Page 5 of 16
MI2.{4,6} | Immunity in Infection & Immunoprophylaxis — SDL Guide (Part 2)
Immunoprophylaxis: Active Immunity
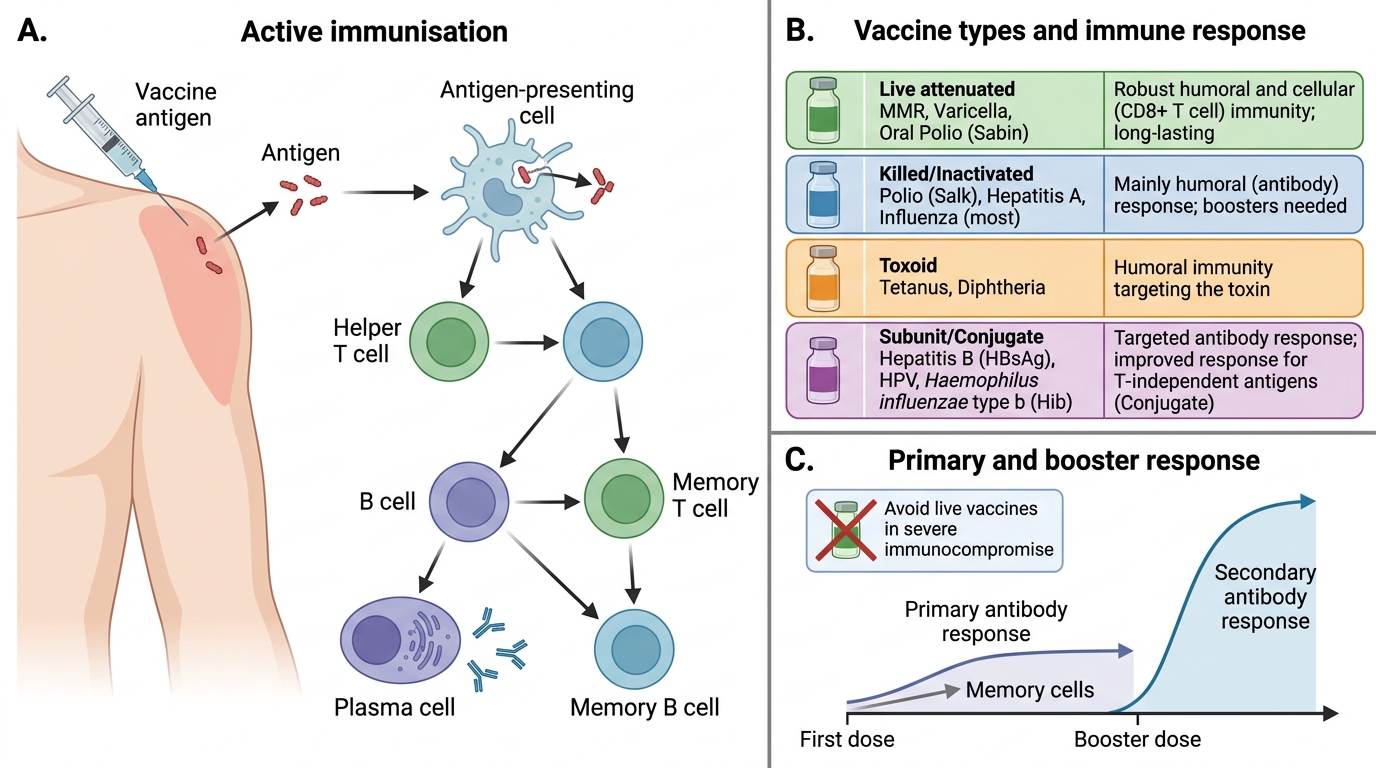
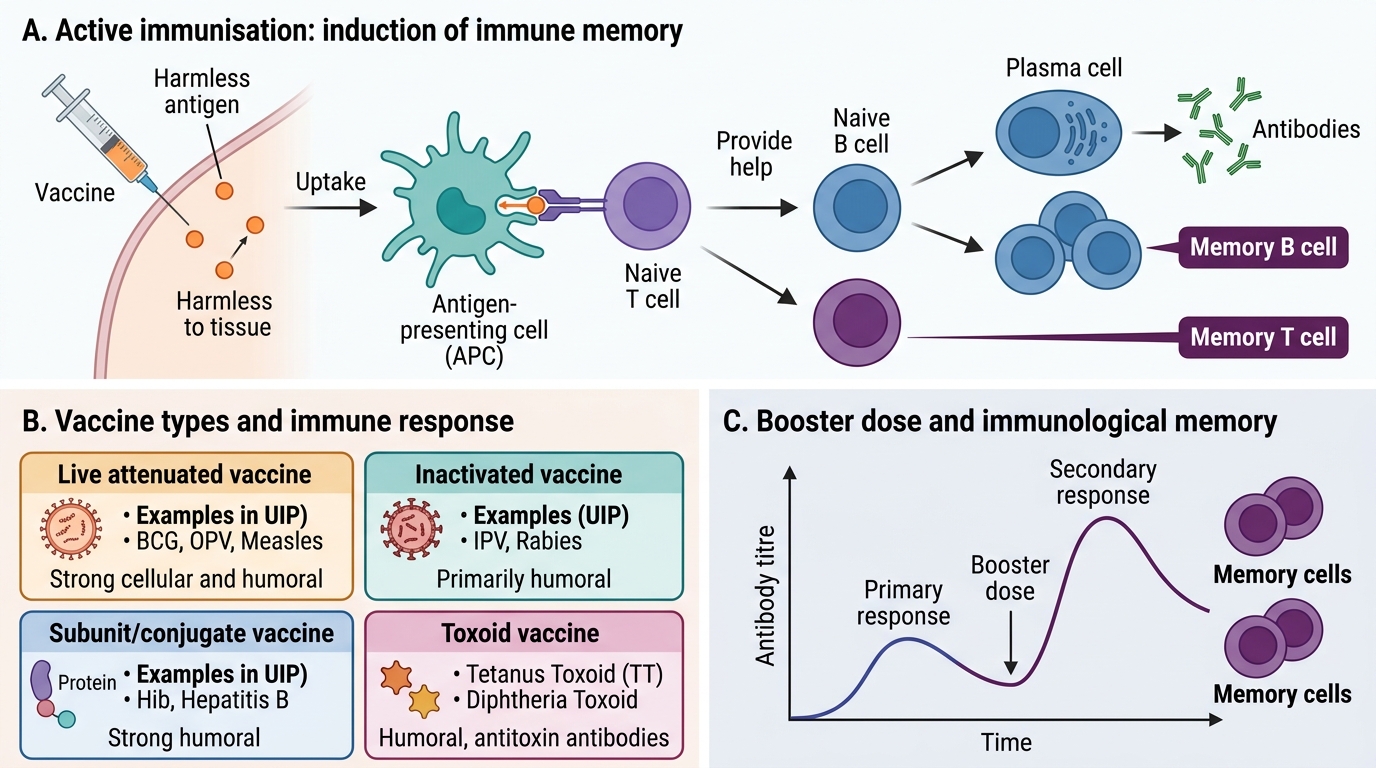
Active Immunisation: Mechanism and Vaccine Types
Active immunisation uses vaccines to induce antigen-specific immunological memory, mimicking the effects of natural infection without causing disease.
Types of vaccines and their immunological basis:
| Vaccine type | Examples (Indian UIP / National Programme) | Immune response |
|---|---|---|
| Live attenuated | OPV, MMR, BCG, varicella, rotavirus, yellow fever | Strong, long-lasting CMI + antibody; mimics natural infection; risk of reversion in immunocompromised |
| Killed/inactivated | IPV, whole-cell pertussis (DPT), hepatitis A, influenza (some) | Mainly antibody; often requires boosters; safe in immunocompromised |
| Toxoid | Diphtheria toxoid (DT), tetanus toxoid (TT) | Antibody against toxin; requires boosters |
| Subunit/conjugate | HepB surface antigen, PCV13, Hib, meningococcal conjugate, HPV (VLPs) | Antibody; conjugation converts TI to TD antigen (enables infant immunisation) |
| mRNA vaccines | COVID-19 (Covishoot technology) | Antibody + CMI; novel; no live pathogen |
Primary vs booster doses: The primary schedule generates memory cells. Booster doses restimulate memory B and T cells → anamnestic response with rapid, high-titre IgG production. Example: TT schedule — primary series (3 doses in infancy) + boosters at 18 months, 5 years, and pregnancy.
Cold chain: Live attenuated vaccines are thermolabile and MUST be maintained at 2–8°C (or frozen for OPV). Failure of cold chain is the most common operational reason for vaccine failure in India's rural immunisation posts.

Primary and Secondary Antibody Responses
Immunoprophylaxis: Passive Immunity & Herd Immunity
Active Immunisation and Immunological Memory
Passive immunisation provides pre-formed antibodies for immediate but short-lived protection. No memory is generated.
Types of passive immunisation:
| Type | Source | Duration | Indian examples |
|---|---|---|---|
| Natural passive | Maternal IgG crosses placenta; sIgA in breast milk | 3–6 months after birth | Protects neonates from measles, tetanus |
| Artificial passive (homologous) | Human immunoglobulin preparations | 2–3 weeks | HRIG (rabies PEP), VZIG (varicella PEP), tetanus immunoglobulin (TIG) |
| Artificial passive (heterologous) | Equine (horse) antisera | 1–2 weeks; serum sickness risk | Anti-snakevenom serum, older ADS, ATS |
Serum sickness: A systemic Type III hypersensitivity reaction to foreign (animal-derived) immunoglobulin. Occurs 7–14 days after administration. Features: fever, urticaria, arthralgia, lymphadenopathy. Mechanism: antigen–antibody complexes deposited in vessels/joints → complement activation → inflammation.
Herd (population/community) immunity: When a sufficient proportion of a population is immune to an infectious disease, transmission chains are broken even for non-immune individuals — the "herd" protects its vulnerable members.
Herd immunity threshold (HIT):
$$HIT = 1 - \frac{1}{R_0}$$
where R₀ = basic reproduction number (average secondary cases per primary case in a fully susceptible population).
| Disease | R₀ | HIT |
|---|---|---|
| Measles | 12–18 | 92–95% |
| Polio | 5–7 | 80–85% |
| COVID-19 (original) | 2–3 | 50–67% |
| Influenza | 2–3 | 50–67% |
Measles in India: High R₀ means India needs >92% vaccination coverage to prevent outbreaks. Despite strong UIP, pockets of unvaccinated children in urban slums and remote tribal areas have sustained measles outbreaks in recent years, highlighting the gap between national coverage rates and local herd immunity thresholds.

Herd Immunity and Transmission Chains
SELF-CHECK
A 6-month-old infant develops severe measles. The child received the first dose of measles vaccine at 9 months as per UIP schedule. The mother received one dose of measles vaccine at age 9 months 28 years ago but has no documented immunity. Why was this infant NOT protected by maternal immunity?
A. Maternal IgM (not IgG) is transferred to the foetus, which has a short half-life
B. Maternal IgG from a single childhood measles dose wanes over decades and was insufficient to transfer protective levels to the foetus
C. The infant's Fc receptor cannot bind maternal IgG before 6 months of age
D. Live measles vaccine produces CMI only, not IgG, so no maternal antibody is transferred
Reveal Answer
Answer: B. Maternal IgG from a single childhood measles dose wanes over decades and was insufficient to transfer protective levels to the foetus
Maternal IgG is actively transferred across the placenta via FcRn receptors during the third trimester. However, maternal IgG wanes over time. A mother vaccinated once 28 years ago with a single childhood dose likely has low measles IgG titres by adulthood — insufficient to confer protective levels to the foetus. Additionally, even when maternal IgG is transferred, it typically wanes in the infant by 4–6 months. This is why the first measles dose is given at 9 months in India (when maternal antibody has fallen enough to avoid vaccine interference), and why the schedule optimises protection at the age of highest risk.