Page 7 of 16
MI2.{5,7-8} | Immunodiagnostics & Immunological Disorders — SDL Guide
Learning Objectives
- Describe the principles and clinical applications of laboratory tests used in diagnostic microbiology that are based on the host's immune response.
- Describe the immunological mechanisms underlying hypersensitivity reactions, autoimmune disorders, and immunodeficiency states, and discuss laboratory methods for their detection.
- Describe the immunological mechanisms in transplantation and tumour immunity and their applications in disease management.
INSTRUCTIONS
This module completes the Immunology cluster by applying immune principles to diagnosis and to disorders where the immune system itself causes disease. It contains the highest density of clinically testable material in Year-2 Microbiology theory examinations.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 11–13 (textbook)
- Robbins & Cotran Pathologic Basis of Disease, Ch 6 (Diseases of Immunity) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 26-year-old nurse from Hyderabad develops a swollen, itchy hand after changing her latex gloves at work. Within minutes she develops urticaria, wheezing, and her blood pressure drops to 80/50 mmHg. Simultaneously, a 16-year-old girl in the same hospital is found to have positive ANA and anti-dsDNA antibodies after presenting with joint pain, butterfly rash, and protein in her urine. In the transplant unit, a kidney recipient has her graft function declining on Day 7. Three patients, three different immunological crises — all caused not by pathogens, but by the immune system itself.
WHY THIS MATTERS
Immunological disorders are among the most complex and frequently encountered problems in clinical medicine:
- Hypersensitivity reactions explain common presentations: anaphylaxis, asthma, contact dermatitis, drug reactions, serum sickness
- Autoimmune diseases (SLE, rheumatoid arthritis, type 1 diabetes) affect millions in India
- Immunodeficiency underlies the HIV epidemic and congenital conditions presenting in paediatrics
- Transplantation immunology is increasingly relevant as organ transplantation expands in India
- Tumour immunology underlies cancer immunotherapy, one of the fastest-growing fields in oncology
Immunological laboratory tests are the workhorses of diagnostic microbiology — from simple agglutination tests in PHCs to ELISA in district hospitals to flow cytometry in tertiary centres.
RECALL
Brief recall check:
- What is the difference between IgE and IgG in terms of serum concentration and function?
- In the context of infection, what does "antigen–antibody complex" mean, and what complement components get activated?
- What does CD4 count represent clinically in HIV-positive patients?
Immunological Laboratory Tests: Principles and Applications
Principles of Immunological Laboratory Tests
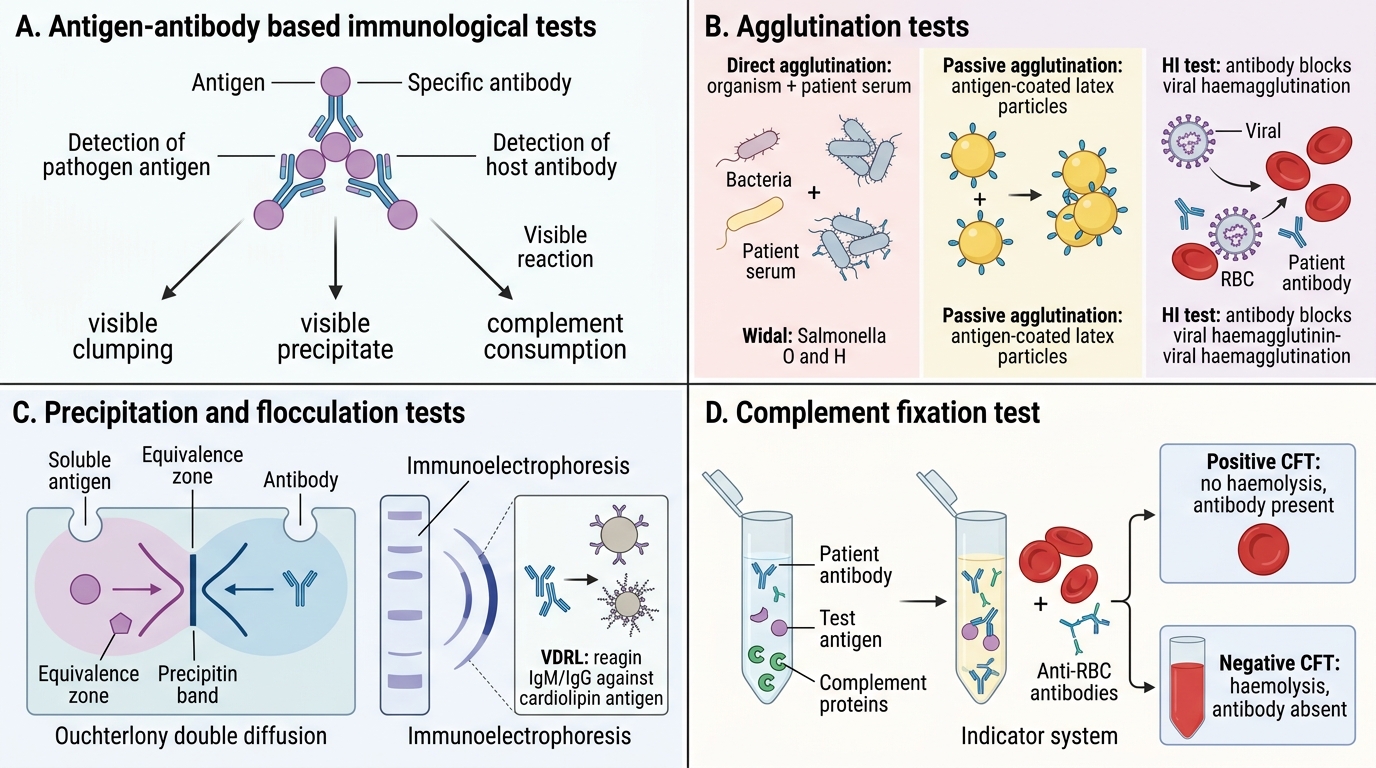
Immunological laboratory tests exploit antigen–antibody interactions for detection of either pathogens or host antibodies.
1. Agglutination tests
- Principle: Particulate antigens (bacteria, RBCs, latex particles) clump visibly when mixed with specific antibody
- Direct agglutination: Organism + patient serum (e.g., Widal test for typhoid: Salmonella O and H agglutination; Brucella agglutination test)
- Indirect (passive) agglutination: Soluble antigen adsorbed onto inert particles (latex, RBCs) + patient serum
- Haemagglutination inhibition (HI): Viral haemagglutinins agglutinate RBCs; patient antibody blocks this — HI titre measures antibody level (e.g., influenza serology)
2. Precipitation tests
- Principle: Soluble antigen + antibody form visible precipitate at equivalence zone
- Ouchterlony double diffusion: Antigen and antibody diffuse toward each other in gel; precipitin band forms (used for aspergillus precipitins)
- Immunoelectrophoresis: Combines gel electrophoresis + precipitin reaction (serum protein analysis)
- VDRL (Venereal Disease Research Laboratory): Non-treponemal flocculation test for syphilis screening — uses reagin (IgM + IgG against cardiolipin–lecithin–cholesterol antigen)
3. Complement fixation test (CFT)
- Principle: If patient antibody binds to test antigen, complement is "fixed" (consumed); residual complement haemolyses indicator RBCs. No haemolysis = positive (antibody present).
- Used for: syphilis (historical), Brucella, mycoplasma serology
4. ELISA (Enzyme-Linked Immunosorbent Assay)
- Most widely used diagnostic immunological test
- Antigen is coated on microtitre plate → patient serum added → enzyme-linked anti-human IgG added → substrate added → colour change indicates antibody presence
- Variants: direct ELISA, indirect ELISA, sandwich ELISA (detects antigen), competitive ELISA
- Indian applications: HIV ELISA (mandatory 3-test algorithm), hepatitis B surface antigen (HBsAg), anti-HCV, dengue NS1 antigen, anti-dengue IgM/IgG
5. Western blot (immunoblot)
- Confirmatory test after ELISA screening (e.g., HIV confirmatory)
- Antigens separated by molecular weight via SDS-PAGE, transferred to nitrocellulose membrane, probed with patient serum + enzyme-labelled anti-human IgG
- Interpretation: specific band patterns confirm diagnosis
6. Immunofluorescence
- Direct IF: Fluorescent antibody applied to specimen — detects antigen (e.g., rabies DFA on brain tissue, Chlamydia DFA)
- Indirect IF (IIF): Patient serum + substrate cells/tissue → fluorescent anti-human IgG. Used for autoantibody detection (ANA-IIF, ANCA-IIF)
7. Flow cytometry
- Principle: Cells in suspension pass through laser; fluorescence-labelled antibodies (monoclonal antibodies against CD markers) identify cell populations
- Indian applications: CD4 count in HIV monitoring (threshold: 200 cells/μL for OI prophylaxis, 350 cells/μL for ART initiation);
lymphocyte subset analysis in immunodeficiency
8. Rapid immunochromatographic tests (lateral flow assays)
- Coloured particle (colloidal gold) conjugated antibody + test strip with capture antibody lines
- Examples: HIV rapid test, malaria RDT (anti-HRP2), dengue combo NS1/IgM/IgG, COVID-19 antigen test
- Point-of-care tests at PHC/CHC level in India's NACO and NVBDCP programmes
CLINICAL PEARL
False-positive VDRL (biological false positive): The VDRL test detects anti-cardiolipin antibody (reagin), not anti-Treponema antibody specifically. Anti-cardiolipin antibodies are also produced in conditions causing tissue damage: SLE, antiphospholipid syndrome, tuberculosis, malaria, pregnancy, viral infections. A patient with SLE and a positive VDRL does NOT necessarily have syphilis — always confirm a reactive VDRL with a treponemal-specific test (TPHA or FTA-ABS).
Hypersensitivity Reactions: The Gell & Coombs Classification
Gell & Coombs Classification of Hypersensitivity Reactions
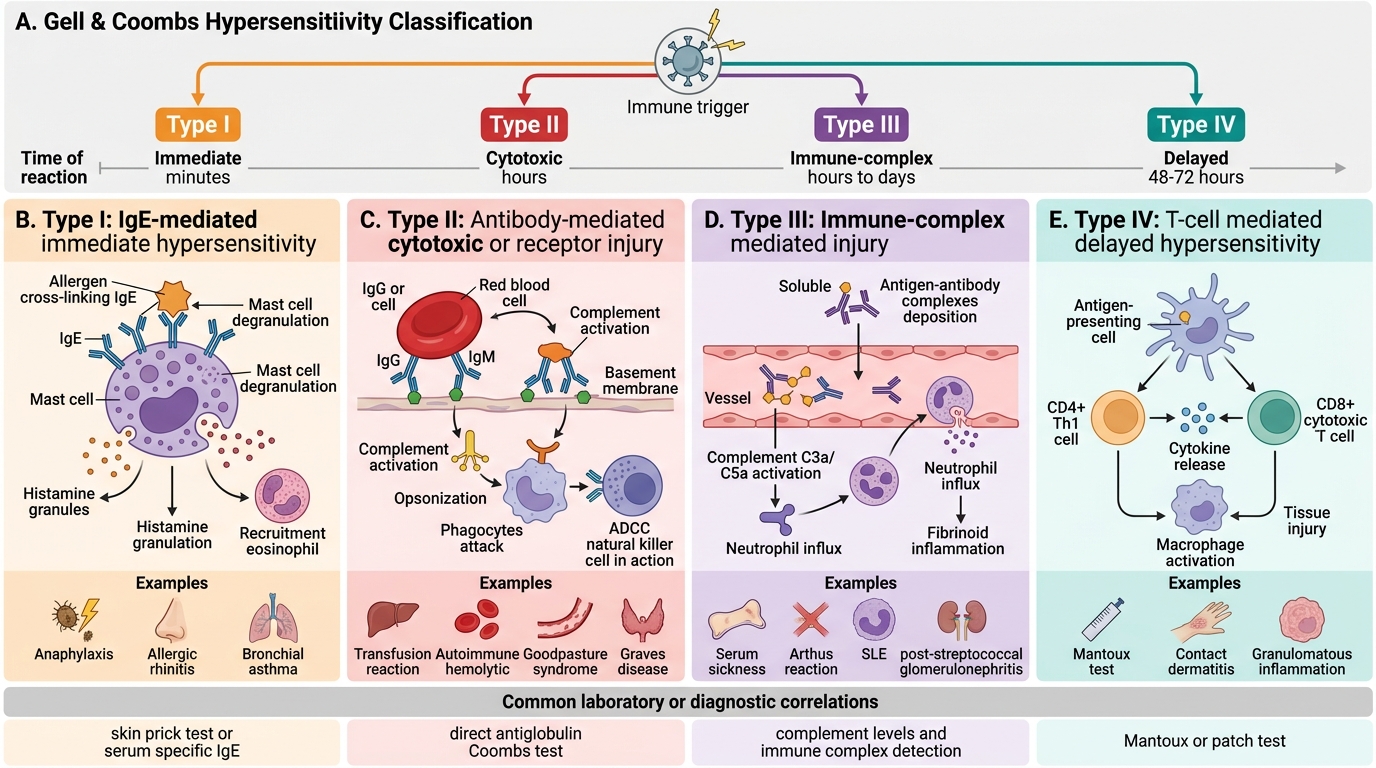
Hypersensitivity is an exaggerated or inappropriate immune response to antigens (allergens, self-antigens, drugs), causing tissue damage.
Gell & Coombs classification (4 types):
Type I — Immediate (IgE-mediated, Anaphylactic)
- Mechanism: First exposure → antigen sensitises mast cells/basophils via IgE bound to FcεR1 → re-exposure → antigen cross-links IgE → mast cell degranulation → histamine, leukotrienes, prostaglandins
- Onset: Seconds to minutes
- Indian examples: Anaphylaxis (penicillin, latex, bee sting), atopic asthma, allergic rhinitis, food allergy
- Lab: Elevated total serum IgE, specific IgE (RAST/ImmunoCAP), skin prick test
Type II — Cytotoxic (Antibody-mediated, IgG/IgM)
- Mechanism: Antibody (IgG or IgM) directed against cell surface or extracellular matrix antigens → complement activation + ADCC → cell destruction
- Onset: Hours
- Indian examples: Haemolytic transfusion reactions (ABO incompatibility), autoimmune haemolytic anaemia, Goodpasture's syndrome (anti-GBM antibody → glomerulonephritis + pulmonary haemorrhage), myasthenia gravis (anti-AChR antibody blocks neuromuscular junction)
Type III — Immune Complex (IgG-antigen complexes)
- Mechanism: Soluble antigen–antibody complexes deposited in vessel walls/joints → complement activation → C3a, C5a → neutrophil recruitment → lysosomal enzyme release → tissue damage
- Onset: Hours to days
- Indian examples: Post-streptococcal glomerulonephritis, serum sickness (equine anti-snake venom), SLE (anti-dsDNA complexes in glomeruli), reactive arthritis, Arthus reaction
- Lab: Low complement (C3, C4), circulating immune complexes, granular immunofluorescence on renal biopsy
Type IV — Delayed-type (Cell-mediated, DTH)
- Mechanism: Sensitised CD4+ Th1 cells re-exposed to antigen → IFN-γ secretion → macrophage activation → tissue damage (no antibody involved)
- Onset: 24–72 hours (delayed)
- Indian examples: Mantoux/tuberculin test, contact dermatitis (nickel jewellery — very common in India), granulomatous diseases (sarcoidosis, leprosy), graft rejection (cell-mediated)
- Lab: Patch test (contact dermatitis), Mantoux test

Summary of the Four Hypersensitivity Types
SELF-CHECK
A 30-year-old woman develops fever, urticaria, arthralgia, and lymphadenopathy 10 days after receiving equine anti-snakevenom serum. Her complement levels (C3, C4) are low. Urinalysis shows proteinuria. Which type of hypersensitivity reaction is this?
A. Type I (IgE-mediated anaphylaxis)
B. Type II (cytotoxic antibody-mediated)
C. Type III (immune complex-mediated)
D. Type IV (delayed-type, cell-mediated)
Reveal Answer
Answer: C. Type III (immune complex-mediated)
This is classic serum sickness — a Type III (immune complex) hypersensitivity reaction. The timeline (7–14 days after antigen administration), systemic features (fever, urticaria, arthralgia, lymphadenopathy), low complement levels, and renal involvement (proteinuria from glomerular immune complex deposition) are all hallmarks of Type III hypersensitivity. Equine antisera contain foreign (heterologous) proteins that act as antigens; when the immune response peaks at 7–14 days, antigen–antibody complexes form in slight antigen excess (equivalence zone), deposit in vessel walls and glomeruli, activate complement, and recruit neutrophils causing widespread inflammation. Low C3 and C4 confirm complement consumption by deposited complexes.
Autoimmune Disorders: Mechanisms and Laboratory Detection
Autoimmune Disorders: Mechanisms and Detection
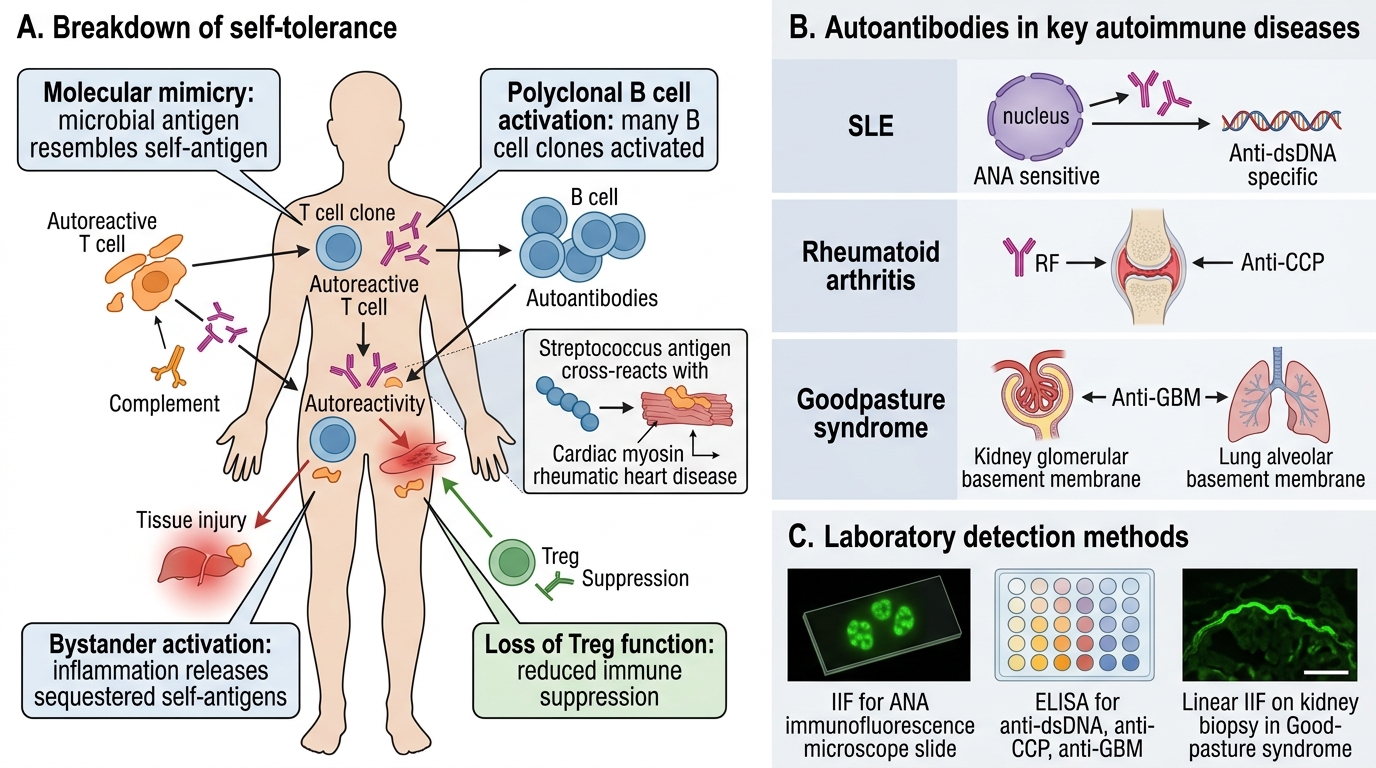
Autoimmune diseases result from failure of self-tolerance — the immune system attacks the body's own tissues.
Mechanisms of tolerance breakdown:
- Molecular mimicry: Microbial antigen resembles self-antigen; anti-microbial immune response cross-reacts with self (e.g., anti-streptolysin O cross-reacts with cardiac myosin → rheumatic heart disease)
- Polyclonal B cell activation: Some pathogens non-specifically activate many B cell clones, including autoreactive ones (e.g., EBV, malaria)
- Bystander activation: Local inflammation releases self-antigens that were previously sequestered
- Loss of T regulatory (Treg) cell function
Key autoimmune diseases and their autoantibodies (testable in theory exams):
| Disease | Key autoantibody | Detection method |
|---|---|---|
| SLE | Anti-dsDNA (specific), ANA (sensitive) | IIF (ANA), ELISA (anti-dsDNA) |
| Rheumatoid arthritis | Rheumatoid factor (RF), anti-CCP | ELISA, agglutination |
| Goodpasture syndrome | Anti-GBM | ELISA, linear IIF on kidney biopsy |
| Myasthenia gravis | Anti-AChR | ELISA, RIA |
| Graves' disease | Anti-TSH receptor (thyroid-stimulating Ig) | ELISA |
| Hashimoto's thyroiditis | Anti-thyroid peroxidase (anti-TPO), anti-thyroglobulin | ELISA |
| Antiphospholipid syndrome | Anticardiolipin Ab, lupus anticoagulant | ELISA, clotting tests |
| Celiac disease | Anti-tissue transglutaminase (anti-tTG) IgA | ELISA |
ANA patterns and clinical significance (by indirect immunofluorescence on HEp-2 cells):
- Homogeneous: Anti-dsDNA → SLE
- Speckled: Anti-Sm, anti-RNP → SLE, mixed connective tissue disease
- Nucleolar: Anti-topoisomerase I (Scl-70) → diffuse systemic sclerosis
- Centromere: Anti-centromere → CREST syndrome (limited systemic sclerosis)