Page 4 of 16
MI2.{4,6} | Immunity in Infection & Immunoprophylaxis — SDL Guide
Learning Objectives
- Explain the immune response to bacterial, mycobacterial, viral, fungal, and parasitic infections, highlighting how pathogen type determines the dominant immune arm.
- Discuss the immunological basis of active and passive immunoprophylaxis.
- Explain herd immunity and its threshold requirements in the Indian context.
INSTRUCTIONS
This module builds directly on the previous SDL (innate/adaptive immunity structure). Now we apply those mechanisms to specific pathogen classes and to immunisation. The clinical examples are drawn from Indian endemic infections and the Universal Immunisation Programme.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 11–12 (textbook)
- Park's Textbook of Preventive and Social Medicine, Ch on Immunology of Vaccines (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In 2014, India was declared polio-free — a disease that once paralysed tens of thousands of Indian children every year. The eradication did not require a cure or even 100% vaccination coverage. It required enough people to be immune that the virus could no longer find new hosts. Understanding how immunity stops infections at both the individual and population level is the scientific foundation of every public health immunisation campaign you will be part of as a doctor.
WHY THIS MATTERS
Two questions define this module's clinical relevance:
- Why does the same pathogen cause different disease in different people? The answer is pathogen-specific immune mechanisms and host immune competence.
- Why do vaccines work, and when do they fail? Herd immunity threshold, vaccine type (live vs killed), and immunological memory explain both.
For an MBBS graduate practising in India, knowledge of the Universal Immunisation Programme (UIP) and the immune basis of each vaccine is directly tested in theory exams and essential for community health postings.
RECALL
Quick recall before we proceed:
- Which T-helper subset (Th1 or Th2) is most important for killing intracellular bacteria? Why?
- What is the difference between IgM and IgG in terms of timing after infection?
- Name one vaccine from the UIP that uses a killed (inactivated) pathogen and one that uses a live attenuated pathogen.
Immune Response to Bacterial Infections
Immune Response to Bacterial Infections
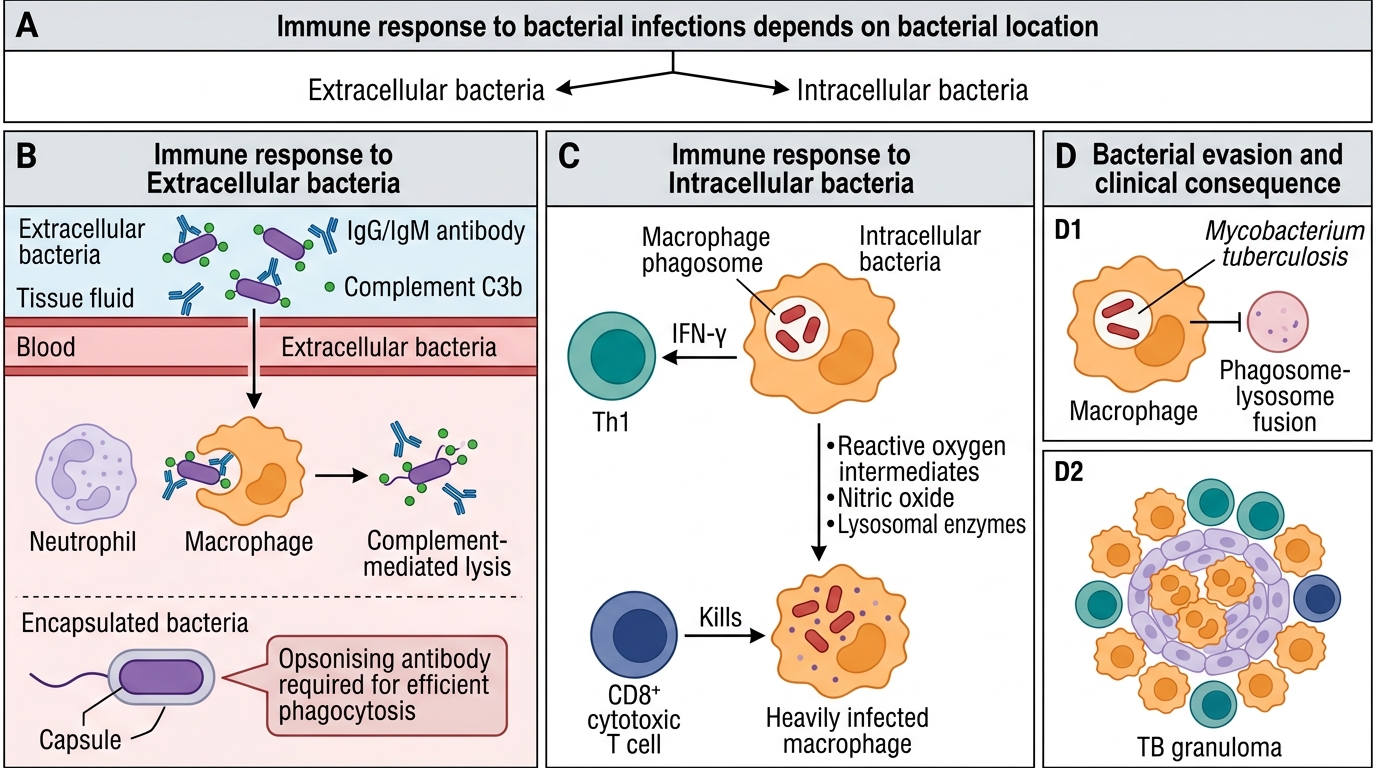
The immune response to bacteria depends critically on whether the bacterium is extracellular or intracellular.
Extracellular bacteria (e.g., Streptococcus pneumoniae, Staphylococcus aureus, Vibrio cholerae, Salmonella typhi in early infection):
- Innate: Complement activation (alternative and lectin pathways), neutrophil and macrophage phagocytosis
- Adaptive: Antibody (IgG, IgM) via humoral response is the primary effector
- Key protective mechanism: Opsonisation + complement-mediated lysis
- Encapsulated bacteria (Streptococcus pneumoniae, Haemophilus influenzae, Neisseria meningitidis) resist phagocytosis without opsonising antibody — this is why splenectomy (removes antibody-primed phagocytes) predisposes to overwhelming sepsis with these organisms
Intracellular bacteria (e.g., Mycobacterium tuberculosis, Listeria monocytogenes, Salmonella typhi — late/systemic phase, Brucella):
- Adaptive CMI is the essential defence
- Th1 cells secrete IFN-γ → activates macrophages → increased production of reactive oxygen intermediates (ROIs), nitric oxide, and lysosomal enzymes that kill intracellular bacteria
- Without Th1 activation, mycobacteria survive and replicate inside macrophage phagosomes
- CD8+ CTLs kill heavily infected macrophages, releasing bacteria for destruction
Mycobacterial infections (TB) — special mechanisms:
- M. tuberculosis evades innate immunity by inhibiting phagosome–lysosome fusion
- Granuloma formation: Characteristic immune response where macrophages, epithelioid cells, giant cells, and lymphocytes wall off the organism
- Granuloma = successful CMI containment; caseous necrosis within granuloma = partial immune failure
- BCG vaccine induces Th1 memory specifically against mycobacterial antigens
CLINICAL PEARL
The Mantoux (tuberculin) test as an immune read-out: The Mantoux test injects purified protein derivative (PPD) of M. tuberculosis intradermally. A positive reaction (≥10 mm induration at 48–72 h) is a Type IV (delayed-type) hypersensitivity reaction mediated by sensitised Th1 cells — not antibody. This distinguishes it from most diagnostic antibody tests. Induration (not erythema alone) is measured. A negative Mantoux in a child with suspected TB in the context of HIV or severe malnutrition (both suppress CMI) does NOT rule out TB.
Immune Response to Viral Infections
Immune Response to Viral Infections
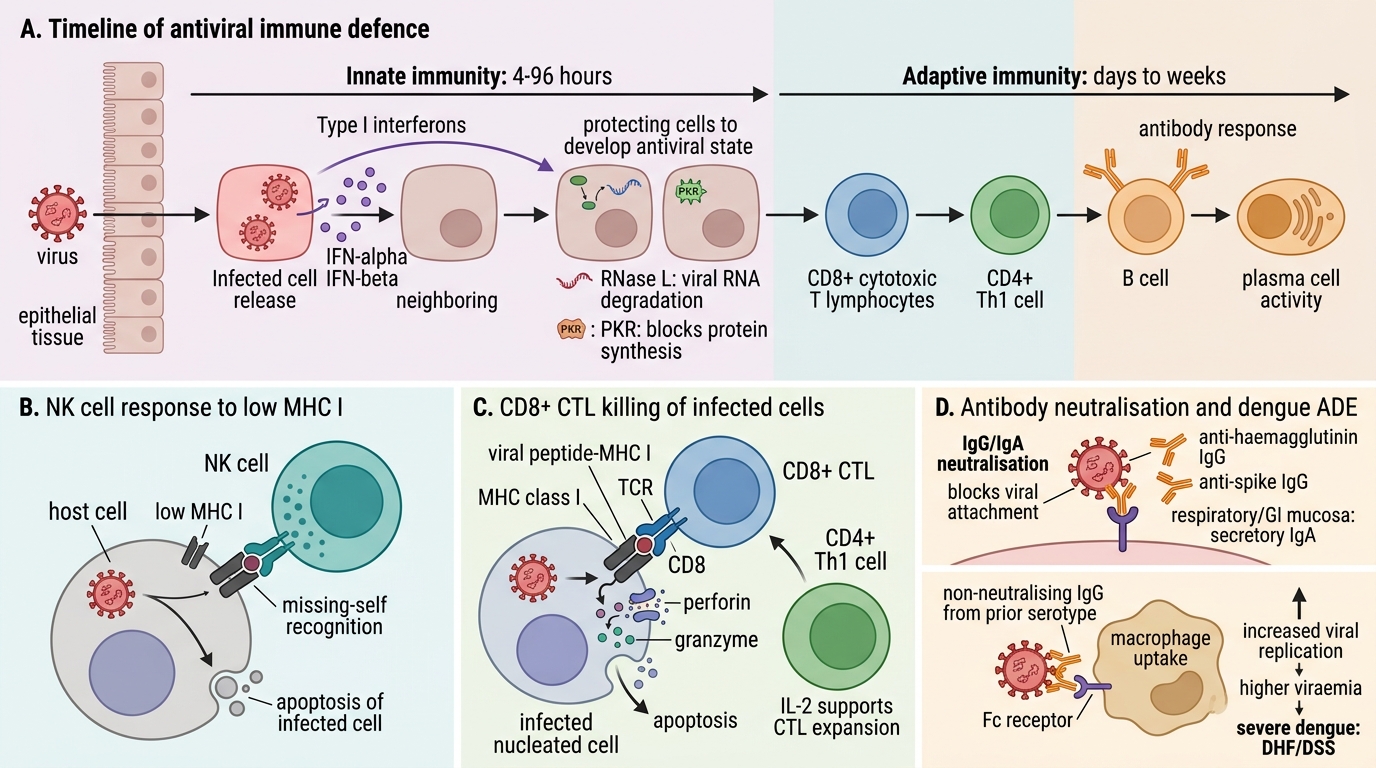
Viruses are obligate intracellular pathogens, so cell-mediated immunity is always central. The timeline of antiviral defence:
Innate (first 4–96 hours):
- Virus-infected cells produce Type I interferons (IFN-α, IFN-β) immediately after infection
- IFNs induce an antiviral state in neighbouring uninfected cells (upregulate RNase L, PKR → degrade viral RNA, block protein synthesis)
- Natural killer (NK) cells kill virally infected cells that downregulate MHC class I (a common viral immune-evasion strategy)
Adaptive (days to weeks):
- CD8+ CTLs: Primary effectors — recognise viral peptides on MHC class I and kill infected cells via perforin/granzyme
- CD4+ Th cells: Help activate CTLs and B cells; Th1 supports CTL expansion
- Antibody (IgG, IgA): Important for neutralisation — blocking viral attachment to host cell receptors (e.g., anti-haemagglutinin IgG prevents influenza infection; anti-SARS-CoV-2 spike IgG neutralises entry)
- Secretory IgA (sIgA) is critical at mucosal portals of entry (respiratory and GI tracts)
Dengue — antibody-dependent enhancement (ADE):
Pre-existing, non-neutralising IgG antibodies from a prior dengue infection with a different serotype can enhance uptake of the second-serotype virus into macrophages via Fc receptors → increased viral replication → higher viraemia → severe dengue (dengue haemorrhagic fever, dengue shock syndrome). This is why secondary dengue infection is typically more severe than primary, and why dengue vaccine design is complex.
Viral latency and reactivation (Herpes simplex, Varicella-zoster, EBV): Latent viruses hide in immune-privileged sites (neurons, B cells) and reactivate when CMI wanes (stress, immunosuppression). Reactivation risk explains why herpes zoster (shingles) is common in elderly and immunocompromised patients in Indian hospitals.
SELF-CHECK
A 35-year-old man from Chennai presents with a second episode of dengue, confirmed serologically with IgM for a different serotype from his first infection 2 years ago. He develops dengue haemorrhagic fever. Which immune mechanism best explains the severity of this second infection?
A. Complete absence of T-cell memory from first infection
B. Antibody-dependent enhancement: non-neutralising IgG from first infection facilitates macrophage uptake of the second serotype
C. Cross-reactive Th1 cells cause autoimmune destruction of endothelium
D. The second serotype produces a more potent NS1 protein that directly destroys platelets
Reveal Answer
Answer: B. Antibody-dependent enhancement: non-neutralising IgG from first infection facilitates macrophage uptake of the second serotype
Antibody-dependent enhancement (ADE) is the immunological mechanism underlying severe secondary dengue. Subneutralising IgG antibodies raised against the first dengue serotype cross-react with the second serotype but fail to neutralise it. Instead, these IgG antibodies bind to the virus and then to Fc receptors on monocytes/macrophages, facilitating viral entry and replication within those cells. This results in higher viral loads, greater cytokine release, and the vascular leak that characterises dengue haemorrhagic fever. ADE is why all four dengue serotypes must ideally be covered by a vaccine before first vaccination.
Immune Response to Fungal and Parasitic Infections
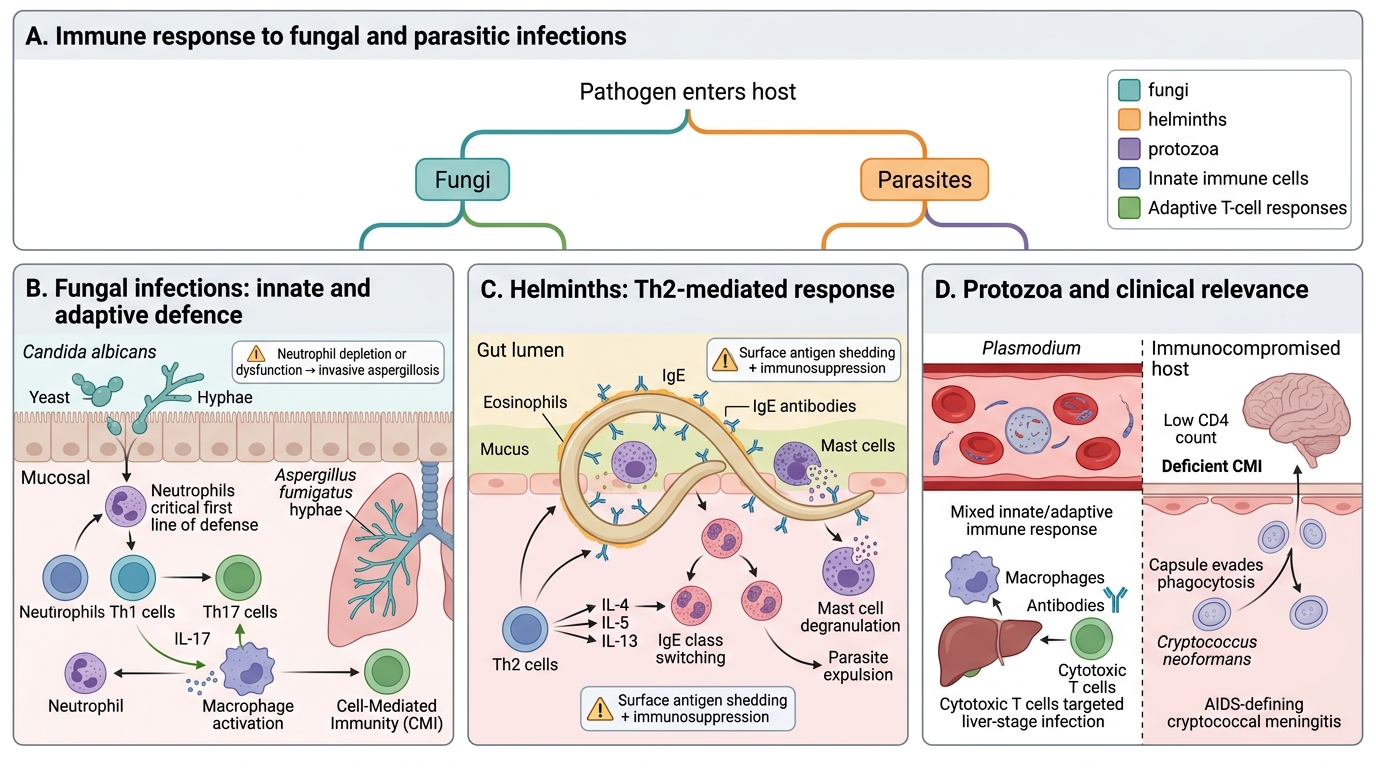
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Immune Response to Fungal and Parasitic Infections
Fungal infections (e.g., Candida albicans, Aspergillus fumigatus, Cryptococcus neoformans, Histoplasma capsulatum):
- Innate: Neutrophils are the critical first line — neutrophil dysfunction (as in agranulocytosis) or depletion predisposes to invasive aspergillosis
- Adaptive: CMI (Th1 and Th17) is the primary adaptive defence
- Th17 cells and IL-17 are particularly important at mucosal surfaces against Candida
- Th1 responses control dimorphic fungi (Histoplasma, Coccidioides)
- Important in India: Cryptococcus neoformans meningitis is an AIDS-defining opportunistic infection. Deficient CMI (low CD4 count) allows capsulated cryptococci to evade phagocytosis and establish CNS infection.
Parasitic infections (helminths and protozoa) — the immune response varies dramatically:
| Parasite type | Dominant immune response | Evasion mechanism |
|---|---|---|
| Helminths (Ascaris, Wuchereria) | Th2 → IgE, eosinophilia, mast cells | Shedding surface antigens, immunosuppression |
| Protozoa (Plasmodium) | Mixed; antibody (anti-merozoite) + CMI | Antigenic variation, RBC sequestration |
| Leishmania | Th1 (IFN-γ) controls infection | Survives in macrophages, inhibits IL-12 |
| Toxoplasma | Th1, CTL; NK in early phase | Inhibits phagosome acidification |
ADCC (antibody-dependent cell-mediated cytotoxicity): IgE coats helminth larvae; eosinophils and mast cells recognise IgE via FcεR and degranulate, releasing toxic eosinophilic granule proteins (major basic protein) that damage helminth cuticle. This explains why elevated IgE and eosinophilia are hallmarks of active helminth infection in Indian patients.