Page 16 of 32
OG18.{2,4} | Neonatal Resuscitation — SDL Guide
Learning Objectives
- Describe the principles of fetal-to-neonatal transition and explain why timely resuscitation prevents hypoxic-ischaemic injury
- Outline the NRP/HBB algorithm and perform the initial steps of neonatal resuscitation in a simulated environment
- Demonstrate correct bag-mask ventilation (PPV) technique and identify when to escalate to chest compressions
- Apply the 3:1 compression-to-ventilation ratio correctly and distinguish it from the adult 30:2 ratio
- Describe the current NRP approach to meconium-stained amniotic fluid
- Interpret the Apgar score at 1 and 5 minutes and explain its clinical significance
INSTRUCTIONS
Neonatal asphyxia accounts for approximately 23% of global neonatal deaths, making resuscitation at birth one of the highest-impact clinical skills in obstetric practice. This module uses the blueprint-first, simulation-centred OG-skills arc to walk you through the NRP/HBB sequence — from the Golden Minute concept through PPV, compressions, and post-resuscitation assessment. You will practise the cognitive components here and consolidate them at the skill station.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch. 27 (textbook)
- Neonatal Resuscitation Programme (NRP) 8th Edition — AAP/AHA 2021 (textbook)
- Helping Babies Breathe, 2nd Edition — WHO/AAP 2016 (textbook)
- Williams Obstetrics, 25th ed., Ch. 32 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the resident on the labour ward at 02:00 h when a primigravida at 39 weeks delivers a limp, pale, non-crying baby after a prolonged second stage. The midwife calls out 'baby is not breathing!' The clock is ticking — you have 60 seconds before the risk of permanent brain injury rises sharply. What do you do first, and in what sequence?
WHY THIS MATTERS
Approximately 10% of newborns require some assistance to breathe at birth, and 1% need intensive resuscitative measures. In India, neonatal asphyxia contributes to nearly 0.3 million deaths annually and is a leading cause of neurodevelopmental disability in survivors. The difference between a normal outcome and hypoxic-ischaemic encephalopathy (HIE) often comes down to whether the provider at the bedside confidently executed the correct sequence within the Golden Minute. As a final-year student rotating through the labour ward, you are that provider. Mastering this skill is not elective — it is a core NMC competency (OG18.2 and OG18.4) and a professional obligation.
RECALL
Before we begin, activate your prior knowledge. Recall from your neonatal physiology module (OG17/OG18.1): What are the five Apgar parameters, and at what time points is the score recorded? What happens to the ductus arteriosus and foramen ovale at birth? What triggers the first breath — is it hypoxia, hypercapnia, tactile stimulation, or temperature change? Write your answers briefly in the reflection space — we will revisit them as we go.
When Every Second Counts: Why Neonatal Resuscitation Is a Core Skill
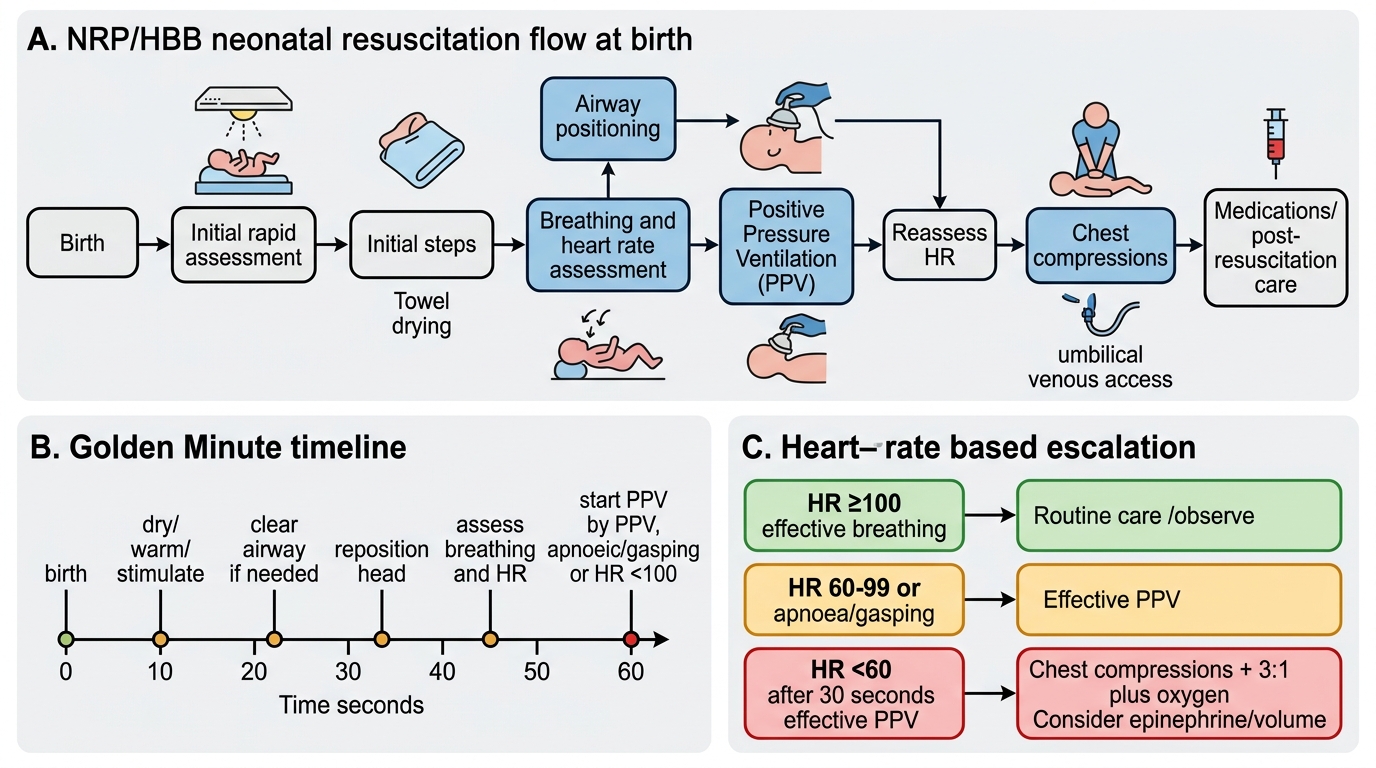
The Golden Minute is the central concept of the NRP (Neonatal Resuscitation Programme, published by the American Academy of Paediatrics) and of HBB (Helping Babies Breathe, the WHO-endorsed low-resource adaptation): complete all initial steps and make a clear breathing/heart-rate assessment within the first 60 seconds of birth. If the baby is not breathing or has a heart rate below 100 beats per minute at the end of this minute, positive-pressure ventilation (PPV) must begin immediately. This narrow window exists because the neonatal brain tolerates hypoxia very poorly — neuronal death begins within 4–6 minutes of complete oxygen deprivation, and the cortical neurones of a term infant are far more vulnerable than those of an adult, partly because their energy reserves (glycogen stores) are proportionally smaller.
The epidemiological burden justifies placing this skill at the top of the OG curriculum. Globally, about 2.5 million neonates die in the first month of life, and birth asphyxia (failure to initiate or sustain breathing at birth) accounts for roughly one quarter of these deaths. In India, a facility-based study published in the National Medical Journal of India found that the simple introduction of HBB training in secondary-level hospitals reduced early neonatal death from birth asphyxia by 46%. The implication is profound: a five-minute skill intervention, correctly performed by the person present at delivery, can prevent death or permanent disability.
Clinically, you should anticipate resuscitation before delivery rather than reacting to it. Antenatal risk factors that increase the probability of requiring resuscitation include: prematurity, meconium-stained amniotic fluid, prolonged rupture of membranes, multiple gestation, abnormal fetal lie, cord prolapse, antepartum haemorrhage, and maternal conditions such as pre-eclampsia, diabetes, or opioid administration. However, approximately 50% of neonates who require resuscitation have NO antenatal risk factors — which is why every delivery should be attended by at least one person trained in basic neonatal resuscitation, with equipment checked and ready.
NRP Neonatal Resuscitation Algorithm and Golden Minute
SELF-CHECK
Within the NRP/HBB framework, the 'Golden Minute' refers to:
A. The time allowed to administer epinephrine after cardiac arrest
B. The first 60 seconds after birth in which initial steps and breathing assessment must be completed
C. The window to clamp and cut the umbilical cord
D. The maximum duration of bag-mask ventilation before intubation is mandatory
Reveal Answer
Answer: B. The first 60 seconds after birth in which initial steps and breathing assessment must be completed
The Golden Minute is the first 60 seconds post-birth: complete warming, drying, stimulation, airway positioning, and then assess breathing and heart rate. If the baby is not breathing adequately or HR <100, PPV begins immediately. It does not refer to the timing of cord clamping, epinephrine, or intubation.
Fetal-to-Neonatal Transition: Anatomical and Physiological Principles
Understanding WHY resuscitation is needed requires appreciating the dramatic physiological shift the neonate must execute in the first minutes of extrauterine life. In the fetus, the lungs are liquid-filled and non-functional for gas exchange — oxygenation is entirely placental. Three key vascular shunts maintain fetal circulation: the ductus venosus (bypasses liver), the foramen ovale (right-to-left shunt across the atrial septum), and the ductus arteriosus (connects pulmonary artery to the descending aorta, bypassing the fluid-filled lungs). Fetal pulmonary vascular resistance (PVR) is very high precisely because the lungs are collapsed and hypoxic.
At birth, a cascade of events must occur within seconds. The cord is clamped, removing the low-resistance placenta from the circuit. The neonate takes its first breath — driven by cold tactile stimulation, rising CO₂, and a sudden drop in intrathoracic pressure — which physically expands the alveoli and mechanically clears lung liquid. This expansion triggers a dramatic fall in PVR. The rise in arterial oxygen tension that follows promotes functional closure of the ductus arteriosus (and later its permanent anatomical closure over weeks), while the increase in left atrial pressure functionally closes the foramen ovale. The result is the adult circulation pattern in which all pulmonary venous blood enters the left heart for systemic distribution.
When any of these steps fail — most commonly because the neonate fails to take effective first breaths — PVR remains high, the shunts remain open, pulmonary blood flow stays low, and a vicious hypoxic cycle begins: hypoxaemia → pulmonary vasoconstriction → more right-to-left shunting → worsening hypoxaemia. The therapeutic logic of PPV is to break this cycle mechanically: inflating the lungs with positive pressure drops PVR, increases pulmonary blood flow, and allows the normal transition to proceed.
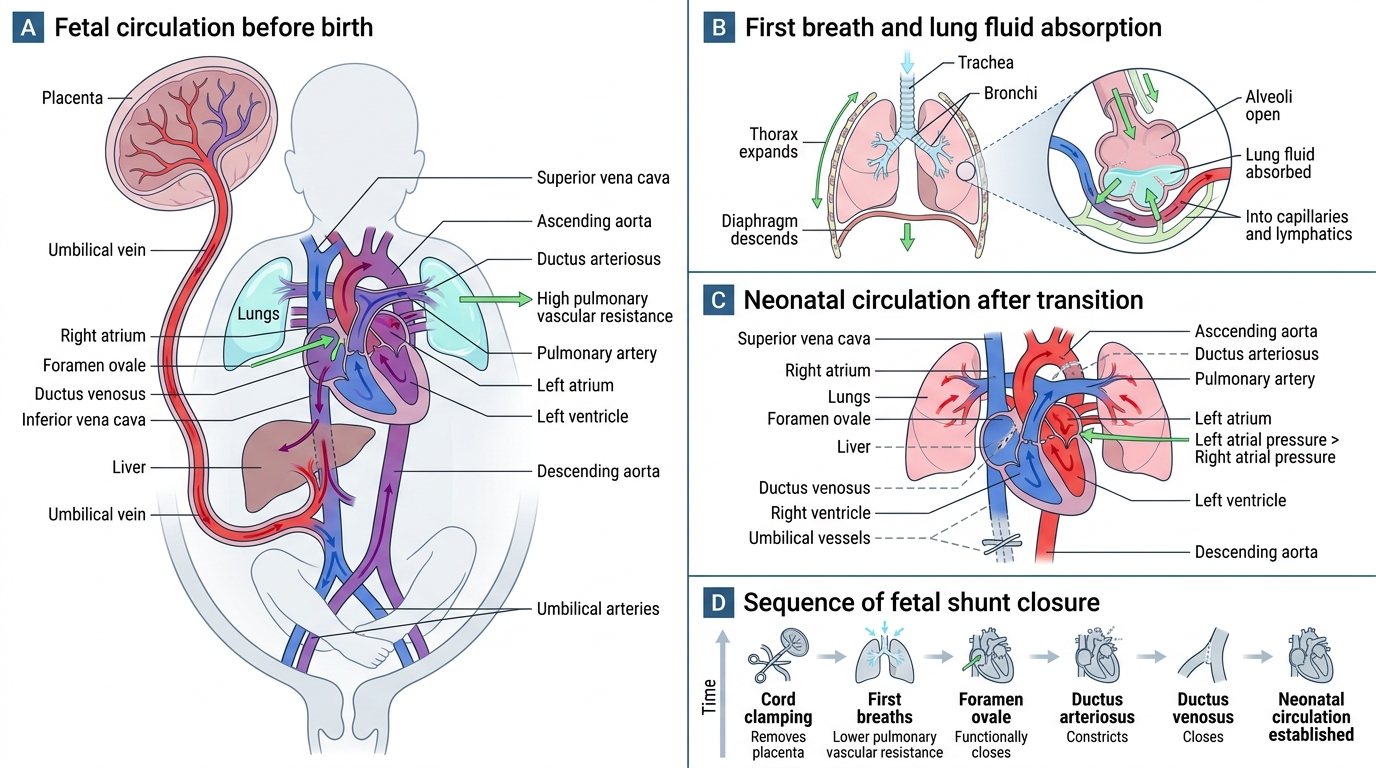
Fetal-to-Neonatal Circulatory Transition
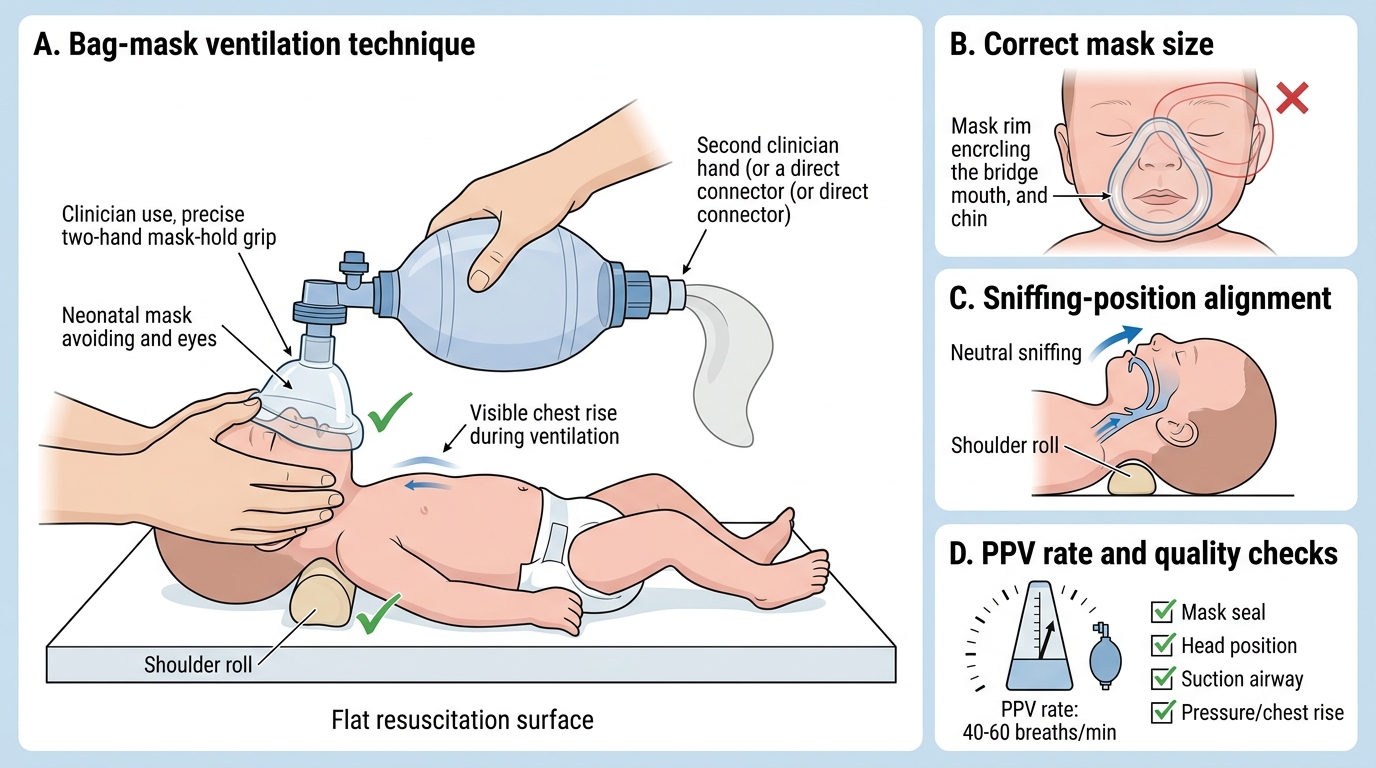
Key anatomical principle for PPV: the neonatal airway is narrow (proportionally smaller than an adult's), the epiglottis is more anterior and cephalad, and the larynx is at the C3-C4 level (vs C5-C6 in adults). This means neutral head position (a small shoulder roll to prevent neck flexion) rather than full head-tilt is the optimal airway position in the neonate. Over-extension compresses the trachea.
The NRP Sequence: Initial Steps, Assessment and PPV
The NRP algorithm begins with a rapid risk assessment before the baby is born — you answer three questions at birth: (1) Is the baby term? (2) Is the baby crying or breathing? (3) Does the baby have good muscle tone? If YES to all three, the baby can remain with the mother for routine care. If NO to any one, proceed immediately to the resuscitation warmer. The reason for this binary sorting is speed: every second spent at the mother's side without warming and stimulating is a second of cooling and unresuscitated hypoxia. The warmer, equipment, and a trained person must all be in place BEFORE the baby arrives — preparation is the first act of resuscitation.
Initial steps (approximately 30 seconds): At the warmer, perform all four initial steps in rapid sequence — they are often remembered by the mnemonic WARM-DRY-STIMULATE-REPOSITION:
• Warm — pre-warmed towels and radiant warmer; for preterm <32 weeks, use a polyethylene wrap instead of drying to minimise heat loss.
• Dry and stimulate — brisk drying of the body and head provides both heat and tactile stimulation to initiate breathing; discard wet towels.
• Reposition airway — place the baby supine, place a small folded towel under the shoulders to bring the head to 'sniffing position' (neutral neck, neither flexed nor hyperextended); this aligns oral-pharyngeal-laryngeal axes.
• Clear secretions — if obvious secretions are present, suction mouth THEN nose with a bulb syringe (NB: suction mouth first — stimulating the nose first can cause reflex apnoea); limit to 5 seconds per suction pass; suction pressure ≤100 mmHg if mechanical.
Breathing and heart-rate assessment (end of 30 seconds): After initial steps, simultaneously assess: Is the baby breathing? What is the heart rate? The quickest clinical method is to feel the base of the umbilical cord for pulsations, which closely reflects HR. Auscultation with a stethoscope placed over the left precordium is the gold standard. Pulse oximetry (probe on the RIGHT hand — pre-ductal) gives SpO₂ but may take 1–2 minutes to register a reliable signal.
Trigger for PPV: Apnoeic OR heart rate < 100 bpm → start PPV within the Golden Minute. PPV is delivered with a bag-mask device (either a flow-inflating bag requiring a gas source, or a self-inflating bag, which works without a gas source — important in resource-limited settings). Use the correct mask size — it covers the mouth and nose but NOT the eyes. Apply a good seal. Rate = 40–60 breaths per minute. The instructor mnemonic 'Squeeze-TWO-THREE' (squeeze on 'squeeze', release over 'TWO-THREE') helps maintain the correct rate. Pressure: initial inflation pressure ~20–25 cmH₂O in term babies (higher — up to 30–40 cmH₂O — may be needed for the first breath to overcome surface tension); watch for visible chest rise as the primary indicator of adequate ventilation. After 30 seconds of PPV, reassess HR:
• HR ≥100 and spontaneous breathing → wean PPV, monitor
• HR 60–99 → continue PPV, check mask seal, head position, suction, increase pressure if needed
• HR < 60 → continue PPV AND begin chest compressions
Neonatal Bag-Mask Ventilation Technique
SELF-CHECK
A term neonate is apnoeic after initial steps. You start PPV. After 30 seconds, the heart rate is 75 bpm. What is your next action?
A. Stop PPV — the heart rate is above 60
B. Start chest compressions immediately because the heart rate is below 100
C. Continue PPV and reassess mask seal, head position, suction, and pressure — escalate to compressions only if HR falls below 60
D. Administer epinephrine via the umbilical vein
Reveal Answer
Answer: C. Continue PPV and reassess mask seal, head position, suction, and pressure — escalate to compressions only if HR falls below 60
HR 60–99 bpm after 30 seconds of PPV: do NOT start compressions yet. First troubleshoot PPV quality — check mask seal (most common failure), head position (neutral sniffing position), suction (clear airway), and increase pressure if chest is not rising. Chest compressions are indicated only if HR remains <60 bpm after 30 seconds of ADEQUATE ventilation. Epinephrine is a later step.