Page 4 of 14
MI5.{2,5} | Bone & Joint Infections and Leprosy — SDL Guide
Learning Objectives
- Explain the etiopathogenesis, clinical course, and laboratory diagnosis of bone and joint infections caused by bacterial, fungal, viral, and parasitic agents.
- Describe the etiopathogenesis, clinical course, complications, and laboratory diagnosis of mycobacterial infections involving skin and soft tissue, with special emphasis on sample collection from/of skin — particularly for leprosy.
INSTRUCTIONS
Bone and joint infections demand early recognition: a septic joint is a surgical emergency and untreated osteomyelitis progresses to chronic infection with permanent sequelae. India remains the country with the world's highest number of new leprosy cases (approximately 100,000 per year), making leprosy diagnosis a mandatory clinical competency for every Indian doctor. Understanding its immunopathology explains the wide clinical spectrum from paucibacillary to multibacillary disease.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 34, 35 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients arrive the same week at your district hospital. The first: a seven-year-old boy with fever, pain, and refusal to move his right leg for 48 hours; blood culture grows Staphylococcus aureus; X-ray is normal. The second: a 40-year-old agricultural worker with hypopigmented, anaesthetic patches on his forearm for two years, brought in because a neighbour noticed the patches and insisted he see a doctor. He is embarrassed and has hidden this from his family. What is the microbiological basis of the pain in the first patient? And why is the second patient's skin insensate when the first patient's is exquisitely tender? The answers lie in the contrasting immunological battlegrounds of these two infections.
WHY THIS MATTERS
Bone and joint infections may be haematogenous (bacteraemia seeding metaphysis or synovium) or contiguous (direct extension from wound, surgery, or prosthesis). Failure to aspirate and culture a hot joint within 6 hours risks irreversible cartilage destruction. Leprosy, though slowly progressive, causes irreversible disability through nerve damage — and India has the highest global leprosy burden, making slit-skin smear interpretation a mandatory competency for MBBS and USMLE candidates alike.
RECALL
Before reading on, revisit:
- Basic bone anatomy: cortex, medulla, metaphysis, epiphysis, periosteum. Recall why the metaphysis is the preferred site of haematogenous osteomyelitis (sluggish capillaries, phagocytic gap).
- The granuloma: macrophage → epithelioid cell → Langhans giant cell → central caseation (TB) vs. non-caseating (sarcoid, BCG).
- Mycobacterial staining: Ziehl-Neelsen (ZN) stain — acid-fast bacilli appear red on blue background.
- Innate vs. adaptive immunity: macrophage-based Th1 response (cell-mediated) vs. antibody (Th2); which side determines resistance vs. susceptibility in leprosy?
Osteomyelitis — Pathogenesis & Microbiology
Osteomyelitis: Pathogenesis & Microbiology
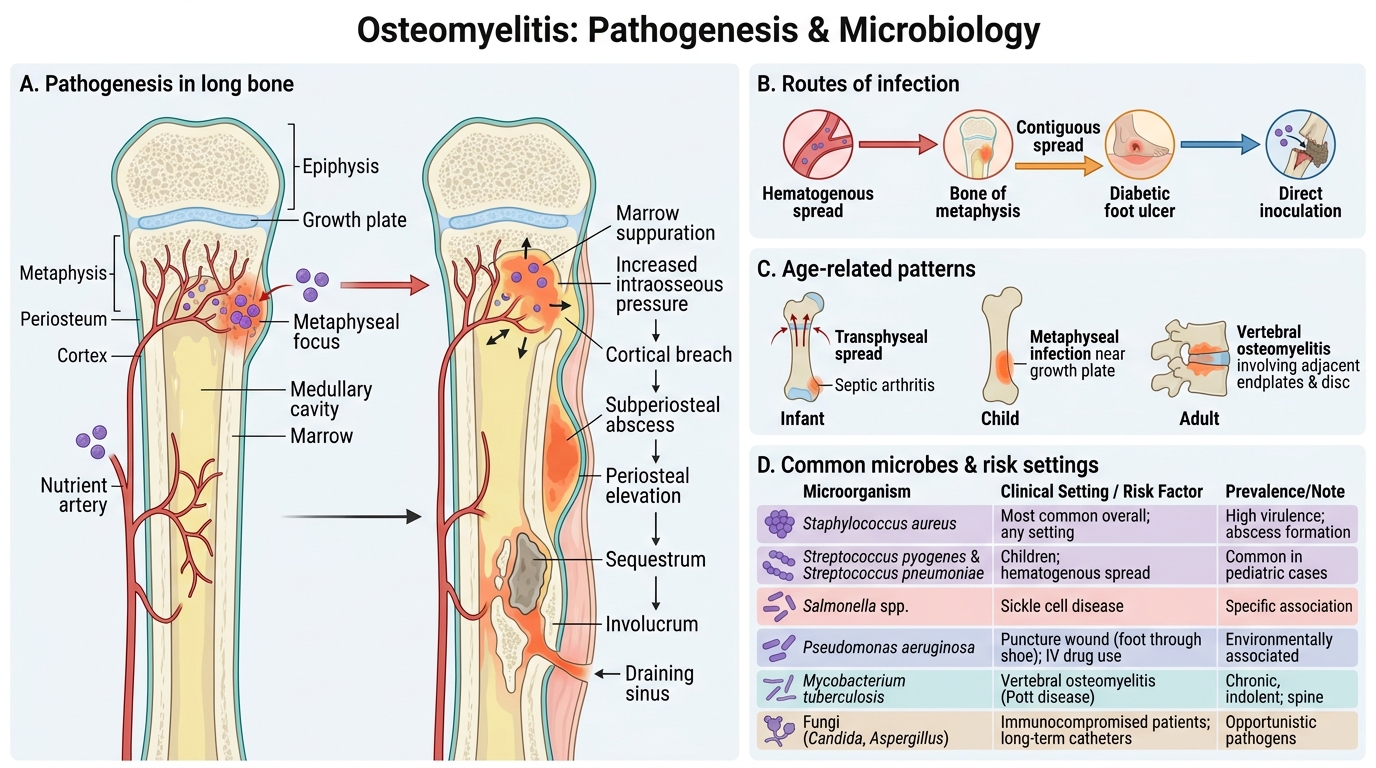
Osteomyelitis is infection of bone, classified by:
- Route: Haematogenous (most common in children) vs. contiguous (adults, post-surgery, diabetic foot) vs. direct inoculation (trauma)
- Duration: Acute (<2 weeks), subacute (2 weeks–3 months), chronic (>3 months, dead bone = sequestrum)
Haematogenous osteomyelitis:
- Children: Metaphysis of long bones (femur, tibia, humerus) — sluggish capillaries in the metaphyseal loop, absence of phagocytic lining cells = bacterial sanctuary
- Adults: Vertebral bodies (vertebral osteomyelitis / spondylodiscitis) — haematogenous via Batson's vertebral venous plexus
- Neonates: Epiphysis and metaphysis both vulnerable; S. aureus + Group B Strep + E. coli
Causative agents by age and context:
| Patient group | Most likely organism |
|---|---|
| Children (1–16 years) | S. aureus (#1 in all ages) |
| Neonates | S. aureus, Group B Strep, Gram-negatives |
| Sickle cell disease | Salmonella spp. (equal to S. aureus) |
| IV drug users | S. aureus, Pseudomonas aeruginosa |
| Diabetic foot | Polymicrobial: S. aureus + Gram-negatives + anaerobes |
| Post-surgical / Prosthetic joint | S. aureus, CoNS (S. epidermidis), Enterococcus |
| Vertebral (Pott's spine) | Mycobacterium tuberculosis |
| Immunocompromised | Candida, Aspergillus, cryptococcosis (bone) |
Pathological progression:
Bacteraemia → metaphyseal seeding → acute inflammation → periosteum elevation (subperiosteal abscess) → pus strips blood supply → devascularised dead bone = sequestrum → new bone around sequestrum = involucrum → chronic osteomyelitis with discharging sinus
Septic Arthritis — Clinical Urgency & Microbiology
Septic Arthritis: Emergency Pathology, Microbiology, and Diagnosis
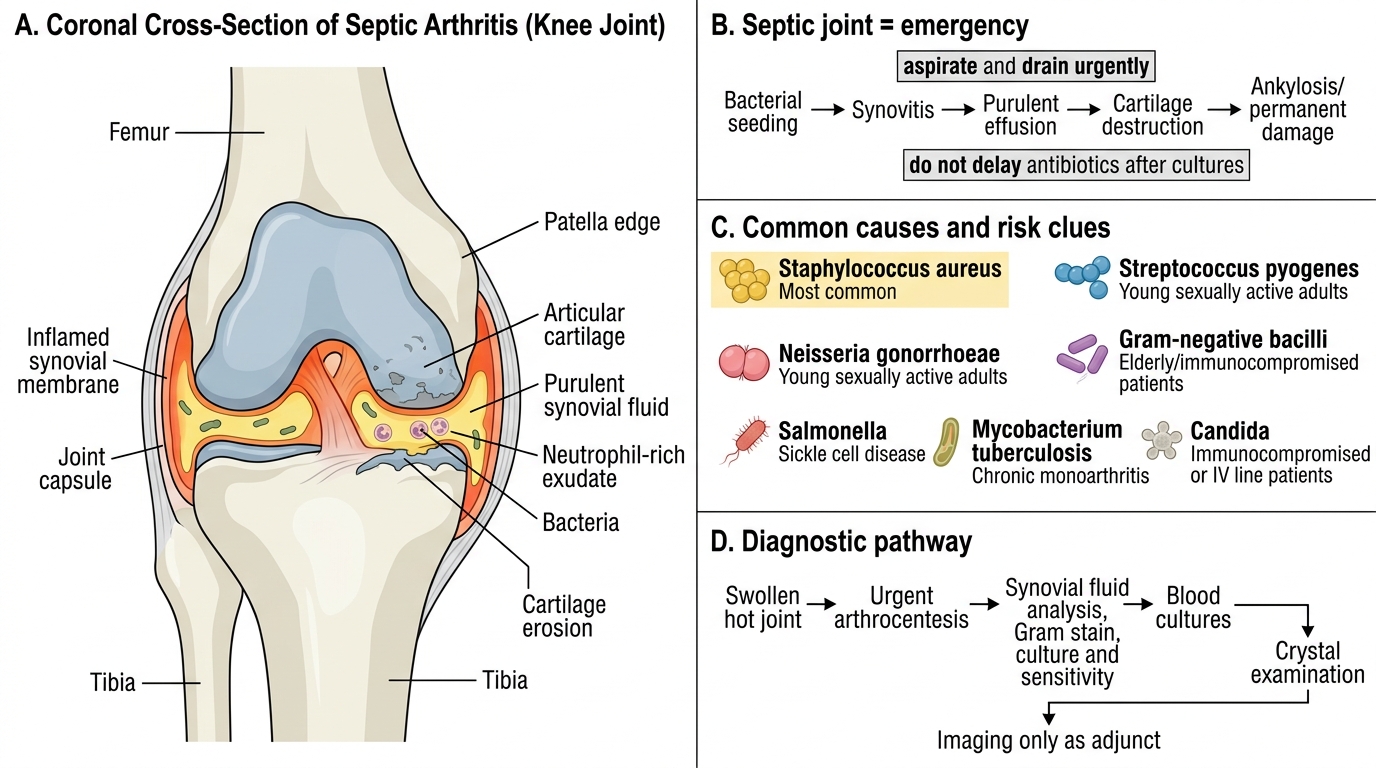
Septic arthritis (infectious arthritis) is a surgical/medical emergency because synovial fluid and proteolytic enzymes destroy cartilage within 4–6 hours of bacterial infection.
Pathogenesis: Haematogenous seeding of synovial membrane (highly vascular, no basement membrane barrier) → bacterial multiplication in synovial fluid → PMN influx → proteolytic enzyme release (matrix metalloproteinases) → cartilage destruction
Common agents:
- Adults <30 years (sexually active): Neisseria gonorrhoeae — most common cause of septic arthritis in sexually active adults in India; polyarticular → oligoarticular → monoarticular progression; skin pustules
- Adults >50 years: S. aureus — monoarticular, large joint (knee, hip)
- Children: S. aureus, H. influenzae (pre-vaccine era), Group A Strep
- Prosthetic joint: S. epidermidis (CoNS), S. aureus, late infections with Propionibacterium (Cutibacterium) acnes
- Reactive arthritis (Reiter's syndrome): Chlamydia trachomatis (genital), Salmonella, Shigella, Campylobacter — joint inflammation is immune-mediated, NOT infective
Diagnosis:
- Joint aspiration (arthrocentesis) is mandatory: synovial fluid WBC >50,000/µL with >75% PMNs = septic until proven otherwise
- Gram stain + culture of synovial fluid
- Blood cultures (positive in 50–70%)
- PCR for gonococcal and Chlamydia if clinically suspected
Treatment: IV antibiotics (anti-staphylococcal + Gram-negative cover pending culture) + joint washout/drainage — delay of even hours worsens outcome
SELF-CHECK
A 12-year-old child with sickle cell disease presents with fever and pain over the left tibia for 5 days. X-ray shows periosteal elevation. Blood culture is ordered. Which organism is MOST likely to be isolated in this specific patient?
A. Staphylococcus aureus
B. Salmonella spp.
C. Streptococcus pyogenes
D. Pseudomonas aeruginosa
Reveal Answer
Answer: B. Salmonella spp.
In sickle cell disease, Salmonella spp. is classically the most common cause of osteomyelitis — equal to or exceeding S. aureus. The mechanism: haemolysed sickle cells release haem, which promotes Salmonella growth; functional asplenia (from autosplenectomy in repeated splenic infarcts) impairs clearance of opsonised Gram-negative bacteria, and Salmonella thrive in the infarcted bone microenvironment. S. aureus remains the overall most common organism in osteomyelitis, but the sickle cell–Salmonella association is a classic examination distinction.
Fungal, Viral, and Parasitic Bone/Joint Infections
Fungal, Viral, and Parasitic Bone/Joint Infections
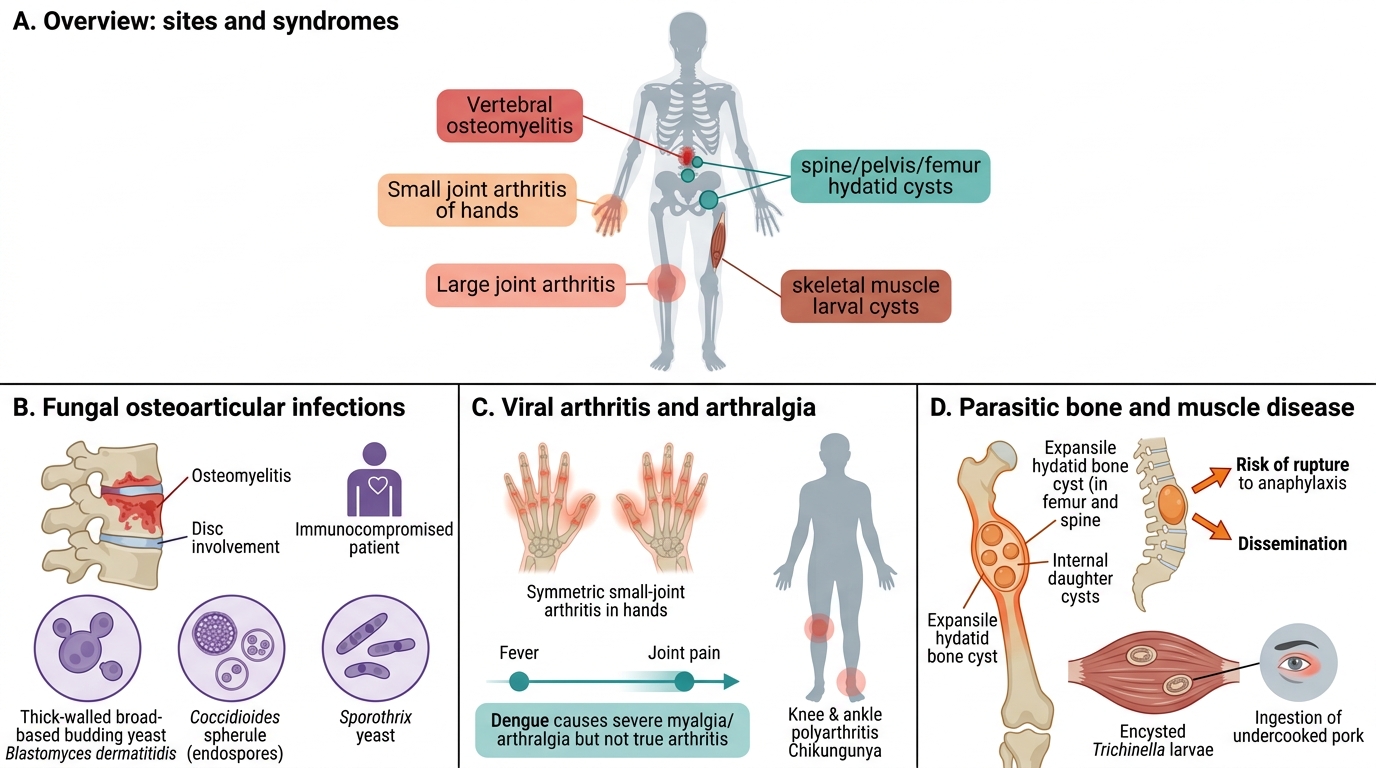
Fungal bone and joint infections:
- Pott's disease analogue: Aspergillus, Candida, Cryptococcus — vertebral osteomyelitis in immunocompromised (HIV, post-transplant, haematological malignancy)
- Blastomycosis (Blastomyces dermatitidis): Bone lesions (lytic) in 25–60% of disseminated cases; thick-walled broad-based budding yeast
- Coccidioidomycosis (Coccidioides immitis): Bone, joint, meningitis in disseminated disease; arthroconidia inhaled; spherule with endospores in tissue
- Sporotrichosis: Arthritis (wrist, elbow, knee) in disseminated form, particularly in immunocompromised; cigar-shaped yeast
Viral arthritis:
- Rubella, Parvovirus B19, Hepatitis B (immune complex): Symmetric small joint arthritis, self-limiting
- Chikungunya virus: Debilitating polyarthritis; often chronic and incapacitating in India; arthritis persists months after fever resolves
- Dengue: Bone pain ('breakbone fever') — severe myalgia/arthralgia, NOT true arthritis
- HIV: Reactive arthritis, septic arthritis (opportunistic agents), avascular necrosis
Parasitic bone/joint disease:
- Hydatid cyst (Echinococcus granulosus): Bone cyst (spine, pelvis, femur) — slowly enlarging; rupture causes anaphylaxis + secondary dissemination; treat with albendazole + surgery
- Trichinosis (Trichinella spiralis): Myositis + periorbital oedema after undercooked pork; larvae encyst in muscle
- Visceral leishmaniasis (Kala-azar): Bone marrow infiltration by Leishmania donovani; no true joint disease but severe myalgia + pancytopenia