Page 5 of 14
MI5.{2,5} | Bone & Joint Infections and Leprosy — SDL Guide (Part 2)
Leprosy — Mycobacterium leprae (MI5.5)
Leprosy: Biology, Transmission, Immunity and Clinical Spectrum
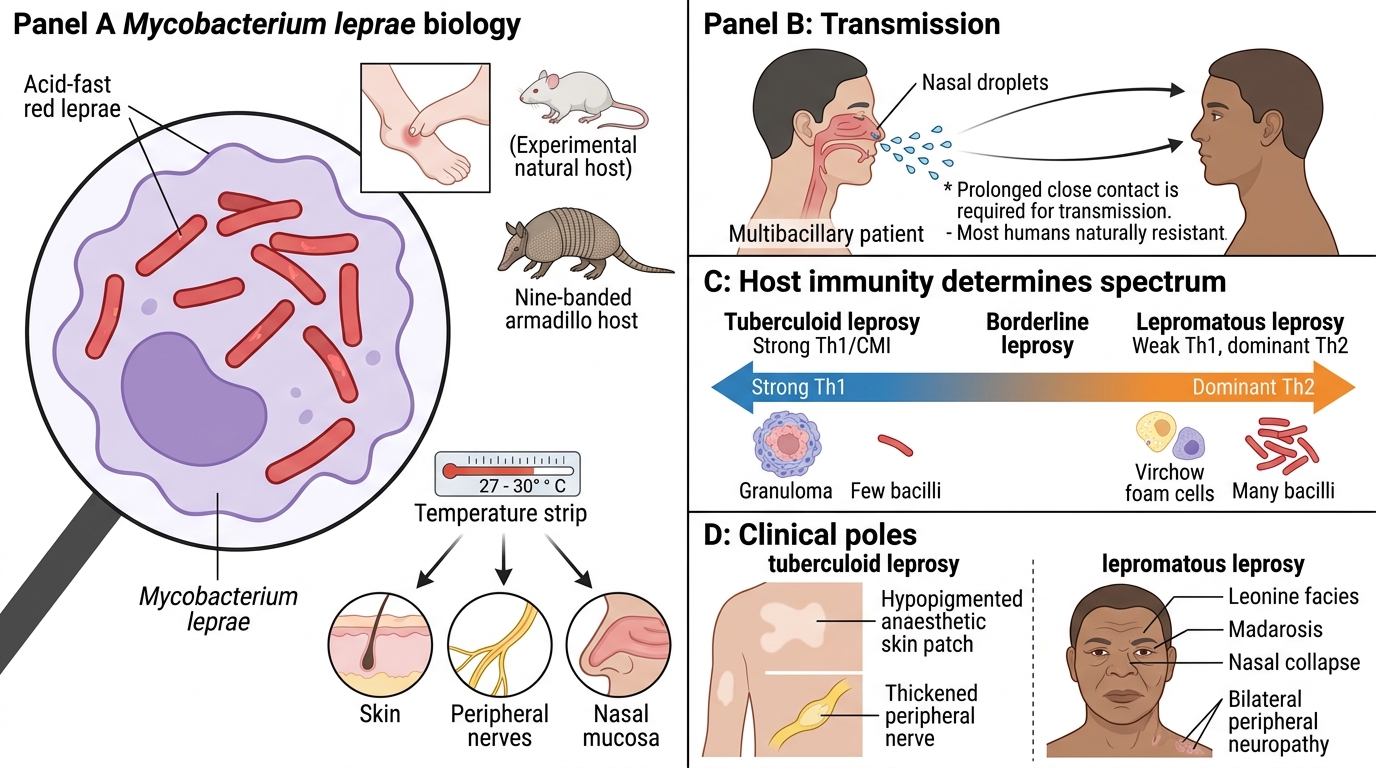
Mycobacterium leprae is an obligate intracellular, acid-fast, Gram-positive rod that:
- Cannot be cultured in vitro (no artificial medium supports its growth)
- Grows in foot-pads of mice (experimental model) and naturally infects nine-banded armadillos (Dasypus novemcinctus)
- Grows at 27–30°C (cooler temperature) — explains preference for skin, peripheral nerves, nasal mucosa (cooler areas)
- Generation time: ~12–14 days (slowest of all human pathogens)
Epidemiology: India has the world's highest leprosy burden (~100,000 new cases/year); 2024 targets elimination; Odisha, UP, Chhattisgarh, Maharashtra highest endemic states.
Transmission: Primarily via nasal droplets from multibacillary (lepromatous) patients; prolonged close contact; NOT highly contagious (95% of humans are naturally resistant). Incubation period 3–10 years.
Pathogenesis: The clinical spectrum is determined by the host immune response (Th1 vs. Th2):
- Tuberculoid leprosy (TT): Strong Th1 (CMI) → granuloma formation → localised nerve damage → few bacteria (paucibacillary) → hypopigmented anaesthetic patches + palpable peripheral nerve thickening
- Lepromatous leprosy (LL): Weak Th1, dominant Th2 (humoral) → no granuloma → macrophages stuffed with bacilli (Virchow cells, foam cells) → multibacillary → leonine facies, madarosis, nasal collapse, bilateral peripheral neuropathy
- Borderline (BT, BB, BL): Intermediate, unstable immunological spectrum
Leprosy — Clinical Features, Nerve Damage & Complications
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Leprosy: Clinical Features, Nerve Damage and Complications
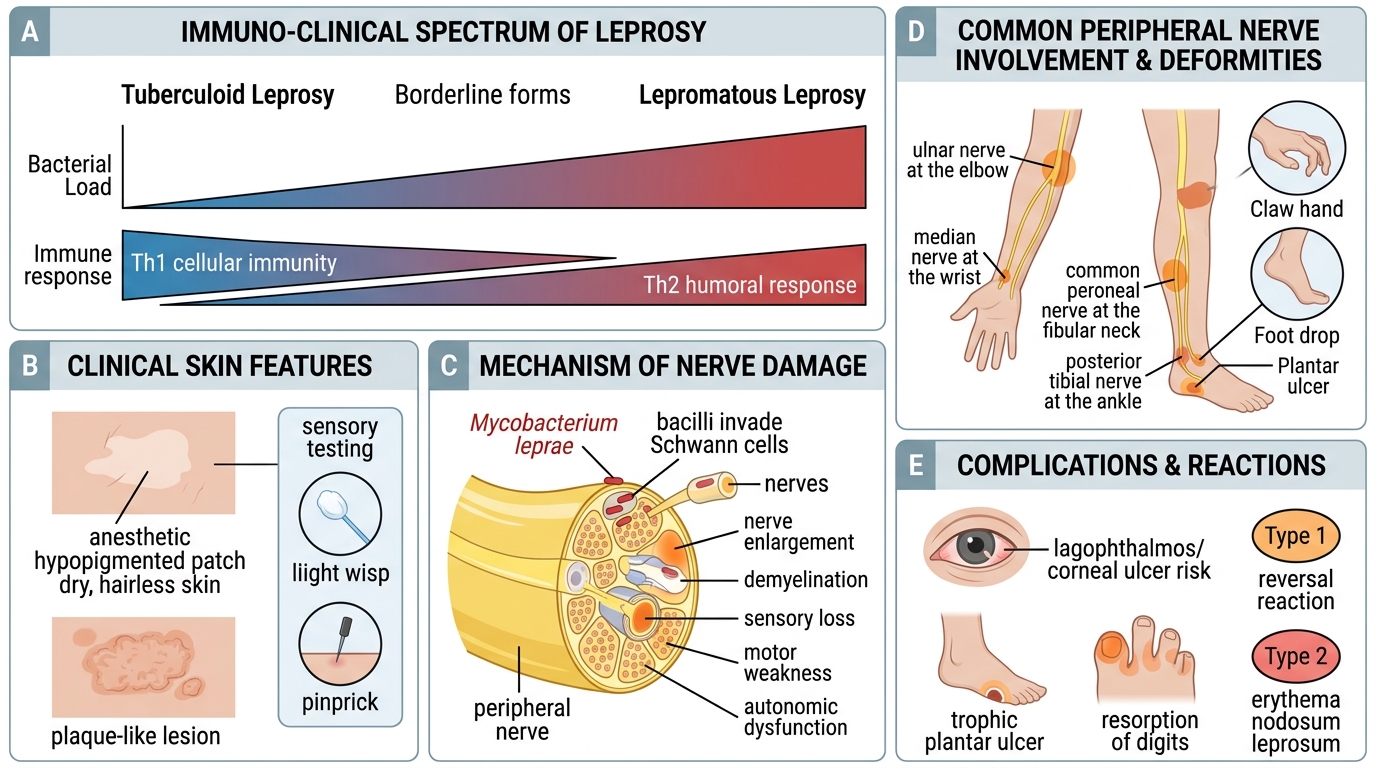
Skin lesions:
- Tuberculoid: 1–5 well-defined, hypopigmented, anaesthetic, dry, hairless patches; raised edges
- Lepromatous: Numerous, poorly defined, symmetric, infiltrated plaques and nodules; sensation INTACT (nerves not yet damaged in early LL)
- Borderline: Features of both
Peripheral nerve involvement (unique to leprosy):
- Superficially located nerves are selectively affected (cooler = preferred temp for M. leprae):
- Great auricular nerve
- Ulnar nerve (at elbow) → claw hand (4th, 5th fingers)
- Median nerve (at wrist) → thumb opposition loss
- Common peroneal nerve (at knee) → foot drop
- Radial nerve → wrist drop
- Facial nerve (in TT, leprosy reactions)
- Posterior tibial nerve → plantar anaesthesia → neuropathic ulcers
Complications:
- Lagophthalmos (corneal exposure) → blindness
- Trophic ulcers → secondary infection → osteomyelitis → bone resorption ("pointing" of fingers)
- Reactive states:
- Lepra type 1 (reversal reaction): Upgrading of CMI in borderline; nerve damage can be acute; treat with prednisolone
- Lepra type 2 (ENL — erythema nodosum leprosum): Immune complex deposition in LL/BL; tender skin nodules + fever; treat with clofazimine/thalidomide
Laboratory Diagnosis of Leprosy — Slit-Skin Smear (MI5.5)
Slit-Skin Smear for Laboratory Diagnosis of Leprosy
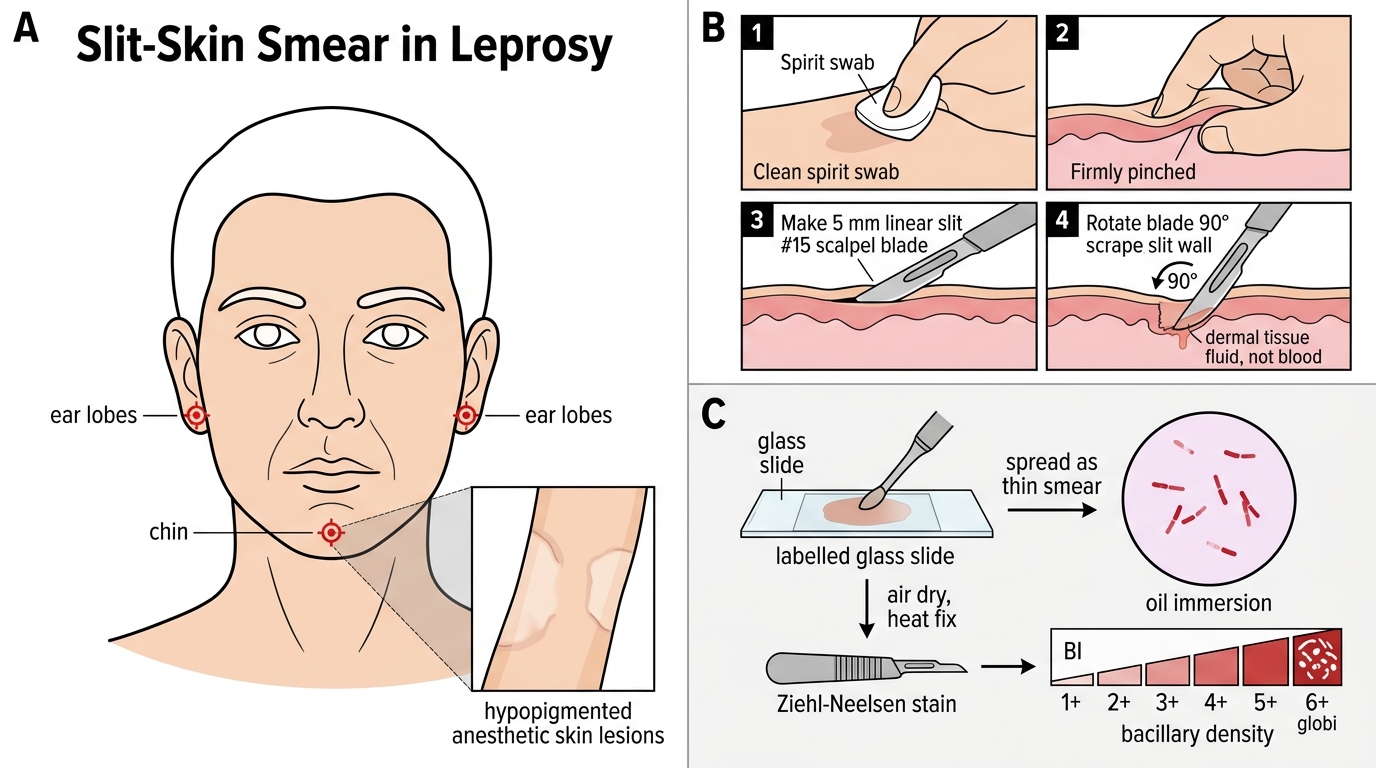
Slit-skin smear (SSS) is the cornerstone of leprosy diagnosis and bacillary load assessment:
Collection sites: Ear lobes (both), chin, lesional skin edges — 4–6 sites standard.
Technique:
1. Clean skin with spirit swab
2. Pinch skin firmly between thumb and index finger to expel blood from site
3. Make a 5 mm linear incision (slit) through epidermis into dermis with a #15 blade
4. Rotate the blade 90° and scrape the walls of the slit to obtain dermal tissue fluid (NOT blood)
5. Spread material on labelled glass slide
6. Air dry → fix → Ziehl-Neelsen stain
Smear grading — Bacteriological Index (BI):
| BI | Bacilli per oil immersion field |
|---|---|
| 1+ | 1–10 per 100 fields |
| 2+ | 1–10 per 10 fields |
| 3+ | 1–10 per field |
| 4+ | 10–100 per field |
| 5+ | 100–1000 per field |
| 6+ | >1000 per field (globi visible) |
Morphological Index (MI): % solid-staining (viable) bacilli. BI does not change rapidly with treatment; MI falls first as treatment kills bacilli.
Histopathology (skin biopsy):
- Tuberculoid: Well-formed granulomas with epithelioid cells + Langhans giant cells; few or no bacilli; epidermal erosion
- Lepromatous: Virchow cells (foam cells) = lipid-laden macrophages packed with bacilli; clear Grenz zone (normal tissue) between epidermis and granuloma; no Langhans giant cells

Lepromatous Leprosy: ZN Smear, Globi, BI and Immune Response
SELF-CHECK
A patient with suspected leprosy has a slit-skin smear showing Bacteriological Index of 3+ from ear lobes and 2+ from a cheek lesion. Histopathology shows numerous lipid-laden macrophages ('foam cells') packed with bacilli and a clear Grenz zone. What type of leprosy does this represent, and what is the predominant immune response?
A. Tuberculoid leprosy with strong Th1 (cell-mediated) immune response
B. Lepromatous leprosy with weak Th1 and dominant Th2 (humoral) immune response
C. Borderline tuberculoid leprosy with mixed Th1/Th2 response
D. Indeterminate leprosy with early undifferentiated immune response
Reveal Answer
Answer: B. Lepromatous leprosy with weak Th1 and dominant Th2 (humoral) immune response
The combination of high bacillary index (BI 3+), foam cells (Virchow cells) packed with bacilli, and a clear Grenz zone on histopathology is diagnostic of lepromatous leprosy (LL). In LL, there is weak or absent Th1 (cell-mediated) immunity — macrophages cannot kill M. leprae — and dominant Th2 (humoral/antibody) response that is ineffective against intracellular organisms. This allows unrestricted bacillary multiplication, producing multibacillary disease. Tuberculoid leprosy (TT) shows strong Th1, well-formed granulomas, and very few or absent bacilli.