Page 1 of 16
MI2.1-3 | Innate & Adaptive Immunity — Structure and Function — SDL Guide
Learning Objectives
- Explain the roles of innate and adaptive immunity in maintaining health and combating disease.
- Describe the cellular and molecular components of the immune system, including antigens, antibodies, and the complement system.
- Outline the humoral and cellular immune responses mounted against microbial infections.
INSTRUCTIONS
Understanding immunity is foundational for microbiology and clinical medicine. Every infectious disease — and the vaccines that prevent them — operates through these mechanisms. Work through this module actively, pausing at each micro-quiz before reading the explanation.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 9–11 (textbook)
- Robbins & Cotran Pathologic Basis of Disease, Ch 6 (Diseases of Immunity) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-year-old child in rural Rajasthan develops high fever, rash, and blistering sores in the mouth. The family has not vaccinated the child. Within days, the disease spreads to siblings. The older, vaccinated sibling remains completely well. Why does the vaccine protect one child but not the other? The answer lies entirely in understanding how the immune system learns — and remembers — its enemies.
WHY THIS MATTERS
Immunology underpins nearly every domain of medicine you will practise:
- Infectious disease: Whether a pathogen causes mild or severe illness depends on host immunity.
- Vaccination: The entire rationale for immunoprophylaxis rests on immunological memory.
- Autoimmunity and allergy: Aberrant immune responses cause rheumatoid arthritis, SLE, asthma, and anaphylaxis.
- Transplantation and oncology: Rejection of organ grafts and immune evasion by tumour cells are immune phenomena.
In Indian clinical practice, where tuberculosis, typhoid, dengue, and hepatitis B remain endemic, understanding host defence mechanisms is not optional — it is essential.
RECALL
Before proceeding, reflect on what you already know:
- What do white blood cells do in a general sense?
- Have you heard of "B cells" and "T cells"? What do you think they do?
- Why do you think a person who survives chickenpox rarely gets it again?
There are no wrong answers here. This module will build on and sharpen whatever you already know.
The Two Pillars of Immunity: Innate vs Adaptive
Innate vs Adaptive Immunity: The Two Pillars
The immune system operates through two functionally distinct but interconnected arms:
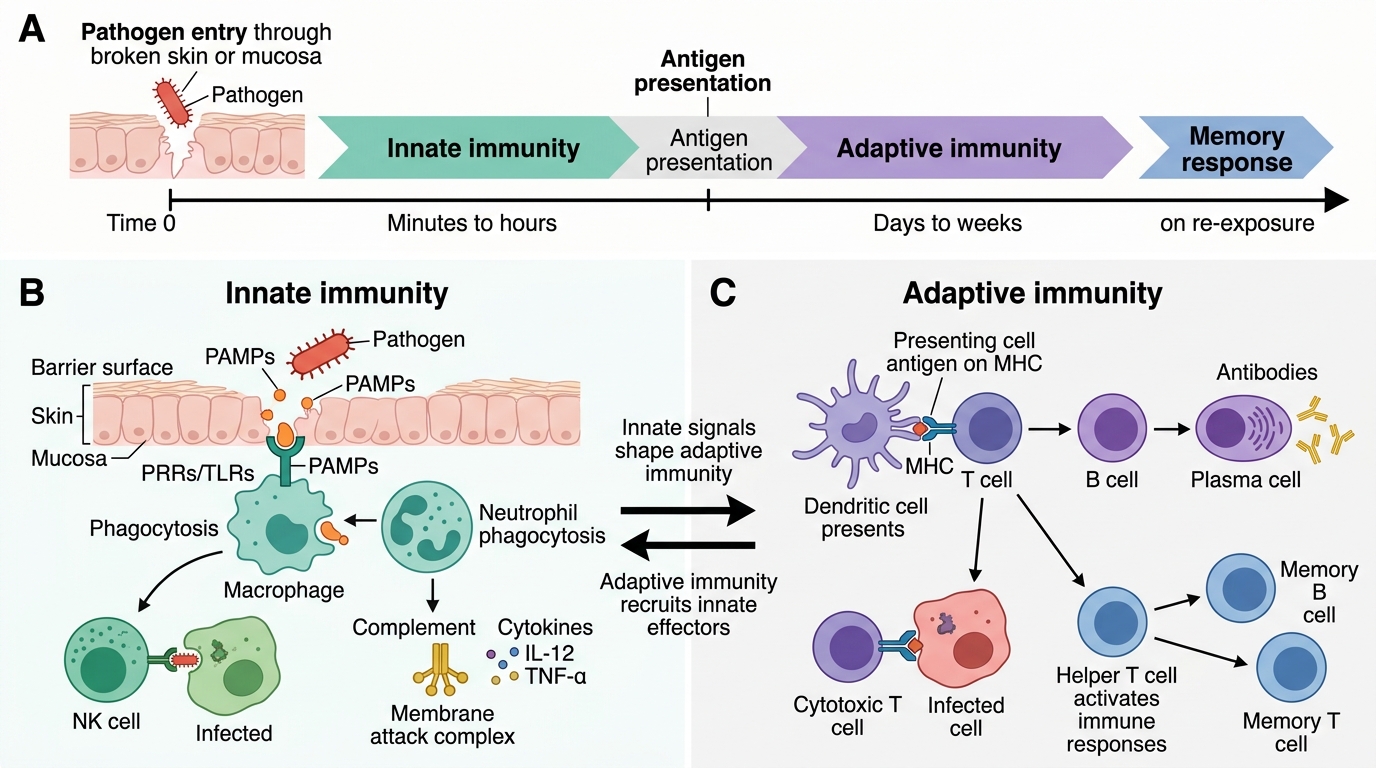
Innate (non-specific) immunity is the body's first line of defence. It acts within minutes to hours, is not antigen-specific, and has no memory. Key features:
- Present from birth
- Recognises broad pathogen-associated molecular patterns (PAMPs) via pattern recognition receptors (PRRs), especially Toll-like receptors (TLRs)
- Components: physical barriers (skin, mucosa), phagocytes (neutrophils, macrophages), natural killer (NK) cells, complement proteins, and cytokines
Adaptive (acquired/specific) immunity develops over days to weeks. It is antigen-specific and generates immunological memory. Key features:
- Acquired through exposure (infection or vaccination)
- Mediated by lymphocytes: B cells (humoral arm) and T cells (cell-mediated arm)
- Hallmarks: specificity, diversity, memory, and self–non-self discrimination
The two systems do not operate in isolation. Innate immune signals (e.g., cytokines like IL-12, TNF-α) activate and shape the adaptive response. Adaptive immunity in turn recruits and activates innate effectors.

Innate vs Adaptive Immunity: Timeline, Components, and Key Features
Antigens: What the Immune System Recognises
Antigens and Immunogenicity
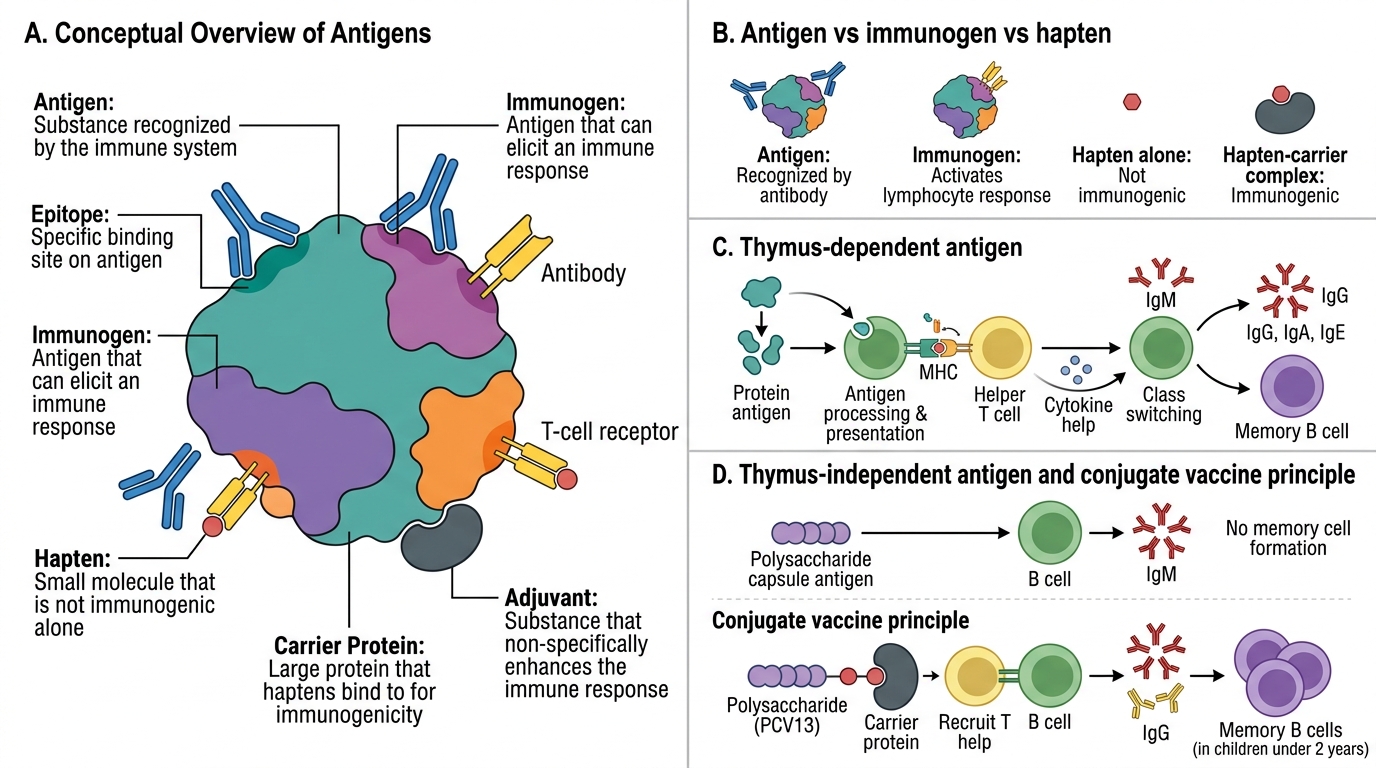
An antigen is any substance that can be specifically recognised by the immune system (lymphocytes or antibodies). Key concepts:
- Immunogen: An antigen capable of inducing an immune response. All immunogens are antigens, but not all antigens are immunogens.
- Epitope (antigenic determinant): The specific region of an antigen that is recognised by an antibody or T-cell receptor. A single antigen molecule carries multiple epitopes.
- Hapten: A small molecule that is antigenic (binds antibody) but not immunogenic alone. Becomes immunogenic when coupled to a carrier protein. Example: penicillin is a hapten — it triggers allergic reactions only after binding to serum proteins.
- Adjuvants: Substances that enhance immunogenicity without being antigens themselves (e.g., alum in vaccines).
Thymus-dependent (TD) antigens: Require T-cell help to elicit antibody production. Most protein antigens are TD. They induce class switching and memory.
Thymus-independent (TI) antigens: Stimulate B cells directly without T-cell help (e.g., polysaccharide capsule antigens). They produce mainly IgM, no memory — which is why polysaccharide vaccines are poorly immunogenic in children under 2 years.
SELF-CHECK
A 14-month-old child receives the Pneumococcal Conjugate Vaccine (PCV13) rather than the older plain polysaccharide vaccine. What is the primary reason for using the conjugate formulation in this age group?
A. Conjugate vaccines are cheaper to manufacture
B. Polysaccharide antigens are T-independent and cannot generate memory in infants under 2 years
C. Plain polysaccharides cause more fever and injection-site reactions
D. PCV13 covers more serotypes than any polysaccharide vaccine
Reveal Answer
Answer: B. Polysaccharide antigens are T-independent and cannot generate memory in infants under 2 years
Polysaccharide antigens are thymus-independent (TI) antigens that stimulate B cells without T-cell help. In children under 2 years, the marginal zone B cells needed for TI responses are immature, so the plain polysaccharide vaccine generates poor antibody responses and no immunological memory. Conjugating the polysaccharide to a carrier protein (e.g., CRM197) converts it to a T-dependent antigen, enabling memory formation and effective protection in infants.
Antibodies: Structure and Function
Antibody Structure and Function
Antibodies (immunoglobulins, Ig) are glycoproteins secreted by plasma cells (differentiated B lymphocytes) in response to antigen stimulation.
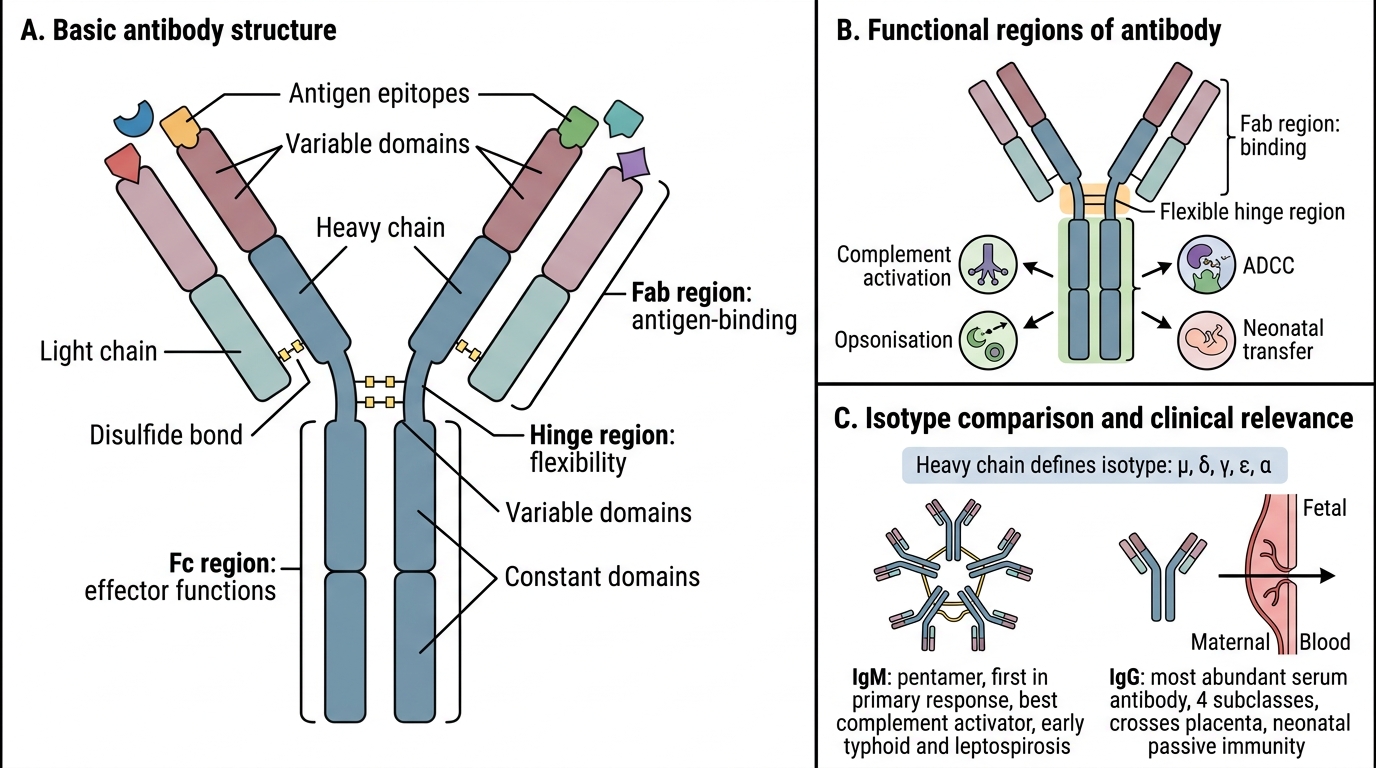
Basic structure: Y-shaped molecule consisting of:
- 2 identical heavy (H) chains and 2 identical light (L) chains linked by disulfide bonds
- Fab region (Fragment antigen-binding): contains the variable (V) domains of H and L chains; this is where antigen binds
- Fc region (Fragment crystallisable): constant domains of H chains; mediates effector functions (complement activation, opsonisation, ADCC, neonatal transfer)
- Hinge region: flexible zone between Fab and Fc; allows bivalent antigen binding
Five classes (isotypes) defined by heavy chain type (μ, δ, γ, ε, α):
| Isotype | Features | Indian clinical relevance |
|---|---|---|
| IgM | Pentamer; first Ab in primary response; best complement activator | Elevated in early typhoid, leptospirosis |
| IgG | Most abundant serum Ab; 4 subclasses; crosses placenta | Passive immunity in neonates |
| IgA | Dimer in secretions (sIgA); mucosal defence | Protects GI and respiratory mucosa |
| IgE | Lowest serum level; mediates Type I hypersensitivity | High in helminth infections, allergy |
| IgD | Mainly B-cell surface receptor | Limited effector function |

Structure of an Antibody and Clinical Serology Correlation
CLINICAL PEARL
IgM elevation in early infection: In clinical practice, a positive IgM serology (e.g., Widal test IgM, dengue NS1 + IgM) indicates recent or acute infection, whereas IgG indicates past infection or vaccination. This distinction guides management — for example, a pregnant woman with IgM anti-rubella antibodies has active infection, posing a risk of congenital rubella syndrome, whereas IgG alone suggests prior immunity.