Page 8 of 16
MI2.{5,7-8} | Immunodiagnostics & Immunological Disorders — SDL Guide (Part 2)
Immunodeficiency States
Primary Immunodeficiency States
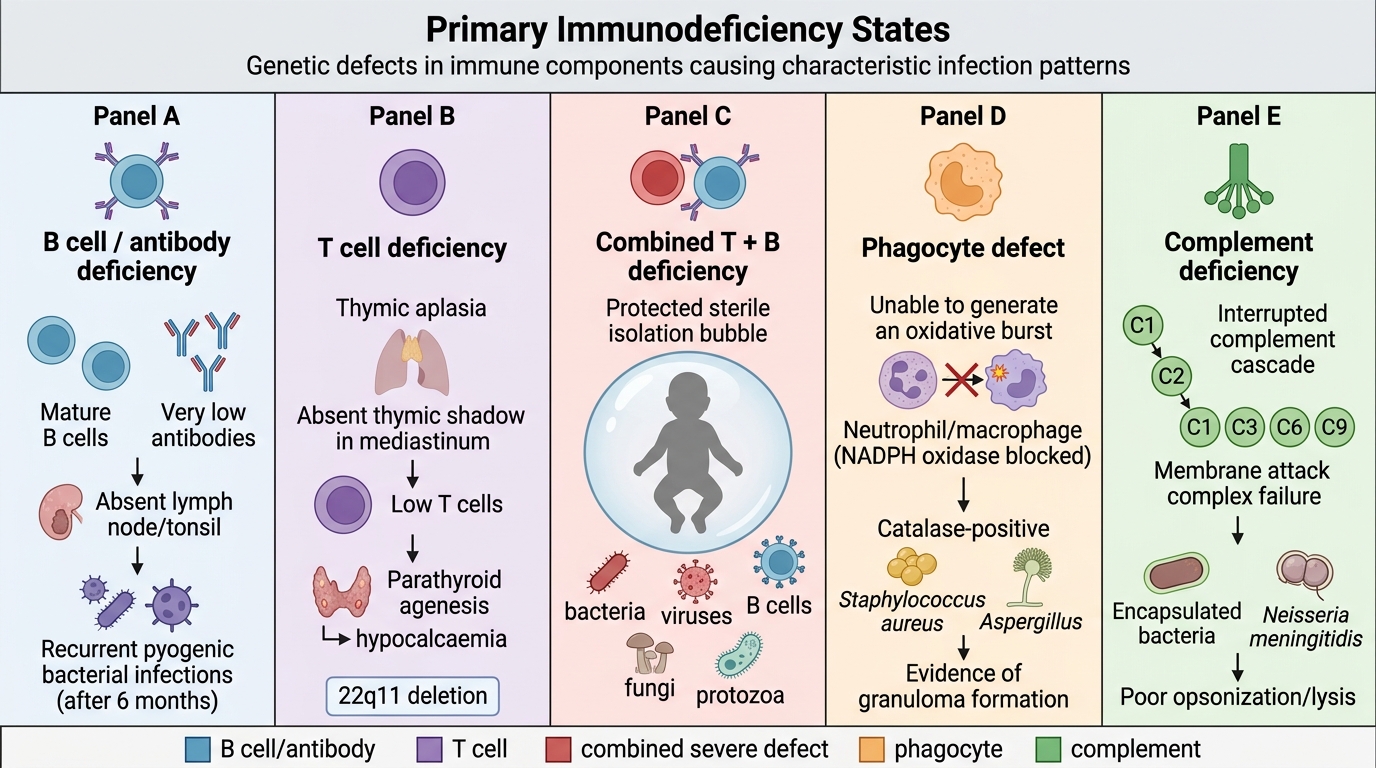
Primary (congenital) immunodeficiency results from genetic defects in immune components.
| Deficiency type | Syndrome | Clinical features |
|---|---|---|
| B cell/antibody | X-linked agammaglobulinaemia (XLA) | Recurrent pyogenic infections after 6 months; absent B cells and Ig; absent lymphoid tissue |
| T cell | DiGeorge syndrome (thymic aplasia) | Recurrent viral, fungal infections; absent thymic shadow; hypocalcaemia (parathyroid agenesis); associated with 22q11 deletion |
| Combined T + B | SCID (Severe Combined Immunodeficiency) | Life-threatening infections with all pathogens from birth; absent T and B cells; "bubble boy" |
| Phagocyte | Chronic granulomatous disease (CGD) | Recurrent infections with catalase-positive bacteria (Staph, Aspergillus); defective NADPH oxidase (oxidative burst absent) |
| Complement | C3 deficiency, MAC deficiencies | (see previous module) |
Secondary (acquired) immunodeficiency — most common causes in India:
- HIV/AIDS: Progressive CD4+ T cell depletion → combined immunodeficiency
- Malnutrition: Most common cause of immune suppression worldwide — protein-energy malnutrition impairs CMI, reduces complement and phagocyte function; highly relevant in rural India
- Diabetes mellitus: Impaired neutrophil function → recurrent skin/UTI/fungal infections
- Immunosuppressive therapy: Corticosteroids, methotrexate, cyclosporin (post-transplant, autoimmune disease)
- Malignancy: Haematological malignancies (CLL, myeloma) cause hypogammaglobulinaemia; solid tumours impair CMI
Laboratory evaluation of immunodeficiency:
- CBC with differential: Lymphocyte count; neutrophil count
- Immunoglobulin quantification (IgG, IgA, IgM) by radial immunodiffusion or ELISA — reduced in humoral immunodeficiencies
- Flow cytometry: CD4/CD8 ratio and absolute counts (HIV monitoring)
- Nitroblue tetrazolium (NBT) test / dihydrorhodamine (DHR) flow assay: Tests oxidative burst — absent in CGD
- Lymphocyte transformation test: Assesses T-cell proliferative response to mitogens
SELF-CHECK
A 4-year-old boy is brought with recurrent liver abscesses and lymphadenitis due to Staphylococcus aureus and Aspergillus fumigatus. His absolute lymphocyte count and immunoglobulin levels are normal. The nitroblue tetrazolium (NBT) test shows no colour change. What is the most likely diagnosis?
A. X-linked agammaglobulinaemia (XLA)
B. Chronic granulomatous disease (CGD)
C. DiGeorge syndrome
D. Severe combined immunodeficiency (SCID)
Reveal Answer
Answer: B. Chronic granulomatous disease (CGD)
Chronic granulomatous disease (CGD) is caused by a defect in NADPH oxidase, the enzyme phagocytes use to generate the reactive oxygen species (superoxide) required to kill catalase-positive organisms. Catalase-positive bacteria and fungi (Staphylococcus aureus, Aspergillus, Serratia, Burkholderia) are not killed after ingestion, leading to recurrent deep-seated infections (liver abscesses, lymphadenitis, osteomyelitis). The NBT test (reduced to blue formazan by normal oxidative burst) shows no colour change because the oxidative burst is absent. Lymphocytes and immunoglobulins are normal because B and T cell arms are unaffected.
Transplantation Immunology
Transplant Rejection and Allorecognition
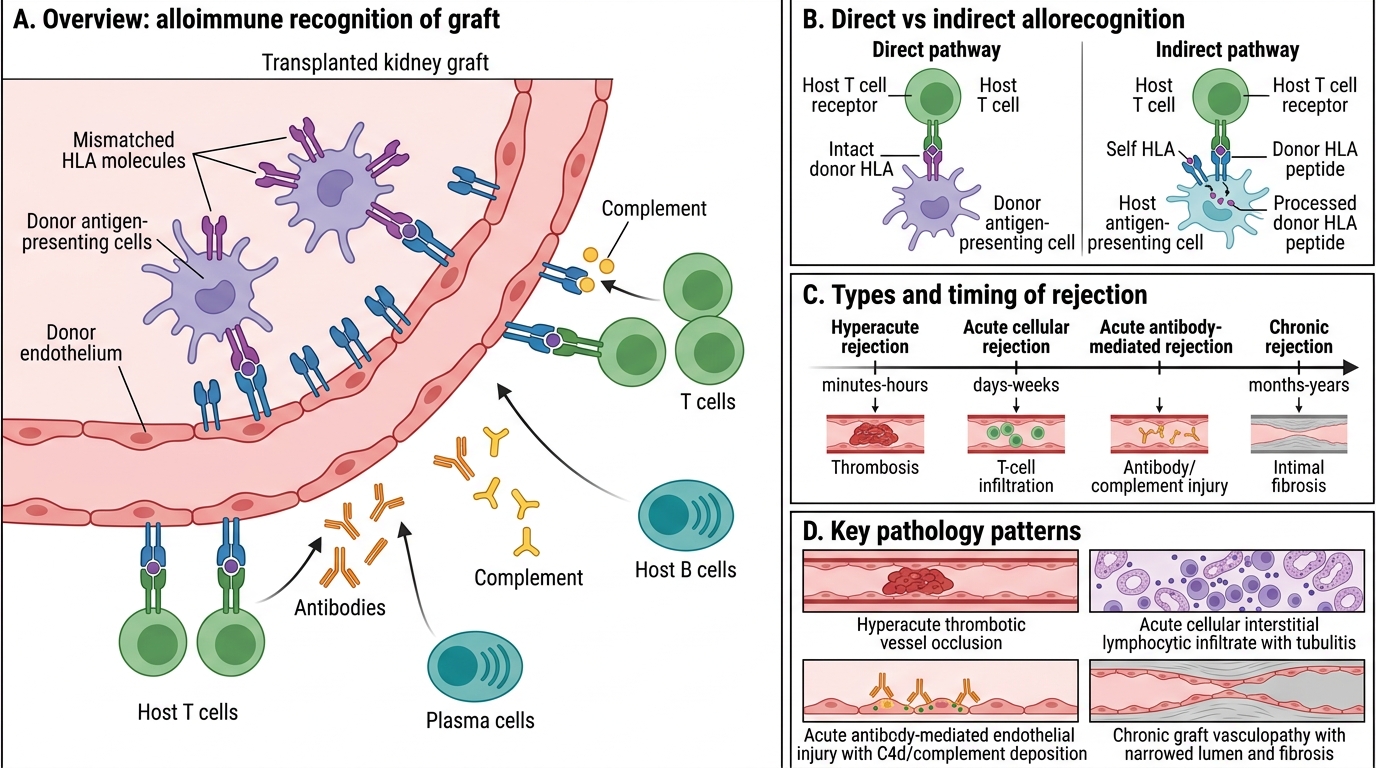
Transplant rejection is the major immunological barrier to successful organ grafting, driven by immune recognition of major histocompatibility complex (MHC/HLA) differences between donor and recipient.
Allorecognition pathways:
- Direct pathway: Host T cells directly recognise intact donor MHC molecules on donor antigen-presenting cells — responsible for acute rejection
- Indirect pathway: Host T cells recognise processed donor peptides presented on host MHC — responsible for chronic rejection
Types of rejection:
| Type | Timing | Mechanism | Pathology |
|---|---|---|---|
| Hyperacute | Minutes to hours | Pre-formed donor-specific antibodies (ABO mismatch, prior sensitisation) → complement + thrombosis | Thrombotic vessel occlusion; graft immediately non-functional |
| Acute cellular | Days to weeks | CD8+ CTLs and Th1 cells attack graft | Lymphocyte infiltration, tubulitis (renal), endothelialitis |
| Acute humoral | Days to weeks | Donor-specific antibodies (DSA) → complement + Fc-mediated endothelial injury | C4d deposition, glomerulitis |
| Chronic | Months to years | Low-grade antibody + T cell responses → fibrosis | Graft vessel intimal thickening, interstitial fibrosis |
HLA matching and crossmatch:
- HLA typing (by PCR or sequencing) identifies recipient and donor HLA-A, B, C (class I) and DR, DQ, DP (class II) alleles
- Crossmatch test: Donor lymphocytes + recipient serum → if pre-formed antibodies present → positive crossmatch → absolute contraindication to transplant (hyperacute rejection risk)
- Panel reactive antibody (PRA): Measures breadth of anti-HLA sensitisation in recipient; high PRA = harder to find compatible donor
Graft-versus-host disease (GvHD):
- Occurs in bone marrow/HSCT — donor T cells attack recipient tissues
- Acute GvHD: Skin, liver, gut involvement (cytokine storm, CTL-mediated)
- Chronic GvHD: Resembles autoimmune disease (scleroderma-like)
Immunosuppressive drugs in transplantation:
- Calcineurin inhibitors (cyclosporin, tacrolimus): Block IL-2 transcription, suppress T-cell activation
- mTOR inhibitors (sirolimus): Block T-cell proliferation
- Corticosteroids: Broad anti-inflammatory, suppress cytokine production
- Mycophenolate mofetil: Inhibits purine synthesis → suppresses lymphocyte proliferation
- Biologic agents: Basiliximab (anti-IL-2 receptor), belatacept (anti-CD28 co-stimulation blockade)
Tumour Immunology
Tumour Immunology: Surveillance, Antigens and Immune Evasion
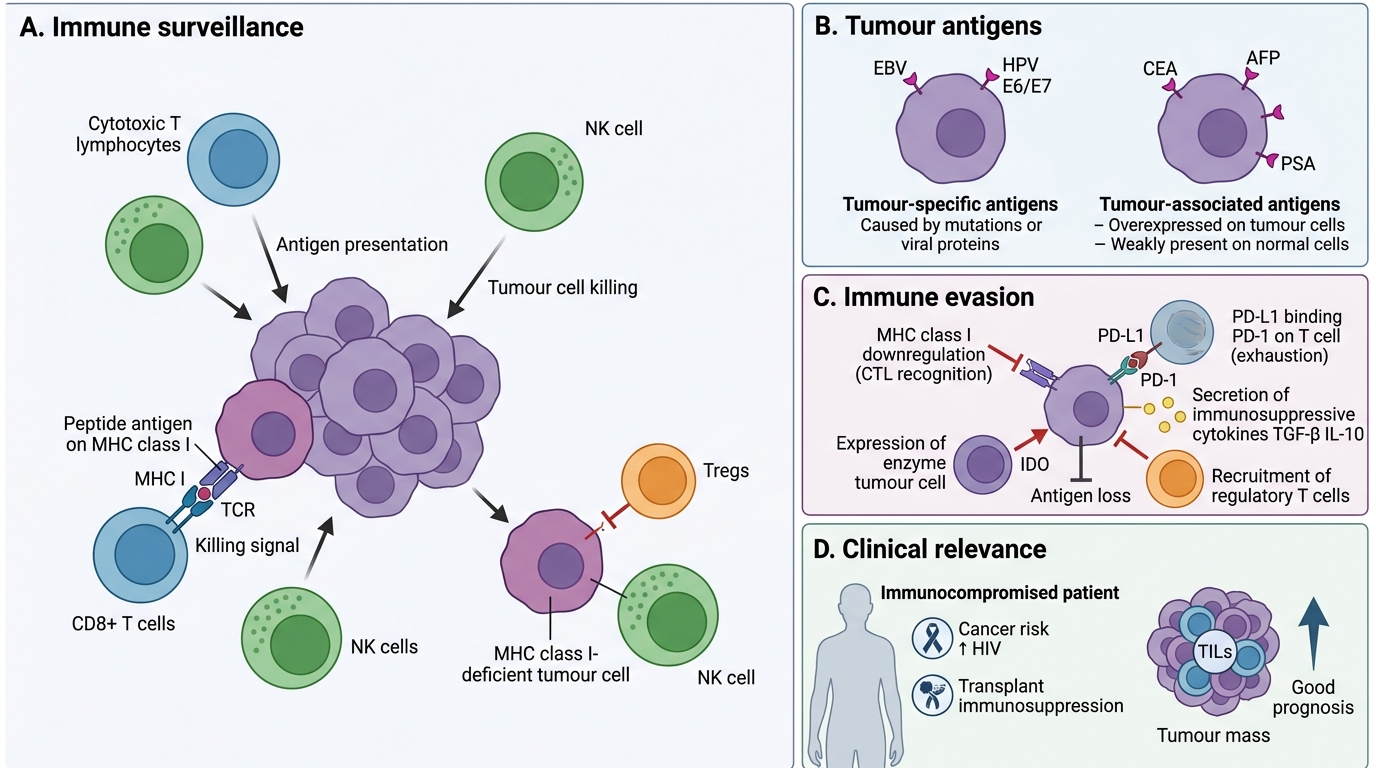
Tumour immunology (cancer immunology) studies how the immune system recognises and destroys malignant cells, and how tumours evade this surveillance.
Tumour antigens:
- Tumour-specific antigens (TSAs): Unique to tumour cells; arise from oncogene mutations, viral proteins (EBV in Burkitt's lymphoma, HPV E6/E7 in cervical cancer)
- Tumour-associated antigens (TAAs): Present on tumour and some normal cells; often overexpressed (e.g., CEA in colon cancer, AFP in hepatocellular carcinoma, PSA in prostate cancer) — used as tumour markers
Immune surveillance (Burnet's theory): The immune system continuously monitors for and eliminates nascent malignant cells. Evidence:
- Immunocompromised patients (HIV, transplant recipients on immunosuppression) have dramatically higher rates of certain cancers (Kaposi's sarcoma, NHL, cervical cancer)
- Tumour-infiltrating lymphocytes (TILs) correlate with better prognosis in many cancers
Mechanisms of tumour immune evasion:
- MHC class I downregulation: Virally infected or mutated cells downregulate MHC I → CTLs cannot recognise them (NK cells can kill MHC I-deficient cells)
- PD-L1 upregulation: Tumours express programmed death ligand-1 (PD-L1), which binds PD-1 on T cells → T-cell exhaustion/anergy
- Immunosuppressive microenvironment: Tumour-secreted TGF-β, IL-10; recruitment of Tregs; IDO expression
- Antigen loss: Tumour cells that lose TSAs escape T-cell killing through immune selection pressure
Cancer immunotherapy (clinically relevant in India's tertiary centres):
- Immune checkpoint inhibitors: Anti-PD-1 (pembrolizumab, nivolumab), anti-CTLA-4 (ipilimumab) — block inhibitory signals, reactivate T cells against tumour
- CAR-T cell therapy: Patient T cells engineered to express chimeric antigen receptor targeting tumour surface molecule (e.g., CD19 in B-ALL)
- Cancer vaccines: HPV vaccines (Cervarix, Gardasil) prevent virus-induced cervical cancer; therapeutic vaccines (sipuleucel-T for prostate cancer)
- Monoclonal antibodies (mAbs): Trastuzumab (anti-HER2 in breast cancer), rituximab (anti-CD20 in B-cell lymphomas) — opsonisation + ADCC

Tumour Immune Evasion and Checkpoint Inhibitor Targets
CLINICAL PEARL
HPV vaccination and cervical cancer prevention in India: Cervical cancer is the second most common female cancer in India, with approximately 123,000 new cases annually. High-risk HPV serotypes (16 and 18) cause >70% of cases. HPV vaccines (available in India's national immunisation programme for adolescent girls aged 9–14 years) generate strong neutralising IgG antibody responses and immunological memory. The E6 and E7 oncoproteins of HPV are tumour-specific antigens — HPV vaccination is thus the clearest example of a cancer-preventing vaccine in clinical practice.