Page 2 of 14
OG1.1-3 | Maternal, Perinatal, Stillbirth and Abortion Statistics — SDL Guide (Part 2)
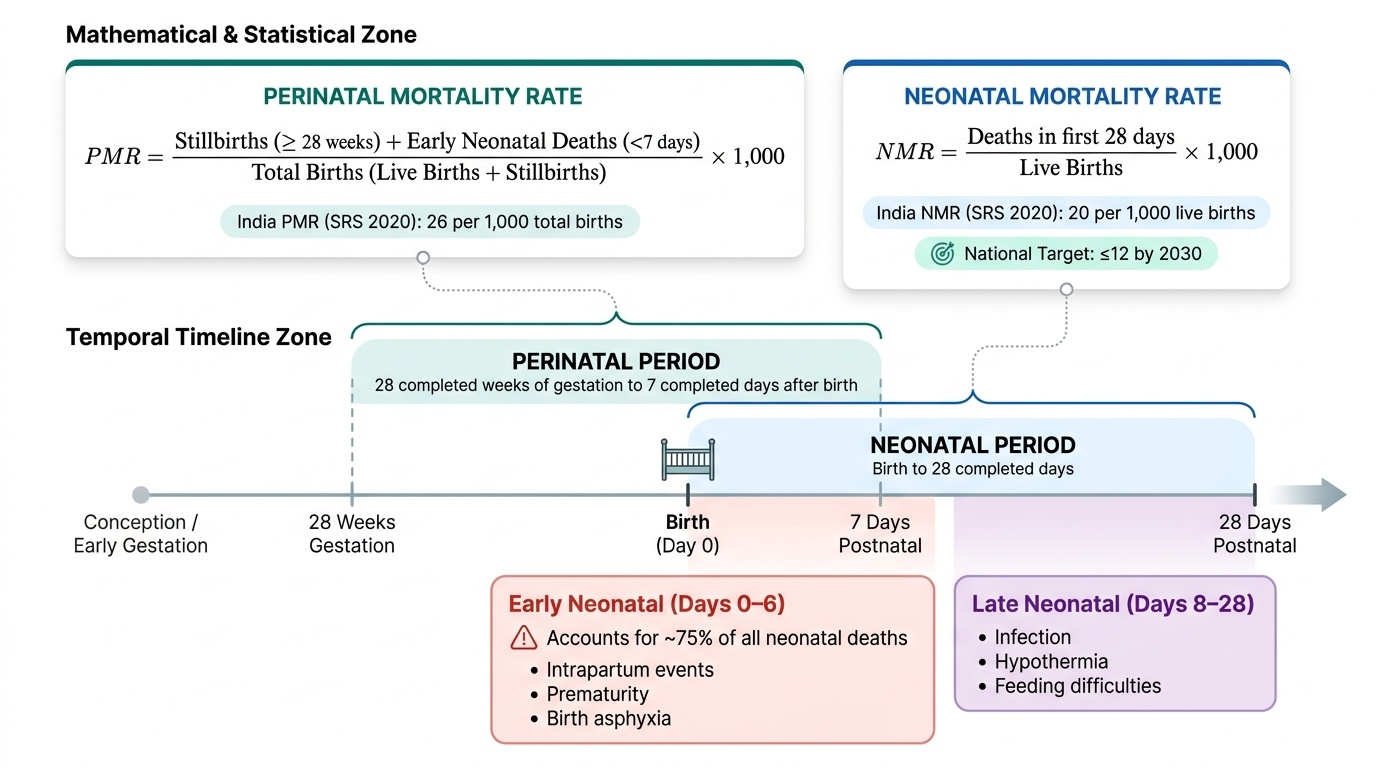
Perinatal and Neonatal Mortality: Definitions and Rates
The perinatal period bridges the end of pregnancy and the first week of postnatal life. It is defined as commencing at 28 completed weeks of gestation and ending at 7 completed days after birth. This period encompasses the highest-risk interval for both fetus and neonate — the majority of infant deaths occur during this window. Extending the lower gestational boundary to 28 weeks (rather than viability at 22–24 weeks used in some high-resource settings) reflects the practical threshold for fetal viability and systematic recording in most Indian health facilities.
The Perinatal Mortality Rate (PMR) = (Stillbirths at ≥28 weeks + Early neonatal deaths in the first 7 days) ÷ (Total births — live births + stillbirths) × 1,000. Critically, the denominator is total births (not live births), because stillbirths — which form part of the numerator — can only be counted if the denominator includes them. India's PMR by the SRS 2020 was approximately 26 per 1,000 total births.
Neonatal mortality describes deaths occurring from birth through 28 completed days of postnatal life. It is subdivided:
• Early neonatal death: death in the first 7 days of life (days 0–6). These account for about 75% of all neonatal deaths and are closely linked to intrapartum events, prematurity, and birth asphyxia.
• Late neonatal death: death from day 8 through day 28. These are more often due to infection, hypothermia, and feeding difficulties.
The Neonatal Mortality Rate (NMR) = (Deaths in the first 28 days) ÷ (Live births) × 1,000. India's NMR was approximately 20 per 1,000 live births (SRS 2020), with a target of ≤12 by 2030.
The Infant Mortality Rate (IMR) = (Deaths in the first year of life) ÷ (Live births) × 1,000. India's IMR was approximately 28 per 1,000 live births (SRS 2020). Neonatal deaths account for roughly 70% of infant deaths in India.
Provided image
Stillbirth: Definition, Causes and Measurement
A stillbirth is the birth of a baby who shows no signs of life at or after 28 completed weeks of gestation. The WHO further allows a weight criterion: ≥1,000 g, which corresponds approximately to 28 weeks. India follows the 28-week gestational threshold for routine registration and vital statistics. In clinical practice, two types of stillbirth are recognised based on the state of the fetus at delivery.
Macerated stillbirth occurs when the fetus has died in utero some time before delivery (typically more than 12–24 hours). The hallmarks are skin slippage (desquamation), discolouration (greenish/brownish), soft tissues collapsing (bag of bones), and overlapping skull bones (Spalding's sign on X-ray). Macerated stillbirths are associated with placental insufficiency, cord complications, severe IUGR, and post-term pregnancy. Fresh stillbirth (or intrapartum stillbirth) is one in which the fetus appears freshly dead at delivery without signs of maceration — suggesting death occurred close to delivery, often from an acute intrapartum event such as cord prolapse, abruptio placentae, or uterine rupture. Intrapartum stillbirths are particularly important for quality of care assessment because many are potentially preventable.
The Stillbirth Rate (SBR) = (Number of stillbirths at ≥28 weeks) ÷ (Total births) × 1,000. Like the PMR, the denominator is total births. India's SBR has declined considerably from over 30 per 1,000 total births in the 1990s to approximately 5–6 per 1,000 total births in recent national data, though facility and state variation is wide.
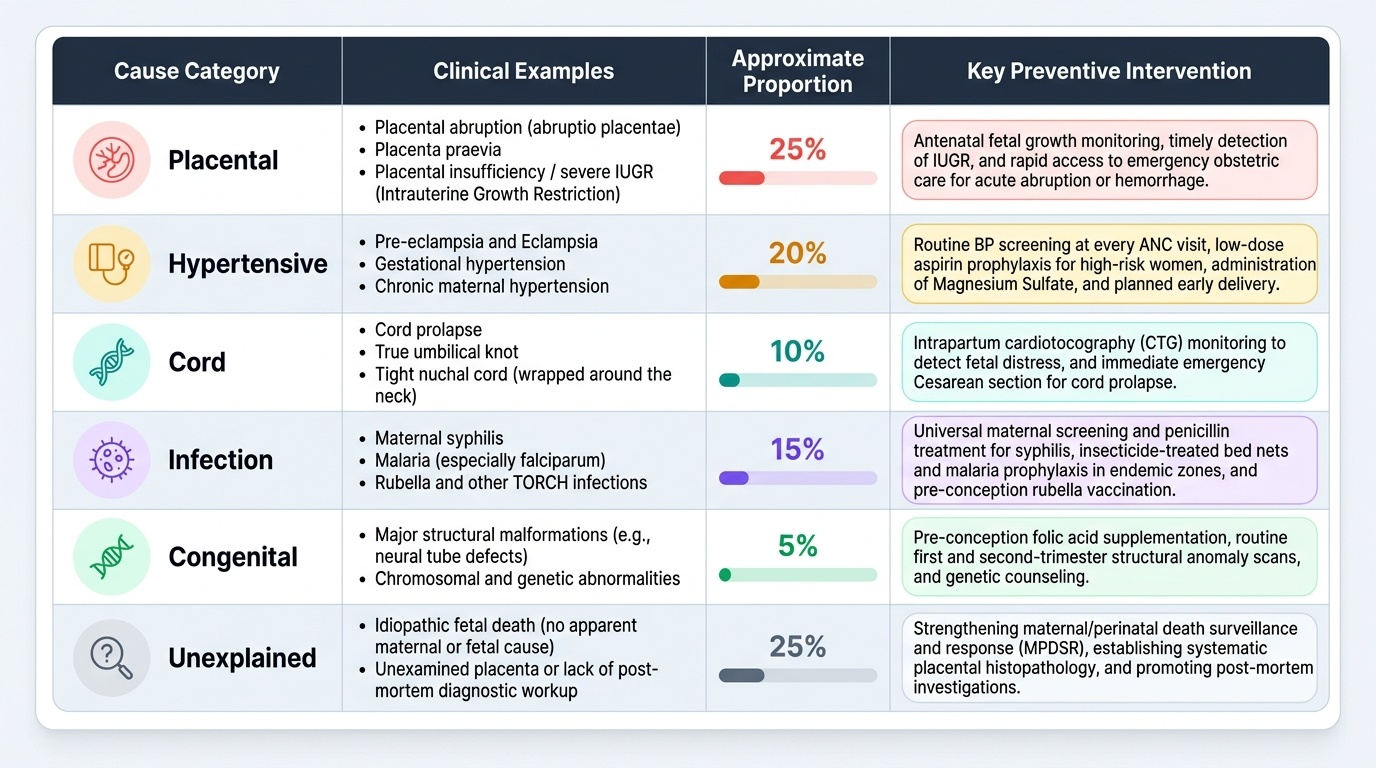
Major causes of stillbirth include: placental abruption, placenta praevia, cord accidents (prolapse, true knot, tight nuchal cord), severe intrauterine growth restriction, hypertensive disorders of pregnancy, congenital anomalies, maternal infections (syphilis, malaria, rubella), and prolonged/obstructed labour. In India, a significant proportion of stillbirths remain with no identified cause (unexplained stillbirth), reflecting gaps in systematic post-mortem and placental examination.
Provided image
Abortion: Definitions and Classification
In obstetrics, abortion is defined as the expulsion or extraction of a fetus or embryo weighing less than 500 grams or before 20 completed weeks of gestation — whichever comes first. This threshold is clinically important: at or beyond 20 weeks, loss of pregnancy is classified as a stillbirth (if the fetus shows no signs of life) or a preterm delivery (if it does), not an abortion. The obstetric definition is a clinical and statistical classification that determines how the case is recorded in vital statistics registers and audits. It is entirely distinct from the legal definition under the Medical Termination of Pregnancy (MTP) Act, which defines the gestational limits within which the voluntary termination of pregnancy may be lawfully performed. Students must keep these two frameworks clearly separate: the obstetric definition classifies any pregnancy loss before 20 weeks regardless of whether it was spontaneous or induced; the MTP Act governs only the legal conditions under which a practitioner may terminate a pregnancy. Conflating the two is a common examination and clinical error.
Abortion is classified along two axes — by causation and by clinical presentation.
By causation:
• Spontaneous abortion (miscarriage): pregnancy loss without medical or surgical intervention, due to chromosomal abnormalities (most common, ~50–60% of first-trimester losses), uterine anomalies, cervical incompetence, thrombophilia, or infection.
• Induced abortion: deliberate termination by medical (mifepristone–misoprostol) or surgical (manual vacuum aspiration, D&E) methods. Under the MTP Act (amended 2021), termination up to 20 weeks requires one registered medical practitioner's opinion; 20–24 weeks requires two practitioners and applies to specific categories (survivors of rape/incest, minors, foetal anomaly, change in marital status, physical or mental disability). Beyond 24 weeks, termination for substantial foetal abnormality requires a State Medical Board's approval.
• Septic abortion: any abortion (spontaneous or induced) complicated by infection, characterised by fever, offensive discharge, uterine tenderness, and leucocytosis. Septic abortion carries a high risk of pelvic sepsis, septicaemia, and maternal death if not managed promptly with antibiotics and uterine evacuation.
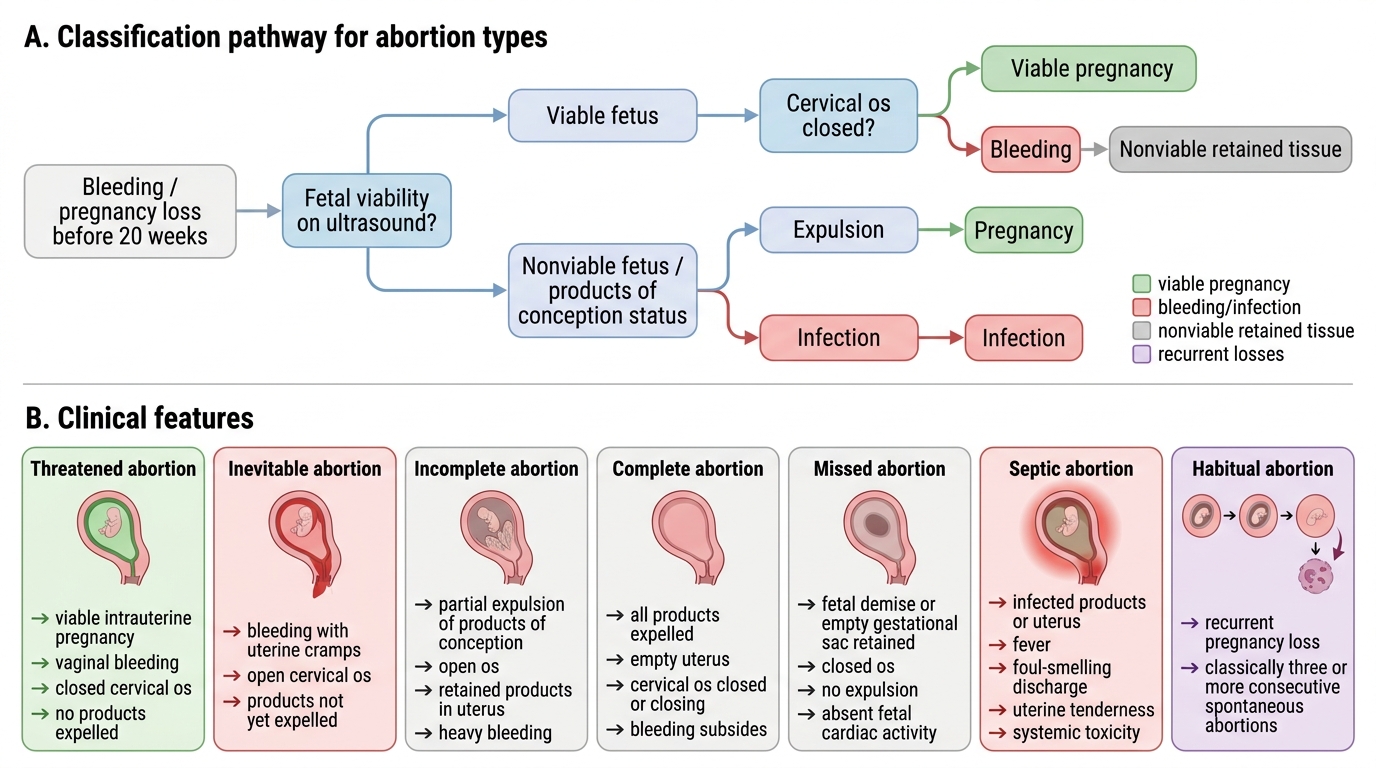
By clinical presentation (spontaneous abortion types):
• Threatened abortion: vaginal bleeding with cervical os closed; pregnancy may continue. Management is expectant.
• Inevitable abortion: bleeding with open os and/or ruptured membranes; pregnancy cannot continue.
• Incomplete abortion: partial expulsion of products of conception; os open, uterus larger than expected.
• Complete abortion: all products expelled; os closed, uterus small and firm.
• Missed abortion (silent/blighted ovum): fetal death or failed development with retained products; os closed, uterus smaller than dates; may present with brown discharge or incidentally on ultrasound.
• Habitual (recurrent) abortion: three or more consecutive spontaneous abortions — now defined by most authorities as two or more. Requires investigation for genetic, uterine, thrombophilic, endocrine, and immune causes.
Classification of Abortion Types
SELF-CHECK
A woman presents with vaginal bleeding at 10 weeks gestation. Ultrasound shows a viable fetus and closed cervical os. What is the correct obstetric classification?
A. Missed abortion
B. Inevitable abortion
C. Threatened abortion
D. Incomplete abortion
Reveal Answer
Answer: C. Threatened abortion
Threatened abortion is characterised by vaginal bleeding in the first 20 weeks with a closed cervical os and a viable intrauterine pregnancy. The pregnancy may still continue. Inevitable abortion has an open os; missed abortion has fetal death without expulsion; incomplete has partially expelled products.