Page 4 of 13
MI7.{2-3,5} | Lower Respiratory Tract Infections — SDL Guide
Learning Objectives
- Explain the etiopathogenesis, laboratory diagnosis and prevention of lower respiratory tract infections (LRTIs) caused by bacterial, mycobacterial, viral, fungal and parasitic agents
- Enumerate and identify etiological agents in specific clinical situations: age groups, immune status, community-acquired pneumonia (CAP) and hospital-acquired pneumonia (HAP)
- Identify common etiological agents of LRTIs from Gram stain and Acid-fast stain of sputum/BAL/tracheal aspirate and correlate with clinical findings
INSTRUCTIONS
Pneumonia kills more children under 5 than any other infectious disease globally, and tuberculosis remains the number one infectious disease killer in India. This SDL equips you to approach a patient with cough, fever and breathlessness with a systematic microbiological framework.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 27 (Pneumococcus), Ch 30 (Mycobacterium), Ch 54–56 (Respiratory Viruses, Influenza), Ch 62 (Pneumocystis, Aspergillus) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 55-year-old diabetic man, retired factory worker, presents with 3 months of low-grade fever, evening sweats, weight loss and a productive cough with blood-streaked sputum. Chest X-ray shows a right upper lobe cavitary lesion. His 10-year-old grandson who lives with him has been coughing for 2 weeks. What is your first priority investigation, and what infection control measure should be implemented immediately in the family?
WHY THIS MATTERS
India bears the world's highest tuberculosis burden (~26% of all global TB cases). Beyond TB, LRTIs — pneumonia, bronchitis, lung abscess — are leading causes of hospital admissions and ICU mortality. Identifying the causative agent guides antibiotic choice, prevents spread, and in the case of TB, triggers contact tracing under RNTCP (now NI-KSHAY programme). You will encounter LRTI at every level of care.
RECALL
Before proceeding, recall: (1) The Ziehl-Neelsen (ZN) acid-fast stain principle — mycobacteria retain carbol fuchsin after acid-alcohol decolourisation due to mycolic acid in their cell wall. (2) The difference between primary complex and post-primary TB. (3) CAP = pneumonia acquired outside hospital or within 48 hr of admission; HAP = pneumonia ≥48 hr after hospital admission. (4) The Gram-stain morphology of S. pneumoniae (Gram+ve diplococci lancet-shaped).
Overview: LRTI Pathogens by Host and Setting (MI7.3)
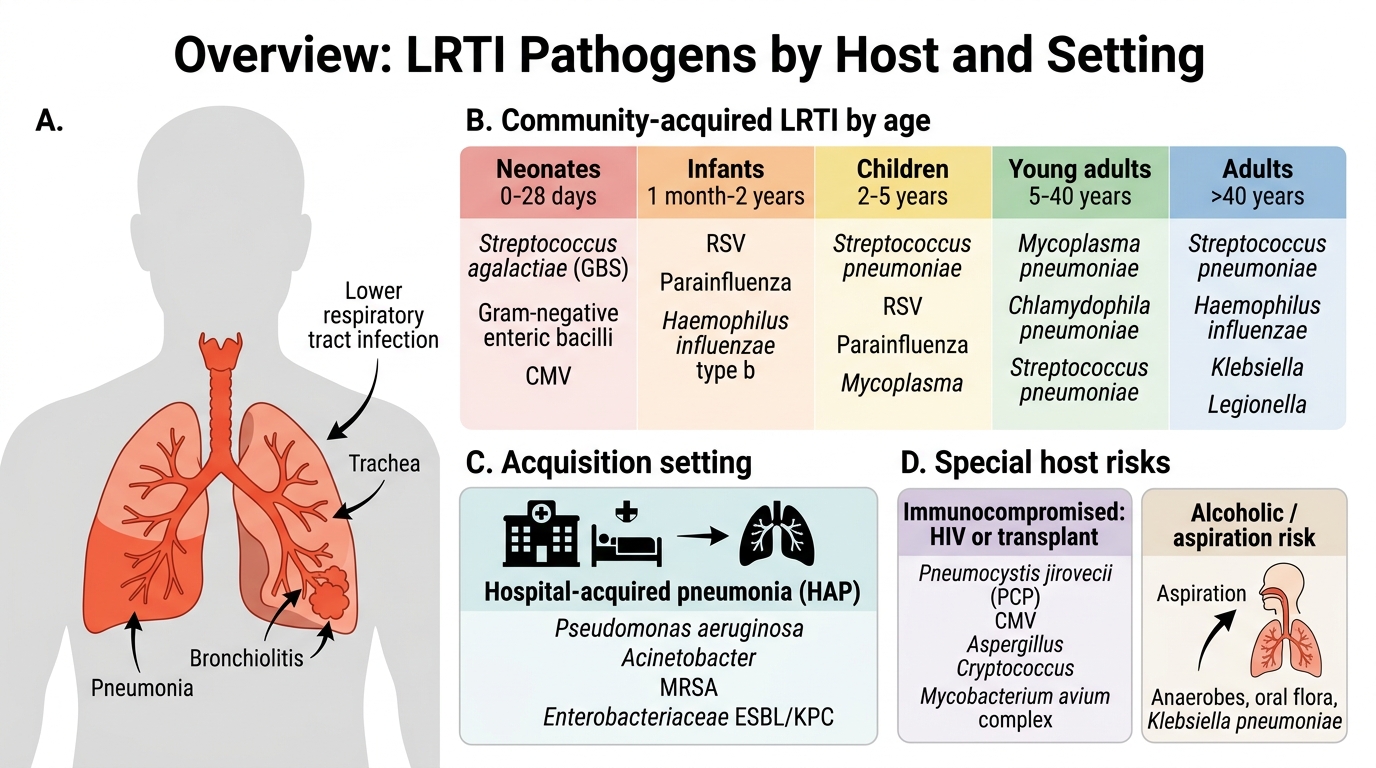
LRTI Pathogens by Host and Setting
Aetiology depends critically on host age, immune status and acquisition setting:
| Clinical Situation | Key Pathogens |
|---|---|
| Neonates (0–28 days) | Streptococcus agalactiae (GBS), Gram-negative enteric bacilli, CMV |
| Infants (1 mo–2 yr) | RSV (bronchiolitis), Parainfluenza, H. influenzae type b |
| Children (2–5 yr) | S. pneumoniae, RSV, Parainfluenza, Mycoplasma |
| Young adults (5–40 yr) | Mycoplasma pneumoniae (walking pneumonia), Chlamydophila pneumoniae, S. pneumoniae |
| Adults >40 yr (CAP) | S. pneumoniae (most common overall), H. influenzae, Klebsiella, Legionella |
| Hospital-acquired (HAP) | Pseudomonas aeruginosa, Acinetobacter, MRSA, Enterobacteriaceae (ESBL/KPC) |
| Immunocompromised (HIV, transplant) | Pneumocystis jirovecii (PCP), CMV, Aspergillus, Cryptococcus, Mycobacterium avium complex |
| Alcoholic / aspiration | Klebsiella pneumoniae (Friedlander's), anaerobes, S. aureus |
| Cystic fibrosis | Pseudomonas aeruginosa (mucoid), Burkholderia cepacia |
Bacterial Pneumonias — Major Pathogens
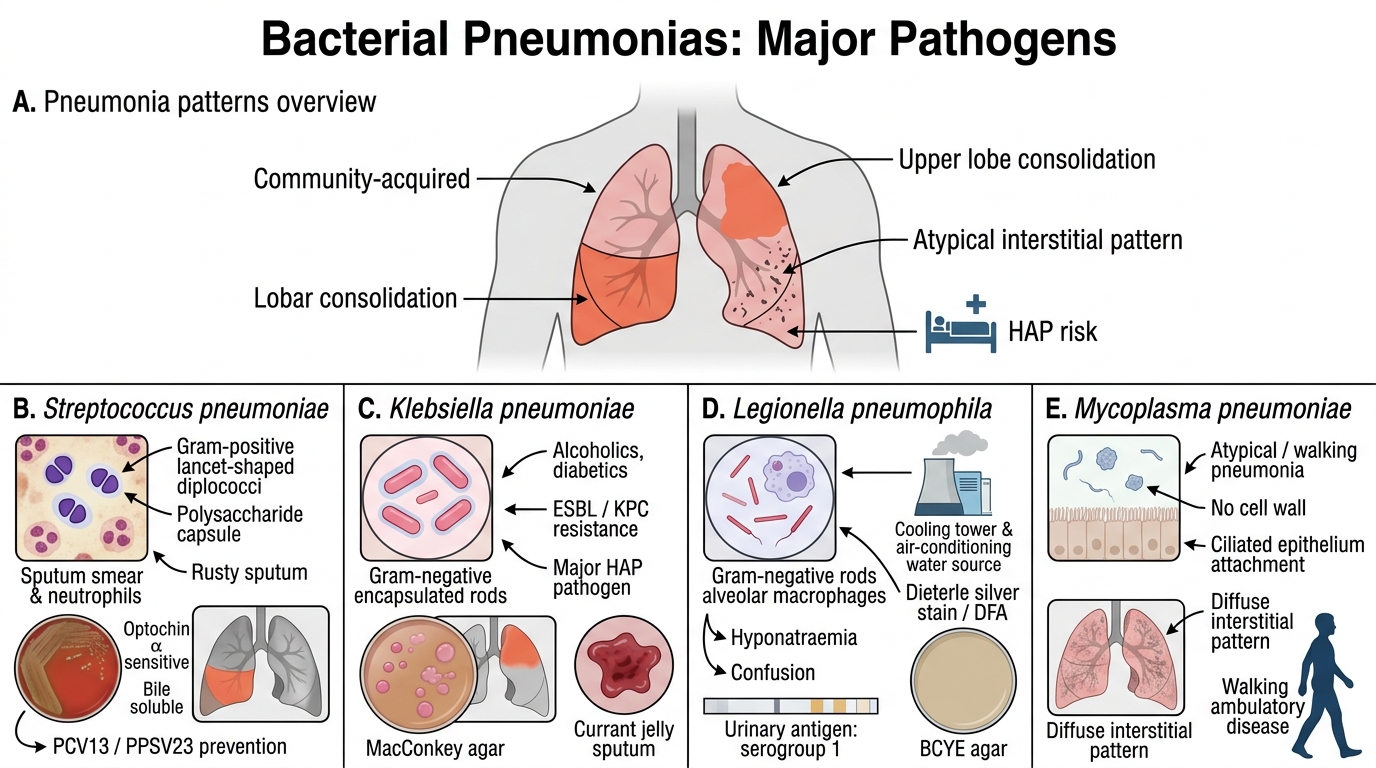
Major Bacterial Pneumonia Pathogens
1. Streptococcus pneumoniae (Pneumococcus) — commonest cause of CAP
- Gram-positive, lancet-shaped diplococci encapsulated; α-haemolytic
- Virulence: polysaccharide capsule (anti-phagocytic; 90+ serotypes); pneumolysin; IgA protease
- Pneumococcal pneumonia: lobar consolidation, rusty sputum (haematin), pleuritic chest pain
- Lab: Sputum Gram stain (Gram+ve diplococci in PMN background); culture on blood agar (draughtsman colonies with α-haemolysis); optochin sensitivity; bile solubility test
- Prevention: PCV13 (conjugate, children in UIP) + PPSV23 (polysaccharide, adults >65, immunocompromised)
2. Klebsiella pneumoniae — Friedlander's pneumonia
- Gram-negative encapsulated rod; lactose fermenter on MacConkey; mucoid colonies
- Classic: alcoholics, diabetics; upper lobe consolidation with currant jelly sputum (blood-stained, viscous)
- Drug-resistant strains: ESBL, KPC — major HAP pathogen
3. Legionella pneumophila
- Gram-negative rod, poorly staining; MUST use Dieterle silver stain or direct fluorescent antibody (DFA)
- Intracellular; replicates in alveolar macrophages; associated with water cooling towers, air-conditioning units
- Legionnaire's disease: severe pneumonia + hyponatraemia + diarrhoea + confusion
- Diagnosis: urinary antigen test (rapid, detects serogroup 1); culture on BCYE agar (buffered charcoal yeast extract)
4. Mycoplasma pneumoniae — atypical/walking pneumonia
- No cell wall → Gram stain negative; cannot be seen on Gram stain
- Interstitial pneumonia; disproportionately mild symptoms; young adults, closed communities
- Diagnosis: Cold agglutinins (IgM); Eaton agent grown on SP4 medium; serology (IgM); PCR (best)

Pneumococcal CAP: Sputum Gram Stain and Clinical Pearls
CLINICAL PEARL
Atypical pneumonia triad: Mycoplasma, Chlamydophila, Legionella do NOT respond to beta-lactam antibiotics (no cell wall target for Mycoplasma; intracellular for the rest). Use macrolides (azithromycin) or fluoroquinolones (levofloxacin) — this is a high-yield prescribing pearl for intern-level clinical decision making.
Tuberculosis (Mycobacterium tuberculosis)
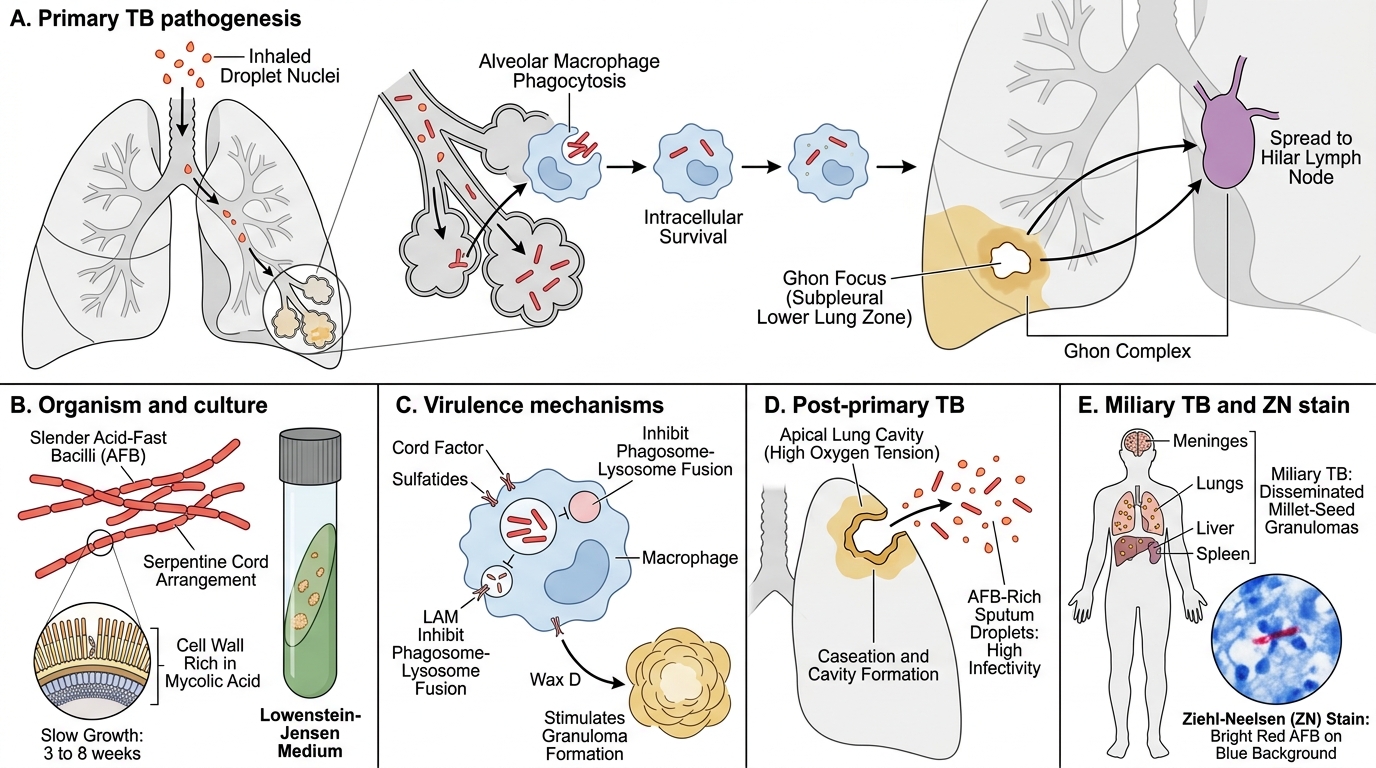
Tuberculosis: Organism, Pathogenesis, and Diagnosis
Organism: Mycobacterium tuberculosis — aerobic, non-motile, non-sporing, acid-fast bacillus (AFB); rich in mycolic acid; slow growing (generation time 18 hr; grows in 3–8 weeks on LJ medium).
Virulence factors:
- Cord factor (trehalose dimycolate) — inhibits phagosome-lysosome fusion; responsible for serpentine cord arrangement
- Sulfatides — inhibit phagolysosome fusion
- Wax D — adjuvant property, stimulates granuloma formation
- LAM (lipoarabinomannan) — inhibits IFN-γ signalling
Etiopathogenesis:
1. Primary TB: Inhaled droplet nuclei (1–5 µm) reach alveoli → phagocytosed by alveolar macrophages but resist killing → intracellular multiplication → Ghon focus (subpleural lower zone) + hilar lymph node → Ghon complex (primary complex). Most primary TB self-heals and calcifies.
2. Post-primary (reactivation) TB: Reactivation at apex (high O₂ tension) → caseation → cavity formation → AFB-rich sputum → highly infectious.
3. Milliary TB: Haematogenous dissemination → multiple millet-seed granulomas in lungs, liver, spleen, meninges.

Ziehl-Neelsen Stain and Laboratory Diagnosis of Tuberculosis
Laboratory diagnosis of TB:
| Step | Method | Details |
|---|---|---|
| Specimen | Early morning sputum (3 samples on 2 consecutive days) | ≥5 mL; mucoid/purulent portion |
| Smear | ZN stain (Ziehl-Neelsen) | AFB appear red/pink on blue background; grading: 1+ to 3+ per RNTCP |
| Fluorescence | Auramine-rhodamine stain | More sensitive; AFB appear yellow-green on dark background; used in high-volume labs |
| Culture | Lowenstein-Jensen (LJ) medium | Growth in 3–8 weeks; rough, buff, raised, cauliflower-like colonies; reference standard |
| Rapid culture | MGIT (Mycobacteria Growth Indicator Tube) | Liquid medium; detects growth in 10–14 days via fluorescence |
| Molecular | CBNAAT/GeneXpert MTB/RIF | Detects MTB DNA and rifampicin resistance in <2 hours; WHO endorsed, free under NI-KSHAY |
| Sensitivity | DST (Drug Susceptibility Testing) | First-line: INH, RIF, PZA, EMB, SM; performed on culture isolate or directly by molecular methods |
Treatment: DOTS (Directly Observed Treatment, Short-course) under NI-KSHAY (formerly RNTCP): 2HRZE/4HR (new sputum-positive). Nikshay Poshan Yojana provides nutritional support.
Drug resistance:
- MDR-TB: Resistance to at least isoniazid + rifampicin
- XDR-TB: MDR + resistance to any fluoroquinolone + at least one injectable second-line drug
Prevention: BCG vaccine at birth (UIP); protects against miliary TB and TB meningitis in children; variable efficacy against pulmonary TB in adults.
SELF-CHECK
A sputum ZN smear report reads '1+ AFB' in a patient with 3-week cough and weight loss. The next step under NI-KSHAY guidelines is:
A. Start empirical antibiotics and repeat sputum at 1 month
B. Request GeneXpert MTB/RIF test
C. Perform Mantoux test and wait for result
D. Directly start Category I DOTS
Reveal Answer
Answer: B. Request GeneXpert MTB/RIF test
Under current NI-KSHAY (RNTCP 2.0) guidelines, any AFB-positive smear should be followed by GeneXpert MTB/RIF to confirm MTB and simultaneously detect rifampicin resistance. GeneXpert results guide treatment category (sensitive vs drug-resistant). Starting DOTS without GeneXpert risks missing MDR-TB.