Page 2 of 13
MI7.{1,4} | Upper Respiratory Tract Infections — SDL Guide (Part 2)
Viral URTIs
Viral Upper Respiratory Tract Infections
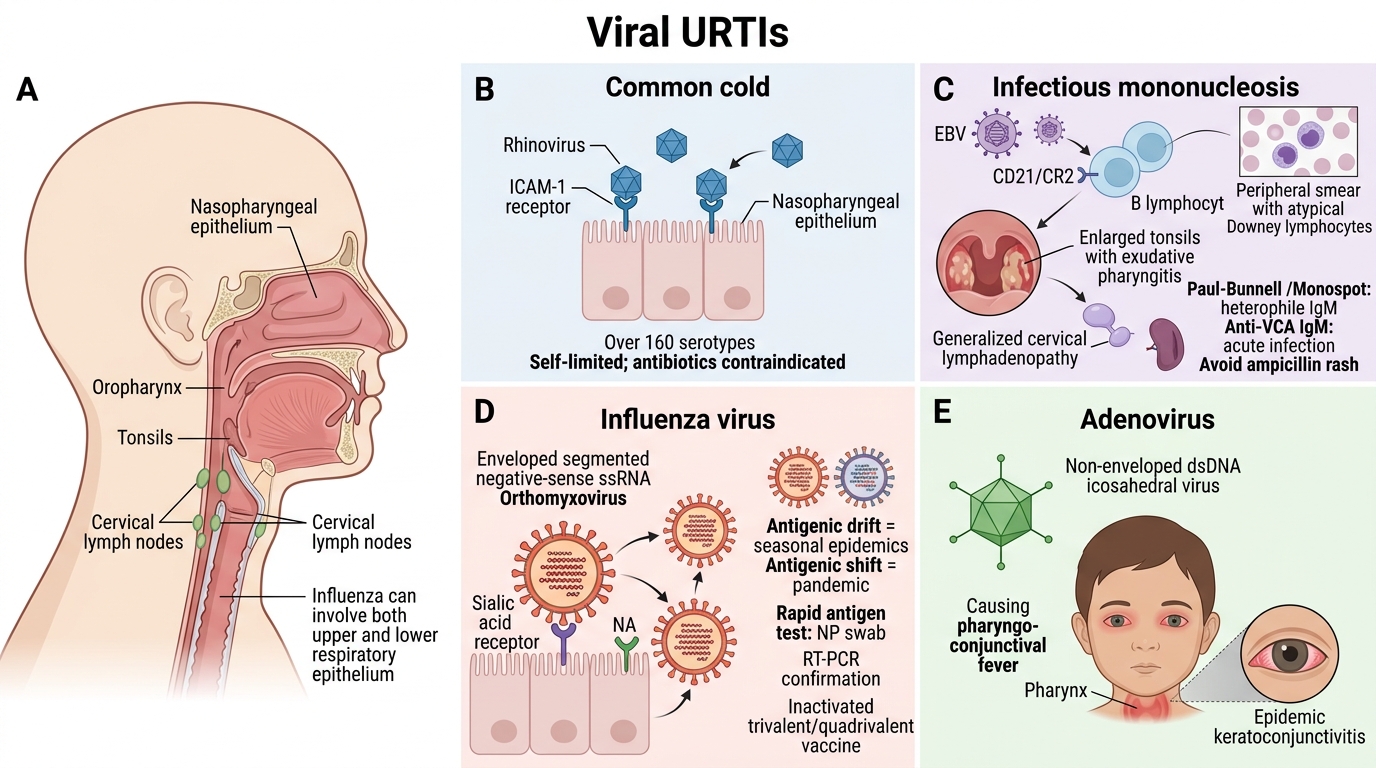
Common cold (Rhinovirus):
- Over 160 serotypes → no vaccine possible
- Binds ICAM-1 receptor on nasopharyngeal epithelium
- Self-limited; antibiotics contraindicated
Infectious Mononucleosis (EBV):
- Epstein–Barr virus (HHV-4), dsDNA, Herpesviridae
- Triad: fever, severe pharyngitis with exudate, generalised lymphadenopathy + splenomegaly
- EBV infects B lymphocytes via CD21 (CR2) receptor
- Atypical lymphocytes (Downey cells) on peripheral blood smear
- Paul–Bunnell / Monospot test — detects heterophile antibodies (IgM agglutinating sheep/horse RBCs)
- Specific: Anti-VCA IgM (acute), Anti-EA, Anti-EBNA
- Avoid ampicillin (causes maculopapular rash in EBV mononucleosis)
Influenza (seasonal):
- Orthomyxovirus; segmented negative-sense ssRNA
- Infects upper AND lower respiratory epithelium
- Haemagglutinin (HA) binds sialic acid receptors; Neuraminidase (NA) enables virion release
- Antigenic drift (mutations) → seasonal epidemics; Antigenic shift (reassortment) → pandemic
- Rapid antigen test (nasopharyngeal swab); RT-PCR for confirmation
- Vaccines: trivalent/quadrivalent inactivated (recommended for healthcare workers in India)
Adenovirus:
- Non-enveloped dsDNA; pharyngo-conjunctival fever in children; epidemic keratoconjunctivitis
Fungal and Parasitic URTIs
Fungal and Parasitic Upper Respiratory Tract Infections
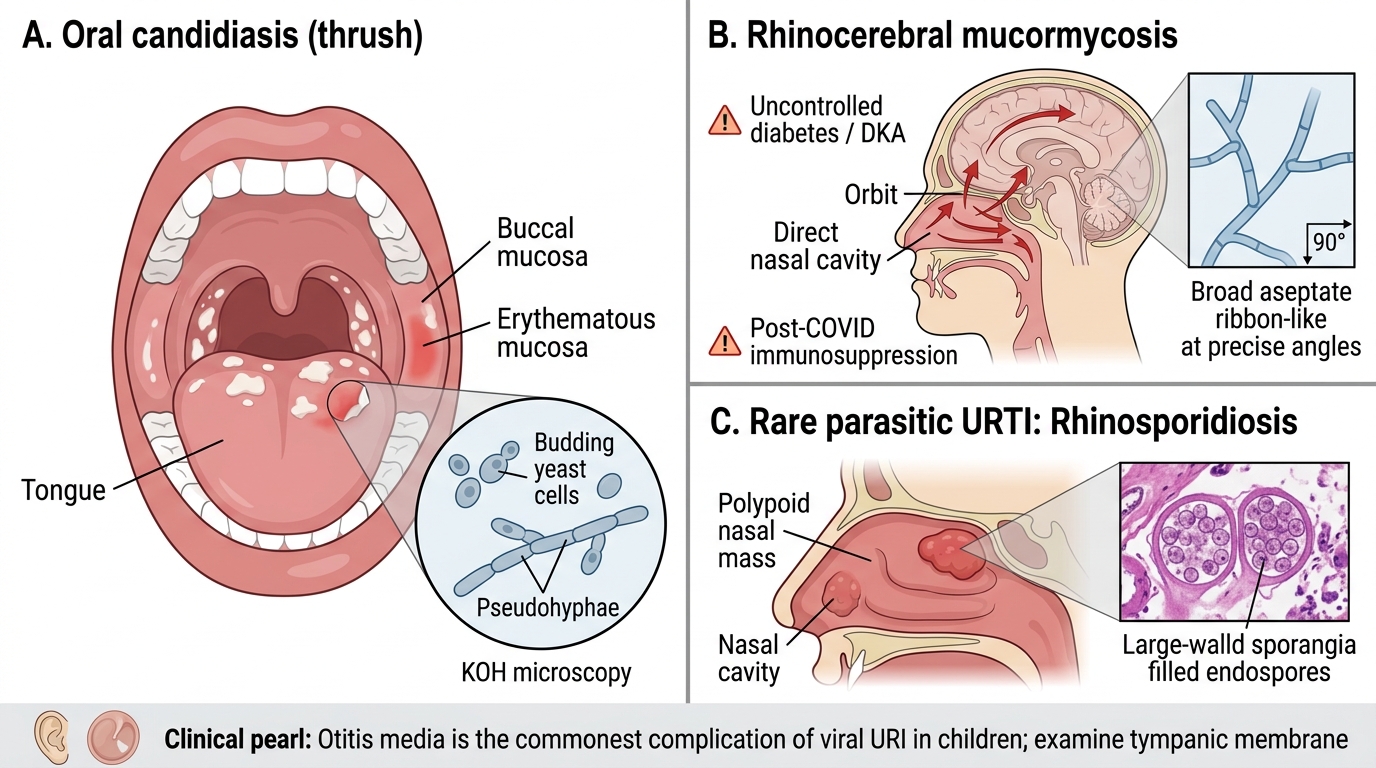
Oral candidiasis (thrush):
- Candida albicans — dimorphic fungus, forms pseudohyphae and chlamydospores
- White removable plaques on buccal mucosa/tongue/pharynx
- Risk factors: broad-spectrum antibiotics, corticosteroid inhalers, diabetes, HIV/immunosuppression
- KOH mount: pseudohyphae + budding yeast cells
- Treatment: topical nystatin; fluconazole for oropharyngeal candidiasis in HIV
Rhinocerebral Mucormycosis:
- Rhizopus, Mucor, Cunninghamella — angioinvasive mould; wide aseptate hyphae at right angles
- Sinuses → orbit → brain; very high mortality
- Risk factors: uncontrolled diabetes (especially DKA), post-COVID immunosuppression (Black Fungus epidemic in India, 2021)
- LPCB/H&E: broad, aseptate, ribbon-like hyphae branching at 90°
- Treatment: liposomal amphotericin B + surgical debridement
Parasitic URTIs are rare in immunocompetent hosts. Rhinosporidiosis (nasal polyps caused by Rhinosporidium seeberi — a protist) is endemic in south India and Sri Lanka; diagnosed by histology showing large sporangia.
CLINICAL PEARL
Otitis media is the commonest complication of viral URI in children. S. pneumoniae (30–40%), H. influenzae non-typeable (25%), and M. catarrhalis (15%) are the major bacterial causes. PCV13 vaccine (part of UIP from 2017 in select states) significantly reduces pneumococcal otitis media. Always examine the tympanic membrane in a febrile child with URI.
Specimen Collection and Processing for URTIs (MI7.4 practical focus)
Throat Swab Collection and Processing for URTIs
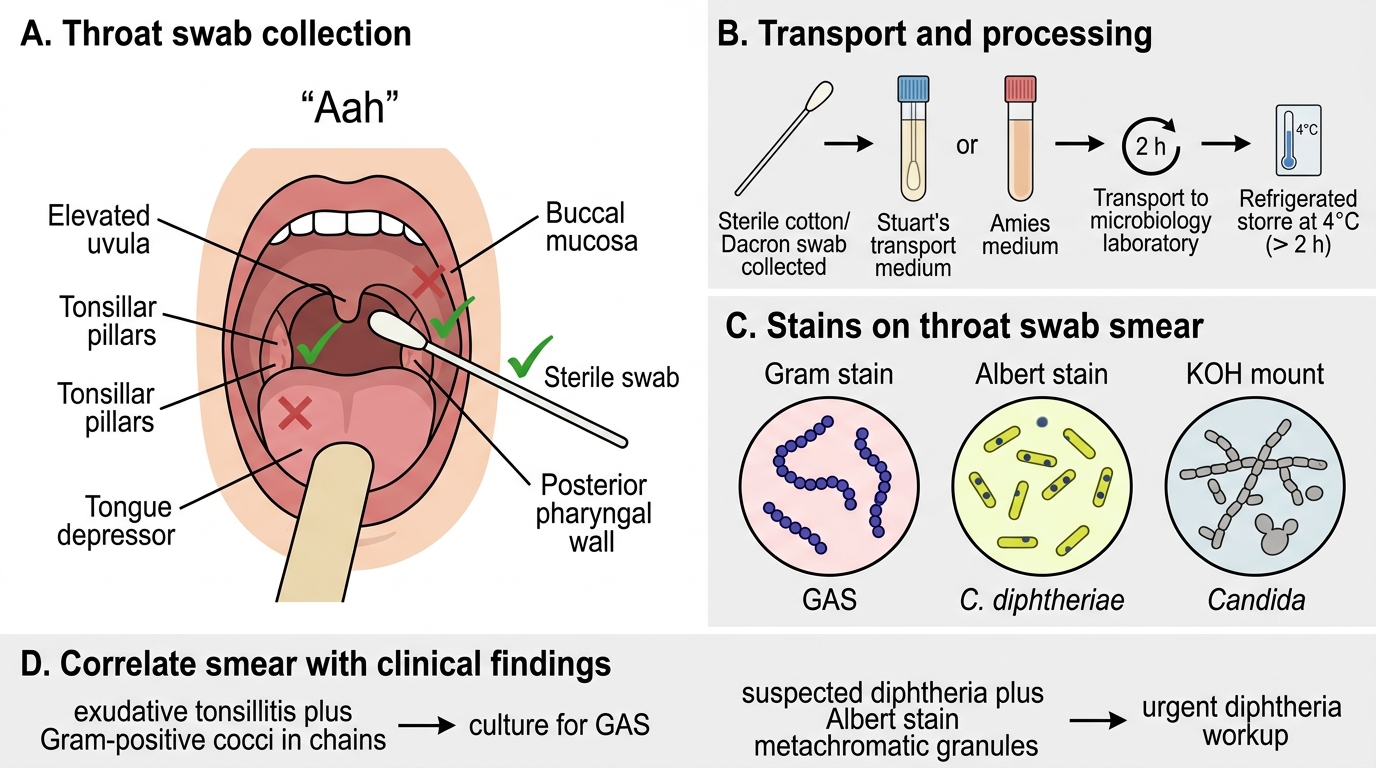
Throat swab technique:
1. Ask patient to say 'Aah' — uvula rises, exposing tonsillar pillars
2. Use a sterile cotton/Dacron swab; avoid tongue and buccal mucosa
3. Swab both tonsillar pillars and posterior pharynx
4. Transport in Stuart's transport medium within 2 hours (or Amies medium)
5. Refrigerate at 4°C if delay >2 hours
Stains performed on throat swab smear:
| Stain | Target | Appearance | Purpose |
|---|---|---|---|
| Gram stain | GAS, other bacteria | Gram+ve cocci in chains (GAS) | Screening |
| Albert stain | C. diphtheriae | Blue-black granules in yellowish-green bacilli | Diphtheria |
| KOH mount | Candida | Pseudohyphae + budding yeast | Oral candidiasis |
Correlating smear with clinical findings:
- Gram stain: Gram+ve cocci in chains + exudative tonsillitis → culture for GAS
- Albert stain: metachromatic granules + pseudomembrane → initiate DAT, confirm with Elek's
- No organisms on Gram stain + prominent lymphadenopathy → consider EBV (Paul-Bunnell test)
SELF-CHECK
A 30-year-old healthcare worker develops fever, severe sore throat and petechiae on the palate. Peripheral blood smear shows atypical lymphocytes. The MOST appropriate next investigation is:
A. Throat culture on blood agar
B. Albert stain of throat swab
C. Paul-Bunnell / Monospot test
D. ASO titre
Reveal Answer
Answer: C. Paul-Bunnell / Monospot test
The clinical picture — exudative tonsillitis, palatal petechiae, atypical lymphocytes (Downey cells) — is classic for Infectious Mononucleosis caused by EBV. The Paul-Bunnell (Monospot) test detects heterophile antibodies and is the rapid bedside test of choice. ASO titre detects past GAS infection; Albert stain is for diphtheria; throat culture would be done but is not the most specific next step here.