Page 2 of 16
MI2.1-3 | Innate & Adaptive Immunity — Structure and Function — SDL Guide (Part 2)
The Complement System
The Complement System: Pathways, Functions and Deficiencies
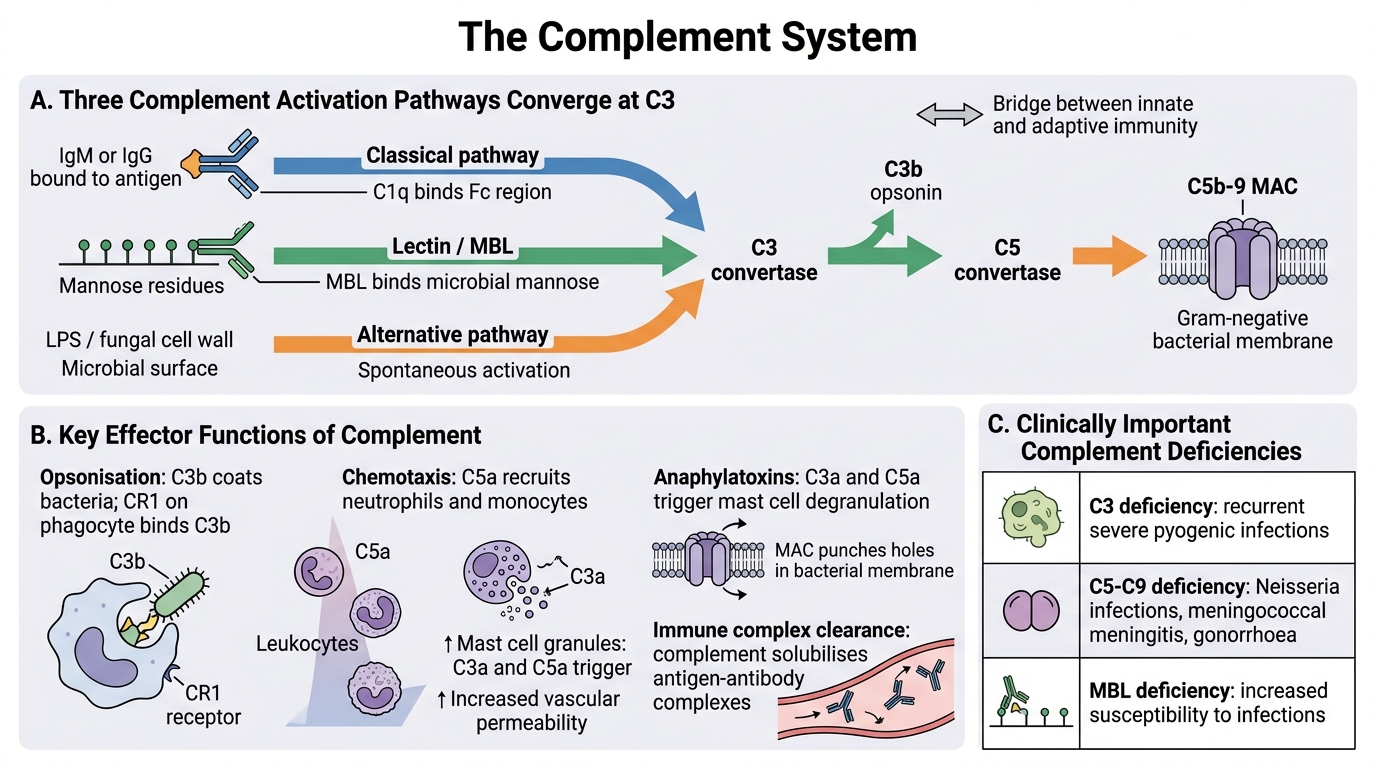
The complement system comprises ~30 serum and membrane proteins that form a proteolytic cascade serving as a bridge between innate and adaptive immunity.
Three activation pathways:
- Classical pathway: Activated by antigen–antibody complexes (IgM or IgG). Requires C1q binding to Fc. Most efficient — amplified by adaptive immunity.
- Lectin (MBL) pathway: Activated by Mannose-Binding Lectin (MBL) binding to mannose residues on microbial surfaces. No antibody required — part of innate immunity.
- Alternative pathway: Activated spontaneously by microbial surfaces (LPS, fungal cell walls). Provides immediate defence without prior sensitisation.
All three pathways converge at C3, producing C3b (opsonin) and generating the membrane attack complex (MAC, C5b-9) which lyses gram-negative bacteria.
Key effector functions:
- Opsonisation: C3b coats bacteria, enhancing phagocytosis (phagocytes have CR1 receptors for C3b)
- Chemotaxis: C5a attracts neutrophils and monocytes to the site of infection
- Anaphylatoxins: C3a and C5a trigger mast cell degranulation and increase vascular permeability
- Lysis: MAC punches holes in bacterial membranes
- Immune complex clearance: Complement helps solubilise and clear antigen–antibody complexes
Complement deficiencies relevant in India:
- C3 deficiency: Recurrent severe pyogenic infections
- C5–C9 deficiency: Susceptibility to Neisseria infections (meningococcal meningitis, gonorrhoea)
- MBL deficiency: Increased susceptibility to early childhood infections

Complement Pathways Converging at C3 and MAC Formation
SELF-CHECK
A 20-year-old male from Assam develops his third episode of meningococcal meningitis in 5 years. Investigation reveals a specific complement deficiency. Which complement component is most likely deficient?
A. C1q
B. C3
C. C4
D. C5 (or a later terminal component)
Reveal Answer
Answer: D. C5 (or a later terminal component)
Deficiencies in terminal complement components C5 through C9 (the components that form the Membrane Attack Complex) predispose specifically to recurrent infections with encapsulated Gram-negative diplococci, particularly Neisseria meningitidis and Neisseria gonorrhoeae. The MAC is essential for lysing the thin peptidoglycan layer of Gram-negative bacteria. C3 deficiency would cause broad susceptibility to pyogenic bacteria, not specifically Neisseria. C1q deficiency predisposes to SLE-like autoimmune disease.
Humoral Immune Response
T-dependent Humoral Immune Response
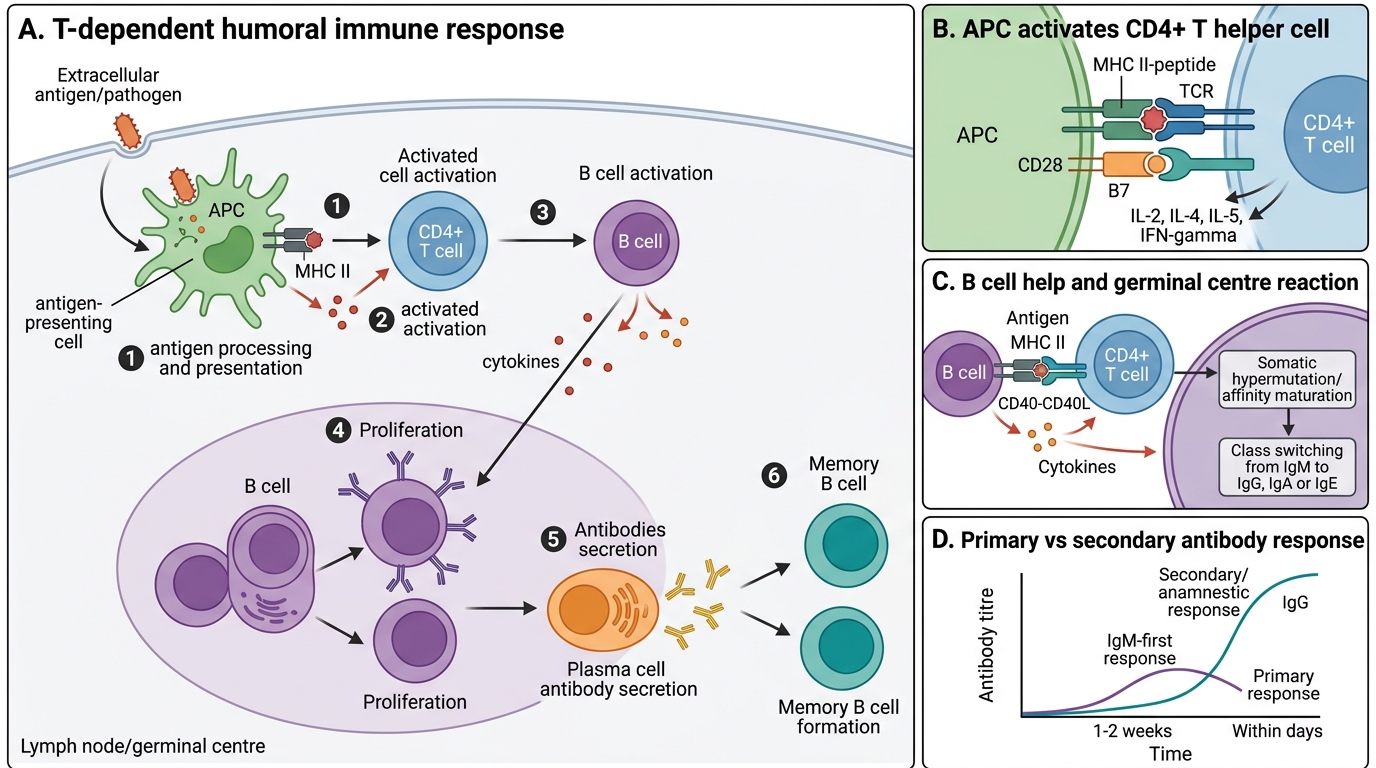
The humoral immune response is mediated by B lymphocytes and the antibodies they produce, targeting extracellular pathogens and toxins.
Sequence of events (T-dependent response):
1. Antigen processing and presentation: Antigen-presenting cells (APCs — dendritic cells, macrophages, B cells) process antigen and present peptide fragments on MHC class II molecules to CD4+ T helper cells.
2. T helper cell activation: CD4+ T cells recognise the MHC II–peptide complex via their TCR. Co-stimulatory signals (CD28–B7 interaction) are required. Activated T cells secrete IL-2 (proliferation), IL-4, IL-5 (B cell activation), and IFN-γ (macrophage activation).
3. B cell activation: B cells present antigen on MHC II to CD4+ T cells and receive T-cell help via CD40L–CD40 interaction and cytokines. This triggers B cell proliferation in germinal centres.
4. Germinal centre reactions:
- Somatic hypermutation: Random mutations in V-region genes generate antibodies with progressively higher affinity (affinity maturation).
- Class switching (isotype switching): B cells switch from producing IgM to IgG, IgA, or IgE depending on cytokine signals.
5. Plasma cells: Long-lived plasma cells secrete large quantities of high-affinity antibodies.
6. Memory B cells: Persist for years; respond rapidly on re-exposure (anamnestic/secondary response).
Secondary (anamnestic) response vs primary response:
- Faster (days vs 1–2 weeks)
- Higher antibody titres
- Predominantly IgG (higher affinity)
- This is the basis of booster vaccination.
Cell-Mediated Immune Response
Cell-Mediated Immune Response
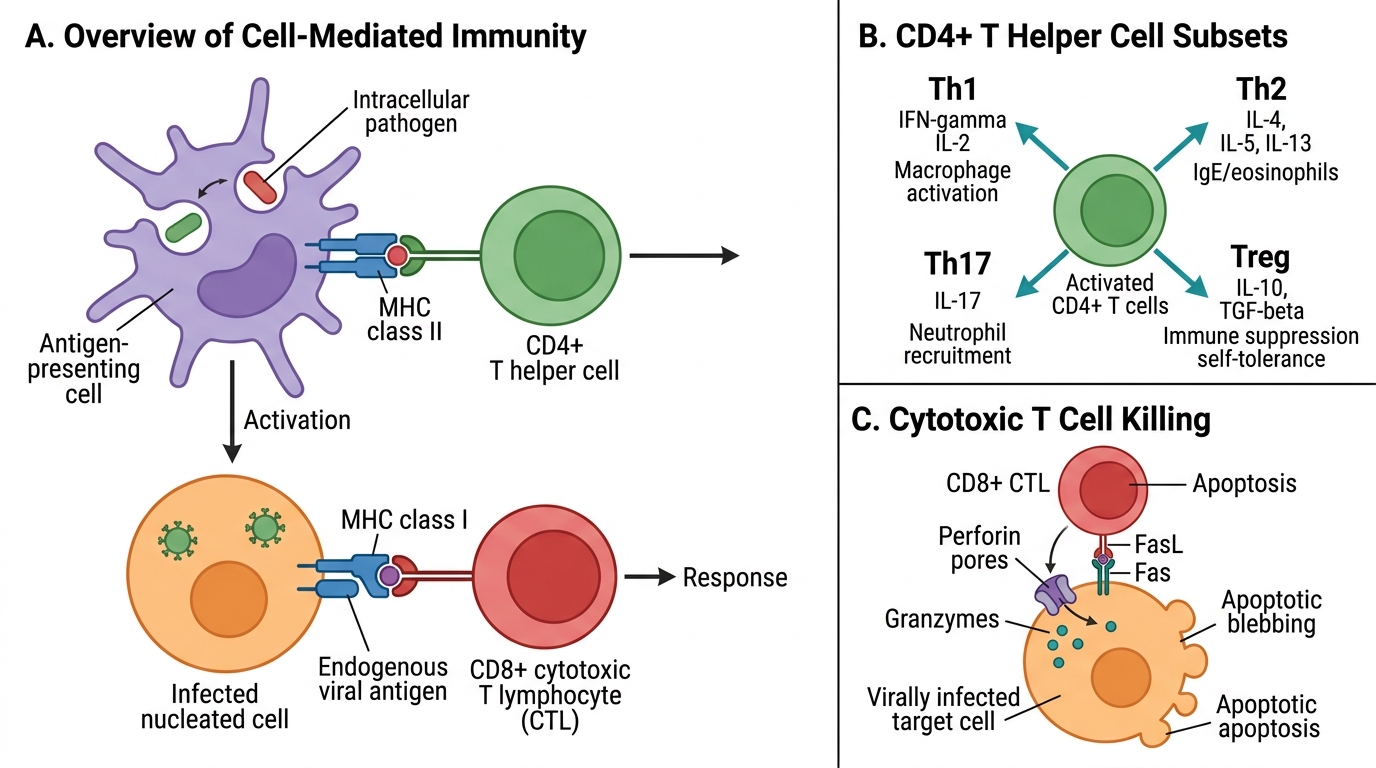
The cell-mediated immune response (CMI) is mediated by T lymphocytes and targets intracellular pathogens (viruses, Mycobacterium tuberculosis, Listeria, fungi) and tumour cells.
Key cell types and their functions:
CD4+ T helper (Th) cells: Orchestrate the immune response. After activation on MHC II, they differentiate into functional subsets:
- Th1: Produce IFN-γ, IL-2 → activate macrophages (essential for killing Mycobacterium tuberculosis), help cytotoxic T cells. Dominated by IL-12 from APCs.
- Th2: Produce IL-4, IL-5, IL-13 → drive B cell responses, IgE production, eosinophil activation. Important in helminth infections and allergy.
- Th17: Produce IL-17 → recruit neutrophils; important in mucosal defence and autoimmunity.
- T regulatory (Treg): Produce IL-10, TGF-β → suppress excessive immune responses; maintain self-tolerance.
CD8+ Cytotoxic T lymphocytes (CTLs): Recognise peptides on MHC class I (expressed by all nucleated cells). Kill virally infected cells and tumour cells by:
- Releasing perforin (pores in target cell membrane) and granzymes (serine proteases triggering apoptosis)
- FasL–Fas interaction (apoptosis induction)
Role of MHC (HLA) molecules:
- MHC class I: Presents endogenous antigens (viral proteins synthesised inside the cell) → recognised by CD8+ CTLs
- MHC class II: Presents exogenous antigens (phagocytosed pathogens) → recognised by CD4+ T helper cells
Mnemonic: "Eight kills One" — CD8 CTLs kill cells via MHC I; CD4 helpers activate via MHC II.
CLINICAL PEARL
HIV and CD4+ T cell depletion: HIV preferentially infects and destroys CD4+ T lymphocytes. As CD4 count falls below 200 cells/μL, CMI collapses — patients become susceptible to opportunistic infections (Pneumocystis jirovecii pneumonia, oesophageal candidiasis, cryptococcal meningitis, CMV retinitis) and AIDS-defining malignancies (Kaposi's sarcoma, primary CNS lymphoma). In Indian practice, TB reactivation is the most common opportunistic infection in HIV/AIDS, as latent TB requires Th1-mediated macrophage activation for control.