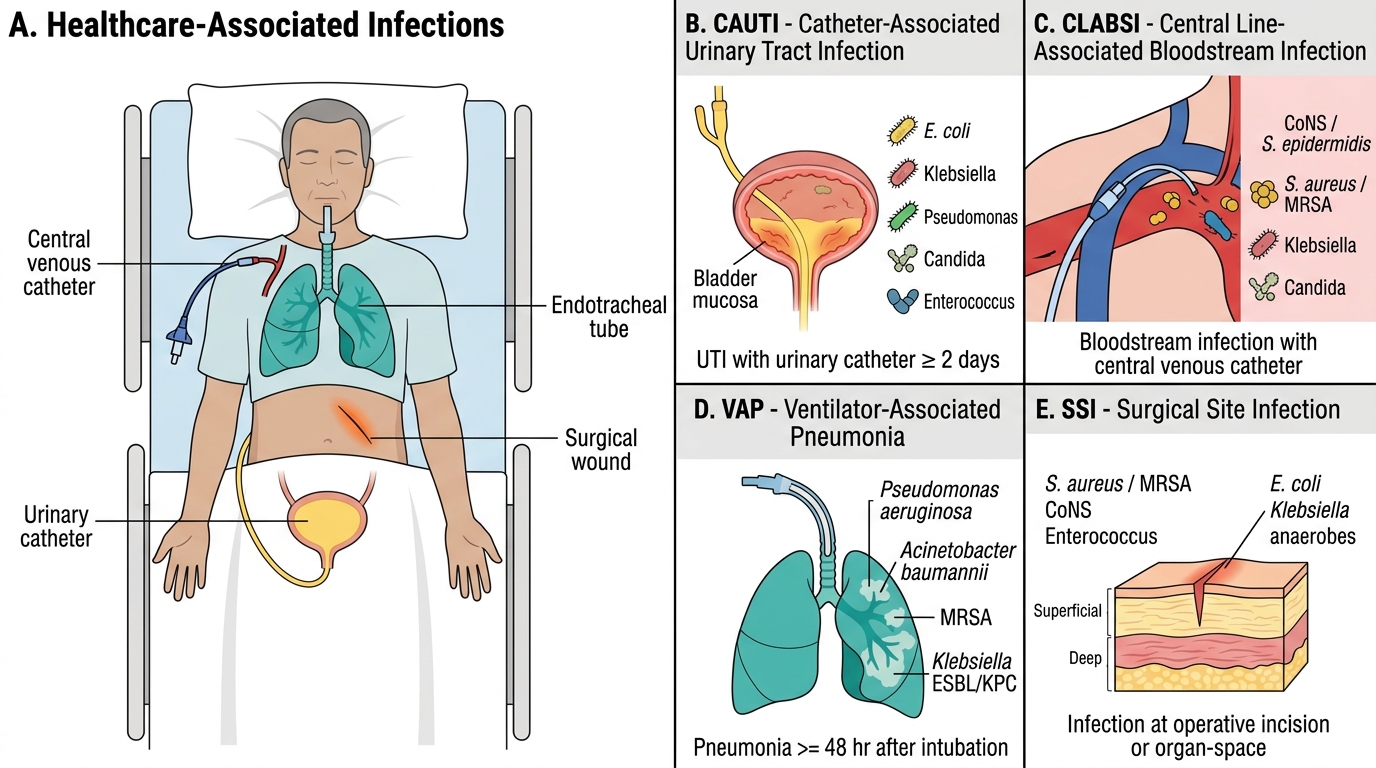
Major HAI types by site (CDC definitions):
| HAI Type | Abbreviation | Definition | Major Causative Agents |
|---|---|---|---|
| Catheter-Associated Urinary Tract Infection | CAUTI | UTI in a patient with urinary catheter ≥2 days | E. coli, Klebsiella, Pseudomonas, Candida, Enterococcus |
| Central Line-Associated Bloodstream Infection | CLABSI | Bloodstream infection in patient with central venous catheter | CoNS (S. epidermidis), S. aureus (MRSA), Klebsiella, Candida |
| Ventilator-Associated Pneumonia | VAP | Pneumonia ≥48 hr after endotracheal intubation | Pseudomonas aeruginosa, Acinetobacter baumannii, MRSA, Klebsiella (ESBL/KPC) |
| Surgical Site Infection | SSI | Infection at operative site within 30 days (1 year for implants) | S. aureus (MRSA), E. coli, Klebsiella, anaerobes (deep SSI) |
| Clostridioides difficile Infection | CDI | Diarrhoea after antibiotic use; toxin A/B positive | Clostridioides difficile (spore-forming anaerobe) |
Device-related HAIs (CAUTI, CLABSI, VAP) are the most targetable via bundle care.
Other HAIs: Bloodstream infections (BSI), pneumonias (non-VAP), GI infections (C. difficile, rotavirus in paediatric wards), meningitis (post-neurosurgery).
Chain of HAI Transmission and Breaking the Chain
Chain of Healthcare-Associated Infection Transmission
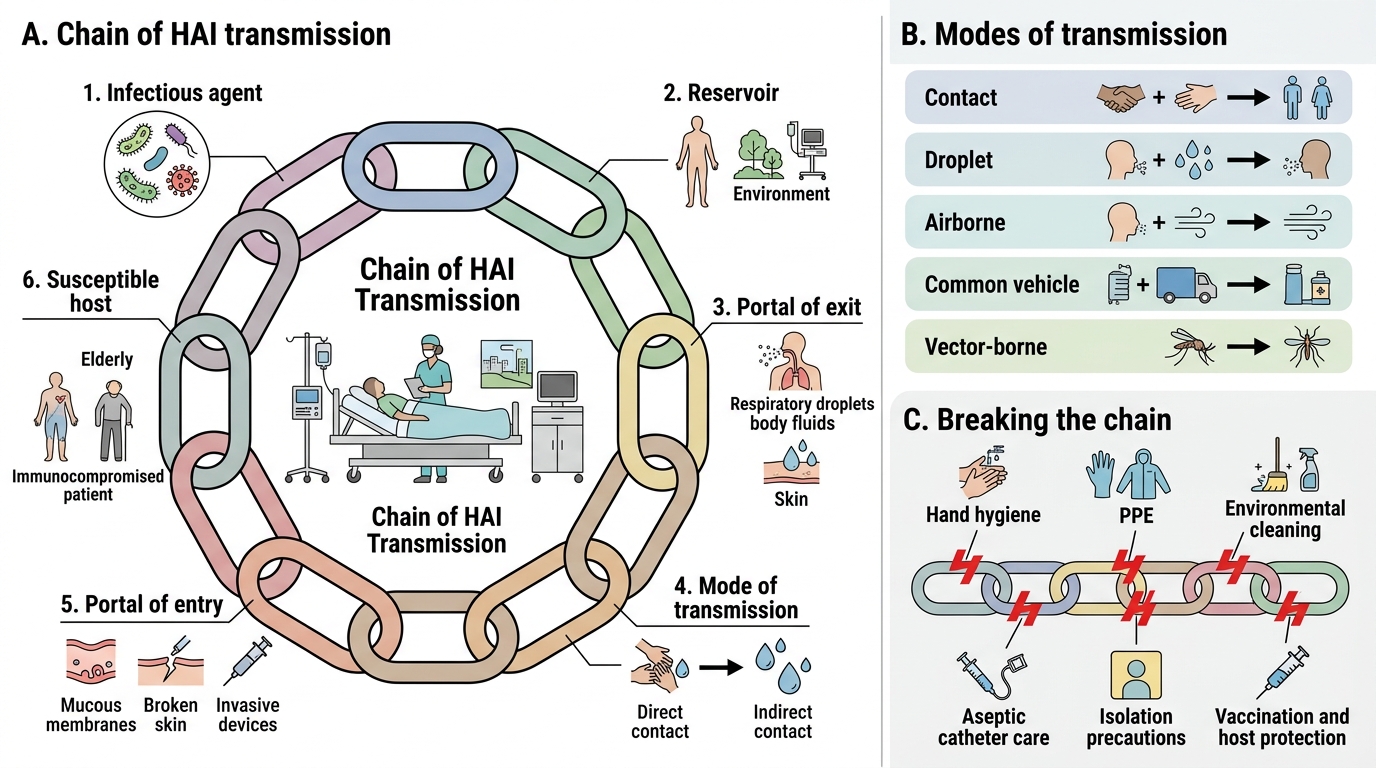
Chain of Transmission in HAI:
1. Infectious Agent: MRSA, carbapenem-resistant Acinetobacter (CRAB), Pseudomonas, Klebsiella, ESBL producers, C. difficile, HBV, HCV, Norovirus
2. Reservoir: Colonised/infected patient, healthcare worker (HCW) hands, environment (bed rails, call buttons, stethoscopes), contaminated equipment (ventilator circuits, catheters)
3. Portal of Exit: Respiratory secretions, blood, urine, wound exudate, faeces
4. Mode of Transmission:
- Contact (most common): Direct (HCW hands) or Indirect (contaminated surfaces)
- Droplet (>5 µm, travels <1 m): Influenza, S. aureus
- Airborne (<5 µm, remains suspended): TB, measles, varicella
- Common vehicle: Contaminated IV fluids, blood products
- Vector-borne: Rare in hospital settings
5. Portal of Entry: IV insertion sites, urinary catheter, surgical wound, respiratory tract (ventilated patients)
6. Susceptible Host: ICU patients, post-surgical, immunocompromised, neonates, elderly
Breaking the chain: Each link is a target for infection control.

Chain of Infection Transmission in Healthcare-Associated Infections
CLINICAL PEARL
WHO '5 Moments of Hand Hygiene' targets the most common chain-break opportunity:
1. Before touching a patient
2. Before a clean/aseptic procedure
3. After body fluid exposure risk
4. After touching a patient
5. After touching patient surroundings
Compliance in Indian hospitals averages 30–40%. Each 10% increase in compliance reduces HAI rates by ~5%. Alcohol-based hand rub (ABHR) is faster and more effective than soap-and-water for non-spore-forming organisms; soap-and-water is MANDATORY for C. difficile (spores resist alcohol).
Standard and Transmission-Based Precautions (MI10.2)
Standard and Transmission-Based Precautions
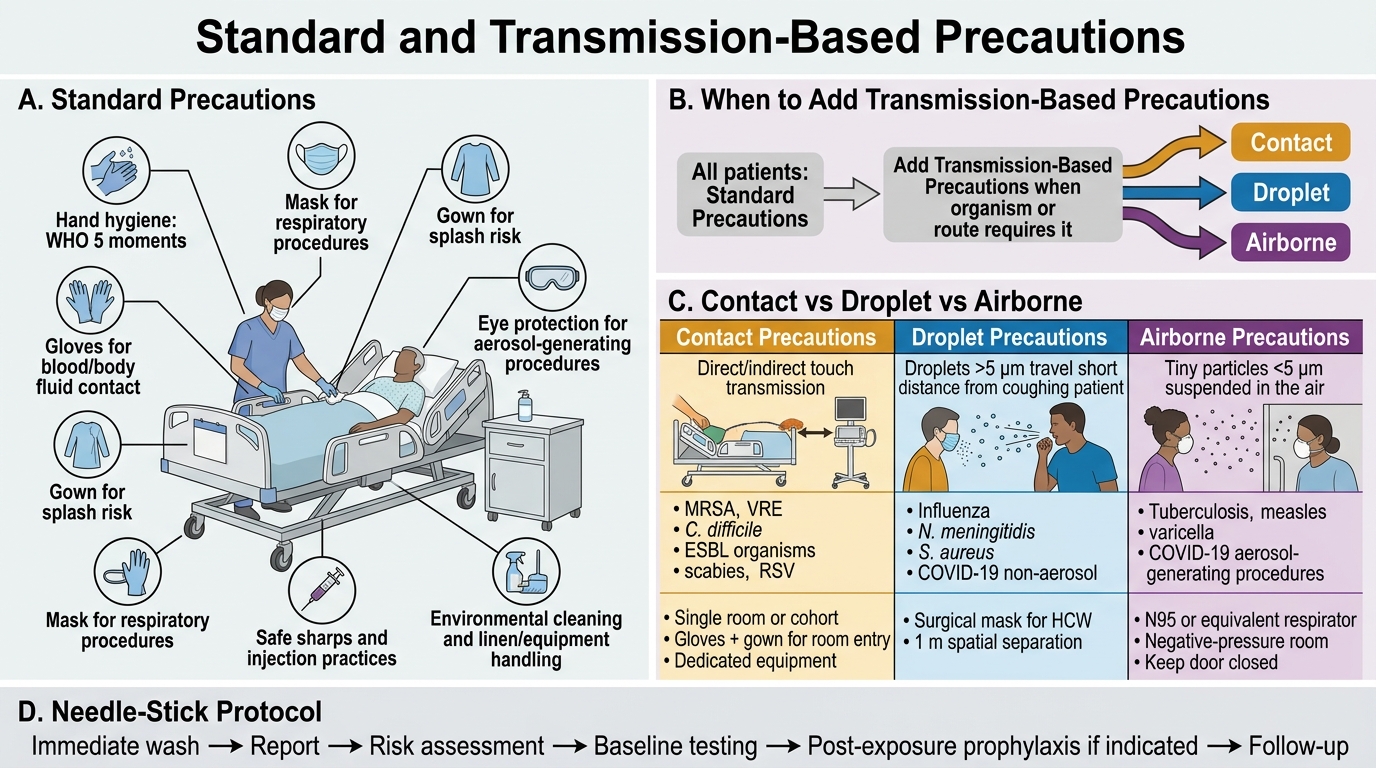
Standard Precautions (applied to ALL patients, regardless of diagnosis):
- Hand hygiene (WHO 5 moments)
- PPE: gloves (any blood/body fluid contact), mask (respiratory procedures), gown (splash risk), eye protection (aerosol-generating procedures)
- Safe needle/sharps handling; needle-stick protocol
- Safe injection practices (single-use syringes/needles)
- Respiratory hygiene/cough etiquette
- Environmental cleaning and linen handling
- Safe handling of potentially contaminated equipment/surfaces
Transmission-Based Precautions (added to standard precautions for specific organisms):
| Precaution Type | Transmission Route | Organisms | Measures |
|---|---|---|---|
| Contact precautions | Direct/indirect contact | MRSA, VRE, C. difficile, ESBL organisms, scabies, RSV | Single room (or cohort); gloves + gown for room entry; dedicated equipment |
| Droplet precautions | Droplets >5 µm | Influenza, N. meningitidis, S. aureus, COVID-19 (non-aerosol) | Surgical mask for HCW; 1 m spatial separation |
| Airborne precautions | Droplet nuclei <5 µm | TB, measles, varicella, SARS-CoV-2 (AGP) | Negative-pressure room (AIIR); N95/FFP2 respirator; door closed; UV if available |
Hospital Infection Control Committee (HICC) — MI10.2:
Mandated by NABH (National Accreditation Board for Hospitals) for all Indian hospitals with >100 beds.
Composition: Medical superintendent (chair), Infection Control Officer (microbiologist), Infection Control Nurse (ICN), representatives from surgery, medicine, nursing, pharmacy, housekeeping, biomedical waste.
Functions:
- Develop and review infection control policies and SOPs
- Surveillance for HAI rates (CAUTI, CLABSI, VAP, SSI bundle rates)
- Outbreak investigation and response
- Antibiotic stewardship programme (ASP) oversight
- Healthcare worker education and training
- Monitor biomedical waste disposal compliance
- Decontamination and sterilisation oversight
- Post-exposure prophylaxis (needle-stick) management
Antibiotic Stewardship Programme (ASP):
- De-escalation: step down from broad-spectrum to targeted therapy once culture results available
- Prior authorisation for carbapenems, colistin, vancomycin
- Restricted formulary strategy
SELF-CHECK
A nurse is caring for a patient with confirmed pulmonary tuberculosis in a general medical ward. According to transmission-based precautions, which of the following is the MOST important additional measure above standard precautions?
A. Surgical face mask for the nurse and transferring the patient to a single room
B. N95/FFP2 respirator for the nurse and transfer to a negative-pressure isolation room
C. Double gloving and apron only
D. Droplet precautions with a 1-metre patient separation
Reveal Answer
Answer: B. N95/FFP2 respirator for the nurse and transfer to a negative-pressure isolation room
Pulmonary TB is transmitted by airborne droplet nuclei (<5 µm) that remain suspended in room air. Airborne precautions require: (1) N95/FFP2 respirator for healthcare workers (surgical masks do NOT filter particles <5 µm), (2) transfer to an Airborne Infection Isolation Room (AIIR) — a negative-pressure single room with ≥12 air changes per hour and exhausted air directed outside. Surgical masks and 1-metre separation are droplet precautions (inadequate for TB).
Antimicrobial Drug Resistance in HAI (MI10.5)
Antimicrobial Drug Resistance in Healthcare-Associated Infections
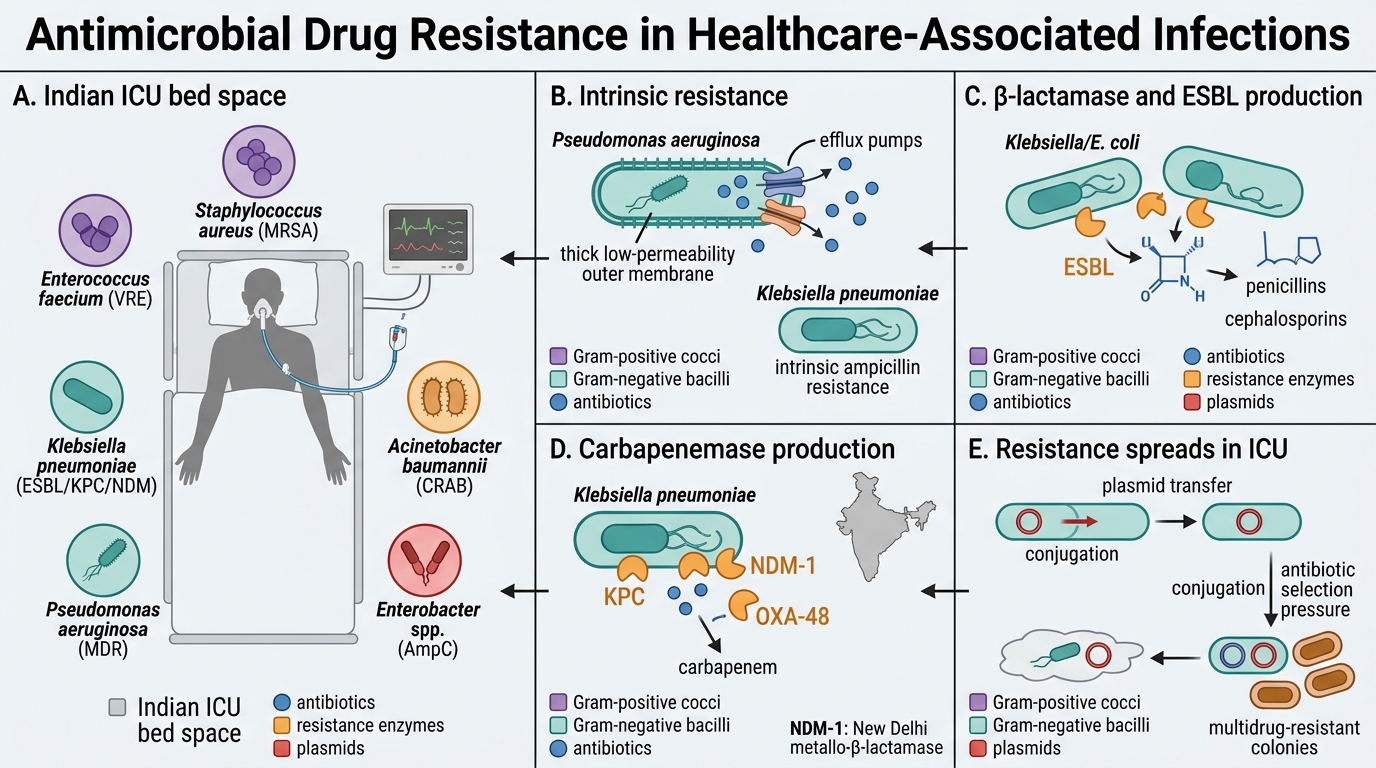
Priority resistant organisms in Indian ICUs (ESKAPE pathogens):
- E — Enterococcus faecium (VRE — Vancomycin-Resistant Enterococcus)
- S — Staphylococcus aureus (MRSA — Methicillin-Resistant S. aureus)
- K — Klebsiella pneumoniae (ESBL, KPC, NDM producers)
- A — Acinetobacter baumannii (CRAB — Carbapenem-Resistant)
- P — Pseudomonas aeruginosa (multidrug-resistant)
- E — Enterobacter spp. (AmpC derepression)
Mechanisms of resistance evolution:
1. Intrinsic resistance: Chromosomally encoded; organism always resistant (e.g., Pseudomonas impermeable to many antibiotics; Klebsiella intrinsic resistance to ampicillin)
2. Acquired resistance mechanisms:
| Mechanism | Example | Resistance to |
|---|---|---|
| β-lactamase production | ESBL (Klebsiella, E. coli) | Penicillins + cephalosporins |
| Carbapenemase production | KPC (K. pneumoniae), NDM-1 (New Delhi Metallo-β-lactamase), OXA-48 | Carbapenems (last resort) |
| Modified PBPs | MRSA (mecA gene → PBP2a) | All β-lactams |
| Efflux pumps | Pseudomonas MexAB-OprM | Multiple antibiotic classes |
| Outer membrane porin loss | Pseudomonas, Klebsiella | Carbapenems |
| Target site modification | VRE (VanA operon modifies D-Ala-D-Ala) | Vancomycin |
| Enzyme inactivation | Aminoglycoside-modifying enzymes | Aminoglycosides |
Spread of resistance in hospital:
- Clonal spread: Resistant organism spreads patient to patient via HCW hands (most common in short outbreaks)
- Horizontal gene transfer (HGT): Plasmids carrying resistance genes (R-plasmids) transferred between different bacterial species via conjugation — explains why NDM-1 spread across multiple genera rapidly
- Selection pressure: Broad-spectrum antibiotic use kills susceptible organisms, selecting resistant mutants

Mechanisms of Carbapenem Resistance in Gram-Negative Bacteria
Control of AMR in hospitals:
1. Antibiotic Stewardship — rational prescribing, de-escalation, formulary restriction
2. Contact Precautions — for all MDR organisms (gloves, gown, single room)
3. Active surveillance cultures — screen high-risk admissions (ICU, transfers) for MRSA/VRE/MDR-GNB rectal swabs
4. Environmental decontamination — terminal cleaning with hypochlorite; hydrogen peroxide vapour for outbreak rooms
5. Cohorting — group MDR-colonised patients, assign dedicated nursing staff
6. Reporting to ICMR AMR surveillance network — mandatory for reference lab isolates
NDM-1 (New Delhi Metallo-β-lactamase):
- Discovered in India (New Delhi, 2008); now global
- Plasmid-encoded carbapenemase conferring resistance to ALL β-lactams including carbapenems
- Last-resort options: colistin, tigecycline, fosfomycin, ceftazidime-avibactam
- Detected by: Modified Hodge Test (MHT), Carba NP test, PCR for bla-NDM gene
SELF-CHECK
NDM-1 (New Delhi Metallo-β-lactamase) resistance genes spread rapidly between different bacterial species in hospital settings primarily through:
A. Transduction (bacteriophage-mediated gene transfer)
B. Transformation (uptake of naked DNA from the environment)
C. Conjugation (plasmid transfer via sex pilus between bacteria)
D. Mutation in chromosomal beta-lactamase genes
Reveal Answer
Answer: C. Conjugation (plasmid transfer via sex pilus between bacteria)
NDM-1 and other carbapenemase genes are typically carried on mobile genetic elements (plasmids, transposons, integrons) that transfer between bacteria via conjugation — direct cell-to-cell contact through a sex pilus (F-like or IncF plasmid). This horizontal gene transfer (HGT) explains why NDM-1 was found simultaneously in Klebsiella, E. coli, Acinetobacter and other species. Transduction (phage-mediated) and transformation (naked DNA uptake) are less efficient over long resistance gene distances.
REFLECT
You are a junior resident on rounds in the medical ICU. You notice that the senior resident examined a patient on isolation precautions for MRSA without putting on gloves, then immediately moved to examine the next patient. The next patient is post-cardiac surgery and has a central line. What would you do? What is your obligation as a junior doctor? How would you communicate this to the senior resident without creating conflict?
KEY TAKEAWAYS
Healthcare-Associated Infections (HAIs) — CAUTI, CLABSI, VAP, SSI, CDI — are caused by device-related, procedural and environmental transmission of healthcare flora, predominantly Gram-negative MDR organisms and MRSA. The chain of transmission (agent → reservoir → exit → mode → entry → susceptible host) offers multiple intervention points. Standard precautions protect against all blood/body fluid exposures for all patients; transmission-based precautions (contact, droplet, airborne) layer additional protections for specific pathogens. The HICC (mandated by NABH) oversees HAI surveillance, outbreak response, antibiotic stewardship and HCW training. AMR in HAI is driven by β-lactamase/carbapenemase production (ESBL, KPC, NDM-1), efflux pumps, porin loss and HGT via plasmid conjugation — spread within hospitals by clonal transmission via hands and selection pressure from broad-spectrum antibiotic use. Control requires hand hygiene, contact precautions, antibiotic stewardship and active surveillance cultures.