Page 5 of 13
MI7.{2-3,5} | Lower Respiratory Tract Infections — SDL Guide (Part 2)
Viral and Fungal LRTIs
Viral and Fungal Lower Respiratory Tract Infections
Viral LRTIs:
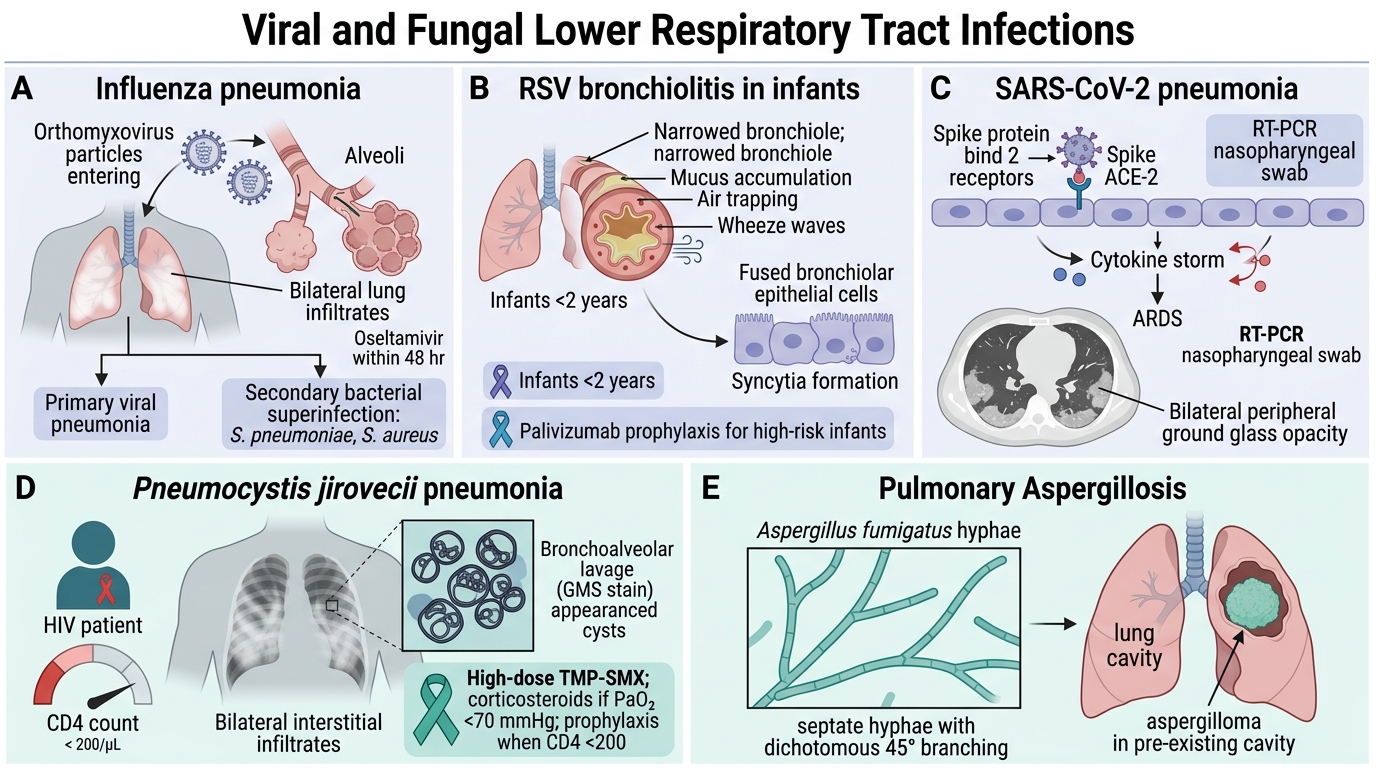
Influenza: Orthomyxovirus can cause severe pneumonia (primary viral pneumonia) or secondary bacterial superinfection (S. pneumoniae, S. aureus). ICU-requiring pneumonia with bilateral infiltrates ('white-out') — high mortality. Oseltamivir within 48 hr of onset.
RSV (Respiratory Syncytial Virus): Leading cause of bronchiolitis in infants <2 years. Syncytia formation in bronchiolar epithelium → air trapping → wheeze. Palivizumab prophylaxis for high-risk infants.
SARS-CoV-2 (COVID-19): Binds ACE-2 receptor via spike protein. Cytokine storm → ARDS; bilateral ground glass opacities on CT. RT-PCR of nasopharyngeal swab is gold standard.
Hantavirus (India — rare): Rodent-associated; Hantavirus Pulmonary Syndrome (HPS) — acute respiratory failure.
Fungal LRTIs:
Pneumocystis jirovecii Pneumonia (PCP):
- Previously called P. carinii; a fungus (despite being treated with cotrimoxazole)
- Cannot be cultured; diagnosis by GMS (Gomori Methenamine Silver) stain or immunofluorescence on BAL — cysts (trophic forms cluster as 'helmet-shaped' cysts)
- Classic: HIV patient with CD4 <200/µL; bilateral interstitial infiltrates; PaO₂ <70 mmHg
- Treatment: High-dose co-trimoxazole (TMP-SMX); add corticosteroids if PaO₂ <70
- Primary prophylaxis with TMP-SMX when CD4 <200 (standard of care under NACO ARTG)
Pulmonary Aspergillosis:
- Aspergillus fumigatus — septate hyphae, dichotomous branching at 45°
- Forms: (1) Aspergilloma — fungus ball in pre-existing cavity (e.g., TB cavity); (2) Allergic bronchopulmonary aspergillosis (ABPA) — asthma + central bronchiectasis; (3) Invasive aspergillosis — immunocompromised (neutropenia, transplant)
- Diagnosis: CT chest (halo sign in invasive), serum galactomannan ELISA (invasive), BAL culture, skin prick test (ABPA)
Cryptococcal pneumonia: Cryptococcus neoformans; thick capsule (India ink stain); primary infection via pigeon droppings; latent → reactivation in HIV (CD4 <100) → meningitis or pneumonia
Histoplasmosis (Histoplasma capsulatum): Dimorphic; not endemic in India but seen in travellers; small yeast inside macrophages on histology.
Parasitic LRTIs
Parasitic Lower Respiratory Tract Infections
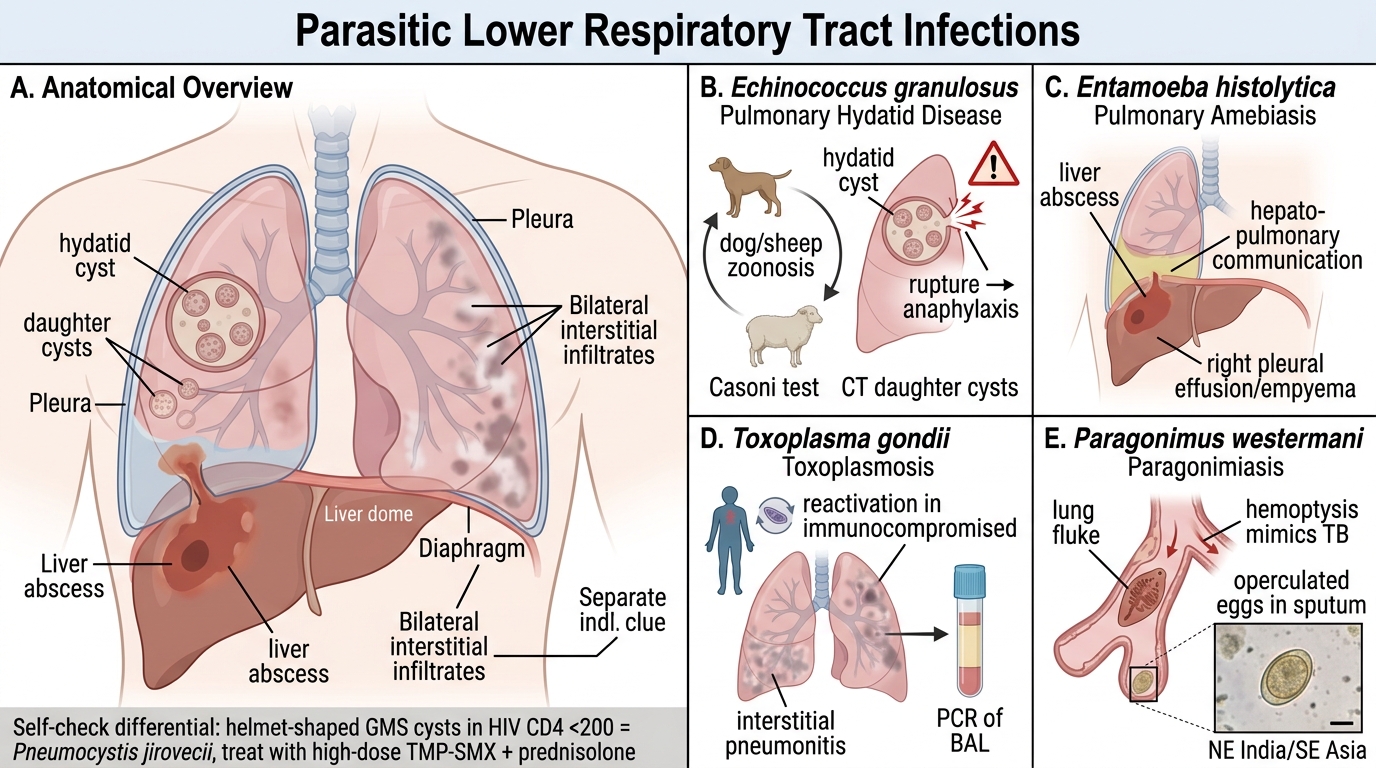
Pulmonary Hydatid Disease (Echinococcus granulosus):
- Cystic lesion (hydatid cyst) in lung; rupture → anaphylaxis; Casoni test (intradermal); CT shows daughter cysts
- Zoonosis from dogs/sheep; endemic in shepherding communities in India (Rajasthan, AP)
Pulmonary Ameobiasis (Entamoeba histolytica):
- Rare; right-sided pleural effusion/empyema due to hepato-pulmonary communication
Toxoplasmosis (Toxoplasma gondii):
- Reactivation in immunocompromised → interstitial pneumonitis; diagnosed by PCR of BAL
Paragonimiasis (Paragonimus westermani):
- Lung fluke; haemoptysis mimicking TB; eggs in sputum (operculated); endemic in NE India, SE Asia
SELF-CHECK
A 28-year-old HIV-positive patient on ART presents with 2-week progressive dyspnoea, dry cough and bilateral interstitial infiltrates. CD4 count is 120 cells/µL. BAL GMS stain shows helmet-shaped cysts. The MOST appropriate treatment is:
A. Liposomal amphotericin B
B. High-dose co-trimoxazole (TMP-SMX) + prednisolone
C. Oseltamivir
D. Isoniazid + rifampicin + pyrazinamide + ethambutol
Reveal Answer
Answer: B. High-dose co-trimoxazole (TMP-SMX) + prednisolone
GMS stain showing helmet-shaped cysts in BAL of an HIV patient with CD4 <200 is diagnostic of Pneumocystis jirovecii Pneumonia (PCP). First-line treatment is high-dose TMP-SMX. Corticosteroids (prednisolone) are added if PaO₂ <70 mmHg to reduce inflammation-mediated respiratory failure. Amphotericin B is for invasive fungal infections like Cryptococcus or Aspergillus, not PCP.
Sputum Processing and Microscopy (MI7.5 practical focus)
Sputum Processing and Microscopy for LRTI
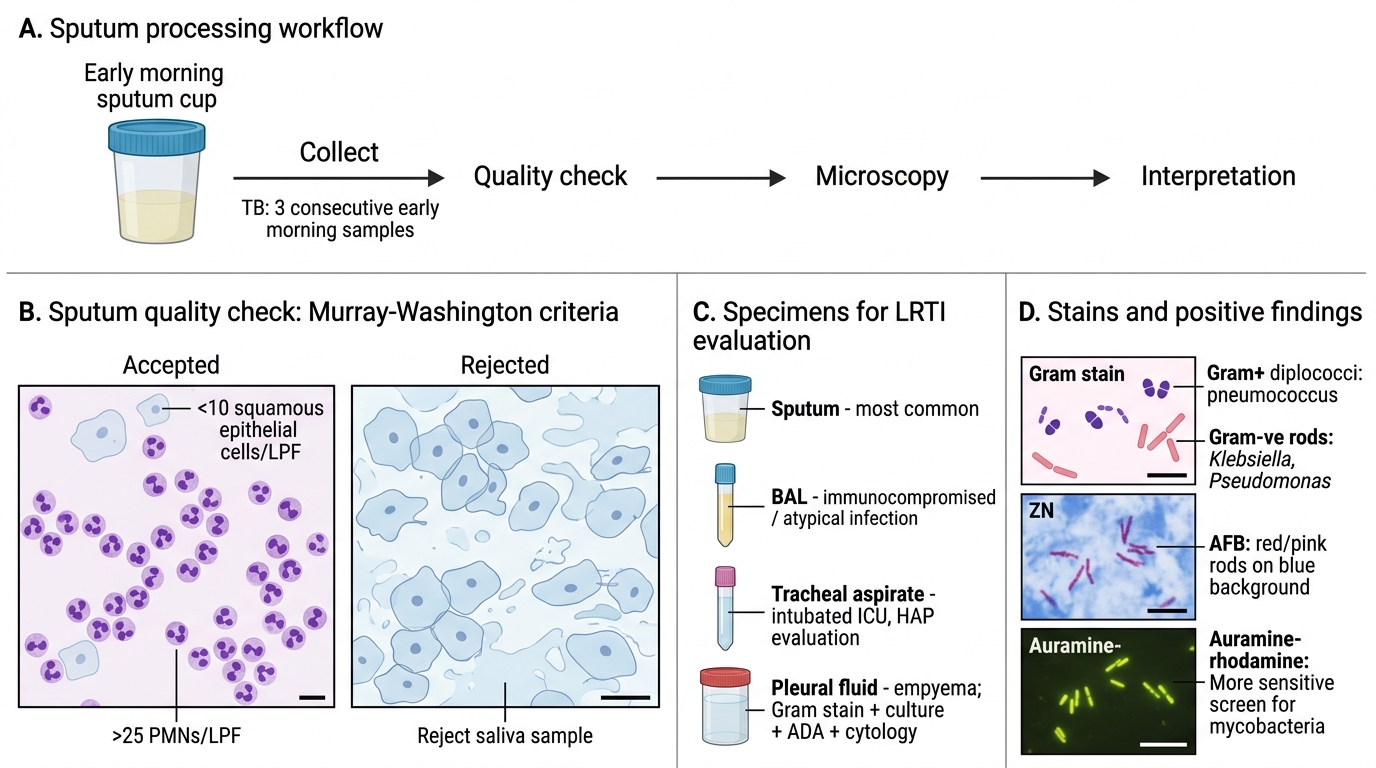
Sputum quality check: A good sputum sample has <10 squamous epithelial cells and >25 PMNs per low-power field (Murray-Washington criteria). Saliva samples are rejected.
Specimen types for LRTI:
- Sputum — most common; early morning; 3 consecutive samples for TB
- BAL (Bronchoalveolar Lavage) — immunocompromised patients, atypical infections
- Tracheal aspirate — intubated ICU patients (HAP evaluation)
- Pleural fluid — empyema; send for Gram stain + culture + ADA + cytology
Stains and interpretation:
| Stain | Organism Targeted | Positive Finding |
|---|---|---|
| Gram stain | Bacteria | Gram+ve diplococci (pneumococcus); Gram-ve rods (Klebsiella, Pseudomonas) |
| ZN (Acid-fast) stain | Mycobacteria | Red/pink rods on blue background (AFB) |
| Auramine-rhodamine | Mycobacteria | Fluorescent yellow-green rods (more sensitive than ZN) |
| GMS (Gomori Methenamine Silver) | Fungi (Aspergillus, PCP) | Black fungal cell walls; PCP cysts |
| India ink | Cryptococcus | Clear halo (capsule) around dark organism |
| KOH + Calcofluor white | All fungi | Fluorescent fungal cell wall |
Correlating Gram stain with clinical scenario:
- Gram+ve lancet-shaped diplococci + lobar consolidation + rusty sputum → S. pneumoniae
- Gram-ve thick capsulated rods + upper lobe + currant jelly sputum → K. pneumoniae
- No organisms + interstitial pattern + atypical features → Mycoplasma / viral / PCP
- AFB on ZN + cavitary upper lobe → MTB (confirm with GeneXpert)