Page 1 of 13
MI7.{1,4} | Upper Respiratory Tract Infections — SDL Guide
Learning Objectives
- Explain the etiopathogenesis of common bacterial, viral, fungal and parasitic upper respiratory tract infections (URTIs)
- Describe the laboratory diagnosis of URTIs including specimen collection, direct microscopy, culture and serology
- Describe preventive strategies for common URTIs
- Identify common etiologic agents of URTIs from Gram stain and Albert stain preparations of throat swabs and correlate with clinical findings
INSTRUCTIONS
Upper respiratory tract infections are among the commonest reasons for antibiotic misuse in India. Understanding the microbiology behind sore throat, croup, epiglottitis and sinusitis will help you choose the right investigation and avoid unnecessary prescriptions.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 24–26 (Streptococci, Corynebacterium, Respiratory Viruses) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 7-year-old boy is brought to a rural health centre in Tamil Nadu with fever, severe sore throat and a greyish-white membrane on his tonsils that bleeds when touched. His mother says two children in the same school died of a similar illness last month. What is the most likely diagnosis, and which stain will you request to confirm it before starting antitoxin?
WHY THIS MATTERS
URTIs account for over 40% of all outpatient visits in India and are the leading cause of antibiotic misuse. Streptococcal pharyngitis can progress to rheumatic heart disease — still a major cause of cardiac morbidity in young Indians. Diphtheria, though vaccine-preventable, continues to cause outbreaks in under-immunised communities. As a clinician you will diagnose, manage and prevent these conditions daily.
RECALL
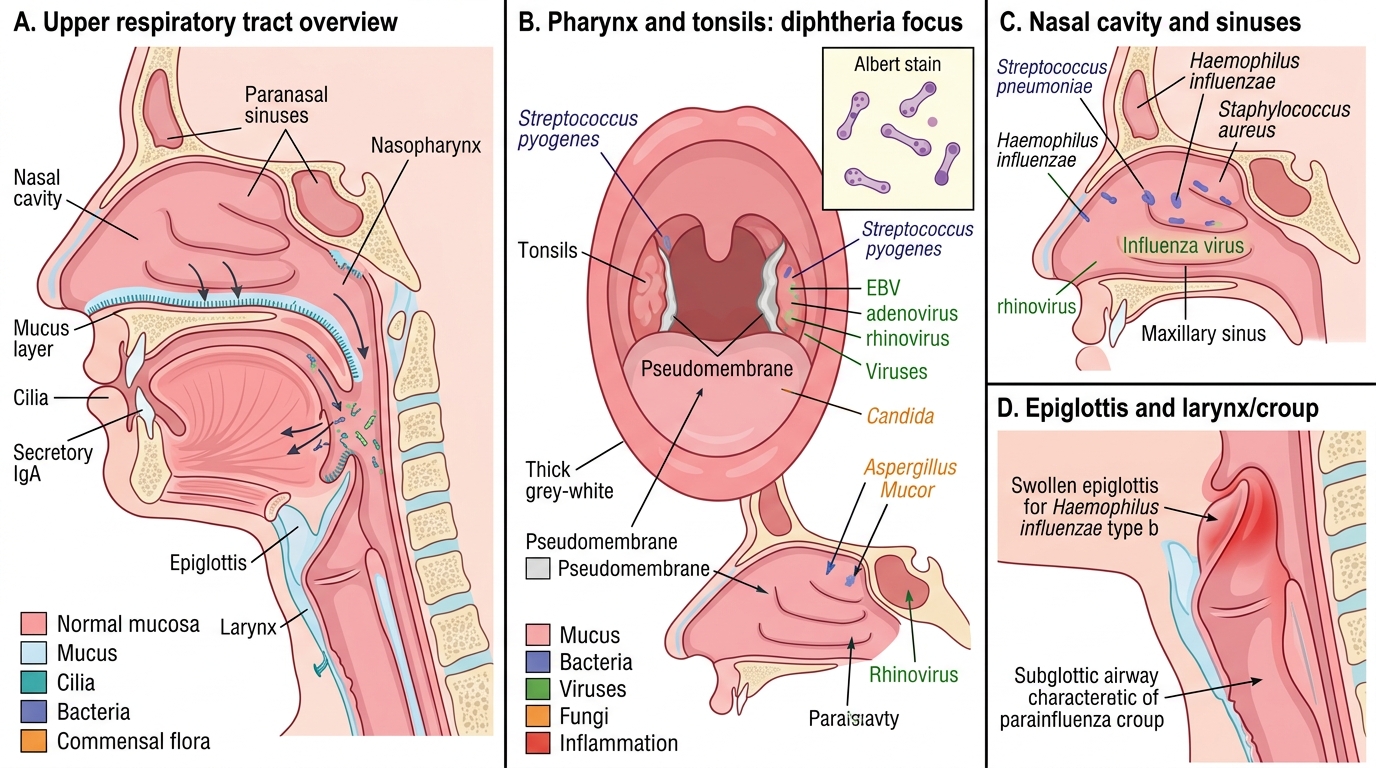
Before proceeding, recall: (1) The anatomical boundaries of the upper respiratory tract (nasal cavity to larynx). (2) Components of the innate mucosal immune defence — mucus, cilia, secretory IgA, lysozyme. (3) The principle behind Gram staining (crystal violet retained by peptidoglycan). (4) Albert stain: used to visualise metachromatic granules in Corynebacterium.
Overview of URTI Pathogens
Overview of Upper Respiratory Tract Pathogens
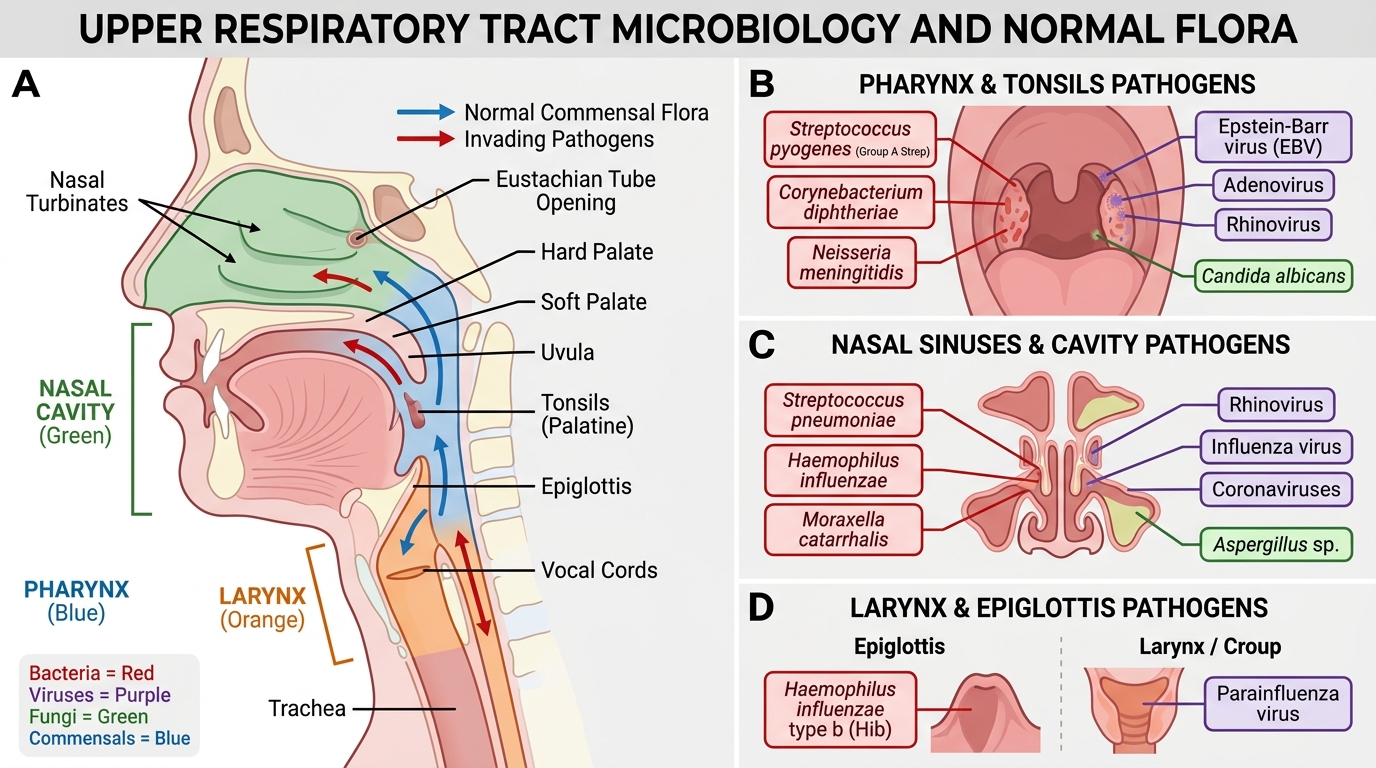
The upper respiratory tract is colonised by commensal flora (viridans streptococci, Neisseria spp., Haemophilus spp.) that compete with pathogens. Infection occurs when host defences are breached.
Anatomical site → key pathogens:
| Site | Bacterial | Viral | Fungal/Parasitic |
|---|---|---|---|
| Pharynx/Tonsils | Streptococcus pyogenes (GAS), Corynebacterium diphtheriae | Rhinovirus, EBV, Adenovirus | Candida (immunocompromised) |
| Nasal sinuses | S. pneumoniae, H. influenzae, S. aureus | Rhinovirus, Influenza | Aspergillus, Mucor |
| Epiglottis | H. influenzae type b (Hib) | — | — |
| Larynx/Croup | — | Parainfluenza virus (commonest) | — |
| Middle ear | S. pneumoniae, H. influenzae | RSV | — |
Viruses cause 80–90% of all URTIs. Rhinovirus (>100 serotypes) is the single most common cause of the common cold.
Streptococcal Pharyngitis (Group A Streptococcus)
Group A Streptococcal Pharyngitis: Pathogenesis and Diagnosis
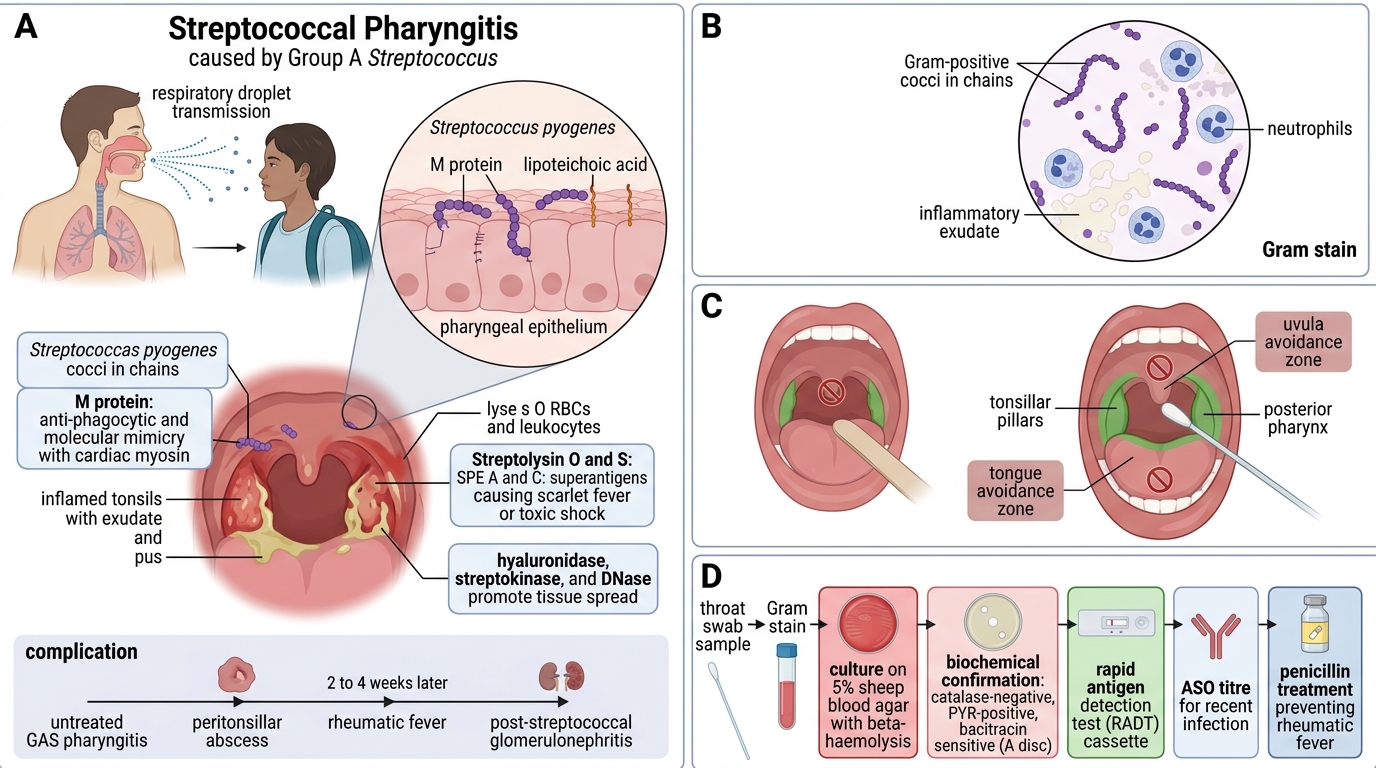
Organism: Streptococcus pyogenes (Group A β-haemolytic streptococcus, GAS)
Virulence factors:
- M protein — anti-phagocytic; molecular mimicry with cardiac myosin (→ rheumatic fever)
- Streptolysin O & S — lyse RBCs and leukocytes
- Streptococcal pyrogenic exotoxins (SPE A, C) — superantigens (→ scarlet fever, streptococcal toxic shock)
- Hyaluronidase, streptokinase, DNase — spread through tissues
Etiopathogenesis: Transmission by respiratory droplets. Adhesion via M protein and lipoteichoic acid to pharyngeal epithelium. Tonsillo-pharyngeal inflammation with pus. If untreated: peritonsillar abscess, rheumatic fever (2–4 weeks later), post-streptococcal glomerulonephritis.

GAS Pharyngitis: Throat Swab Gram Stain and Diagnosis
Laboratory diagnosis:
1. Throat swab — collected from tonsillar pillars avoiding tongue/uvula
2. Gram stain — Gram-positive cocci in chains (not specific but guides culture)
3. Culture on 5% sheep blood agar — β-haemolysis, catalase-negative, PYR-positive, bacitracin sensitive (A disc)
4. Rapid Strep Test (RADT) — immunochromatographic, 95% specificity; negative RADT should be confirmed by culture
5. ASO titre — retrospective diagnosis of GAS infection (>200 IU/mL significant); used for rheumatic fever workup
Prevention: Prompt antibiotic treatment (penicillin × 10 days) prevents rheumatic fever. Benzathine penicillin monthly prophylaxis for established rheumatic heart disease.
CLINICAL PEARL
Centor Score (modified McIsaac): Tonsillar exudate + Tender anterior cervical nodes + Fever >38°C + No cough = 4 points → 50% probability of GAS. Score ≤1: antibiotics not indicated; test and treat only if score ≥2. Overuse of antibiotics for viral pharyngitis is a major driver of antimicrobial resistance in India.
Diphtheria
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Upper Respiratory Tract Infections: Diphtheria in Context
Organism: Corynebacterium diphtheriae — Gram-positive, non-sporing, non-motile, pleomorphic rod with metachromatic (volutin) granules. Arranged in Chinese letter / cuneiform pattern on smear. Toxigenic strains carry the tox gene (encoded by bacteriophage β).
Diphtheria exotoxin (A-B toxin):
- Fragment B — binds to host cell receptor, facilitates entry
- Fragment A — ADP-ribosylates EF-2 (elongation factor 2) → irreversible inhibition of protein synthesis → cell death
- Affects heart (myocarditis), nerves (demyelination — palatal palsy, ocular palsy, peripheral neuropathy), adrenals
Etiopathogenesis: Droplet transmission → colonises upper respiratory mucosa → elaborates toxin locally → systemic toxin dissemination. Pseudomembrane (grayish-white, bleeds on removal, tightly adherent) forms over tonsils/pharynx/larynx; laryngeal diphtheria causes bull-neck, stridor, risk of airway obstruction.

Corynebacterium diphtheriae: Albert Stain and Laboratory Diagnosis
Laboratory diagnosis:
1. Albert stain — demonstrates metachromatic granules (diagnostic clue)
2. Gram stain — Gram-positive pleomorphic rods in Chinese letter arrangement
3. Culture on Loeffler's serum slope — rapid growth (18 hr), enhances granule formation; tellurite medium (Hoyle's/CTBA) — selective, colonies appear grey-black
4. Toxin detection — Elek's gel precipitation test (in vitro gold standard): filter paper strip soaked in diphtheria antitoxin placed on agar; organism streaked perpendicular; precipitation line at 45° = toxigenic
5. Schick test (in vivo, now historical) — assesses individual immunity to toxin
Treatment: Diphtheria antitoxin (DAT) urgently + penicillin/erythromycin (to eliminate organism)
Prevention: DPT/DTP vaccine in Universal Immunisation Programme (UIP). Booster at 5 years (DPT) and 10 years (Td). Investigate contacts; carriers treated with antibiotics.
SELF-CHECK
A throat swab Albert stain shows yellow-green bacilli with blue-black polar granules arranged in a 'V' or 'L' shape. The most appropriate confirmatory test for toxigenicity is:
A. Widal test
B. Elek's gel precipitation test
C. PYR test
D. Optochin sensitivity test
Reveal Answer
Answer: B. Elek's gel precipitation test
Elek's gel precipitation test detects diphtheria toxin in vitro by immunodiffusion. A precipitation arc between the organism streak and antitoxin-impregnated strip confirms toxin production. PYR test identifies GAS; Optochin identifies S. pneumoniae; Widal is for typhoid.