Page 17 of 32
OG18.{2,4} | Neonatal Resuscitation — SDL Guide (Part 2)
Chest Compressions and the 3:1 Neonatal Ratio
Chest compressions in neonatal resuscitation are a later-line intervention, used only when the heart rate remains below 60 bpm after 30 seconds of adequate positive-pressure ventilation (i.e., ventilation confirmed to be producing chest rise, not merely attempted). The cardinal rule is: ventilation is the priority. Most neonates respond to effective PPV alone; compressions are needed in <1% of deliveries.
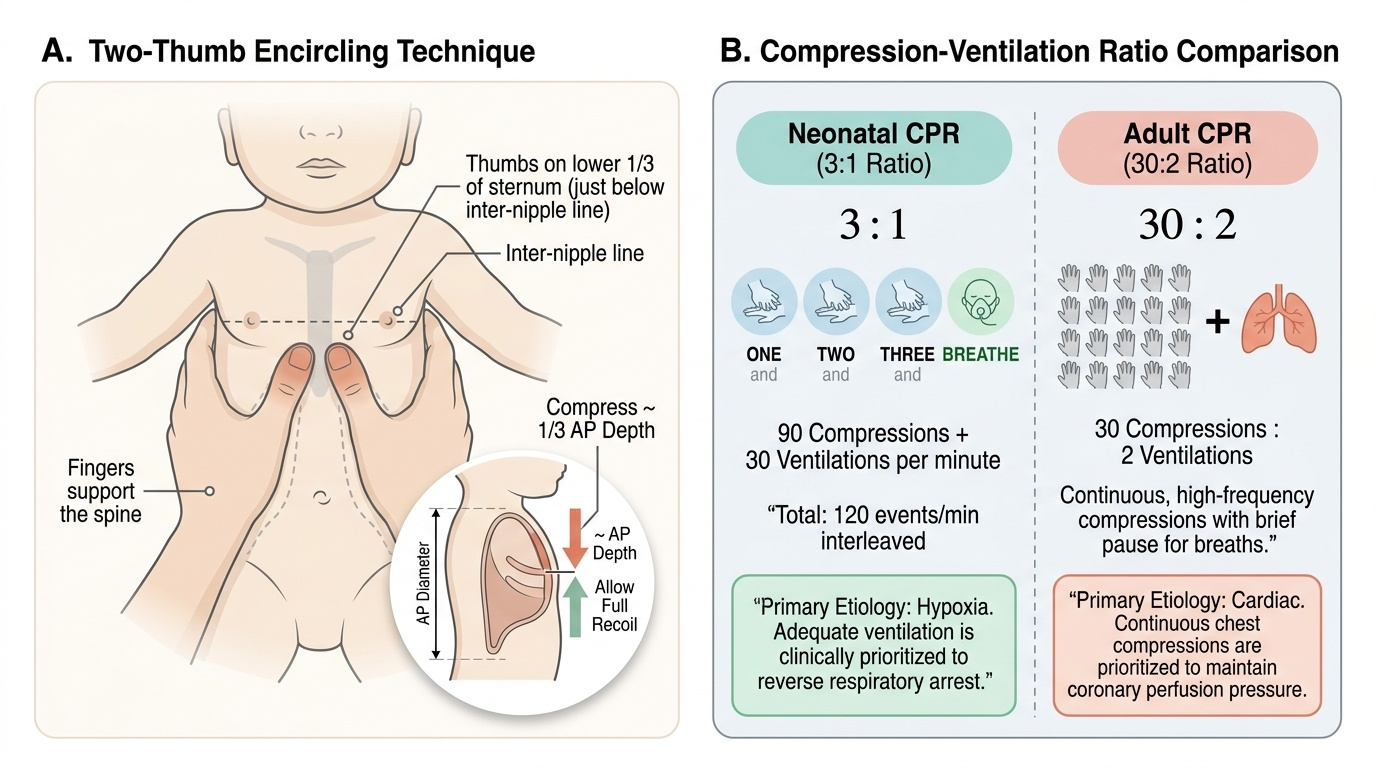
When compressions are indicated, use the two-thumb encircling technique as the preferred method in neonates: encircle the chest with both hands, thumbs placed on the lower one-third of the sternum (just below the inter-nipple line), fingers supporting the back. The two-finger technique (index and middle finger on the sternum) is acceptable if the resuscitator cannot encircle the chest (e.g., when umbilical venous access is simultaneously being obtained). Compress the sternum to a depth of approximately one-third of the anterior-posterior diameter of the chest. After each compression, allow full recoil — partial recoil reduces venous return.
The neonatal compression-ventilation ratio is 3:1 — NOT the adult 30:2. This distinction is tested repeatedly in exams and is clinically critical. The rationale: in neonates, the most common cause of cardiac arrest is hypoxia (not a primary cardiac event as in adults), so adequate ventilation is proportionally more important per unit time. A ratio of 3:1 provides 30 compressions and 10 ventilations per minute when the rhythm is 90/min compressions + 30/min ventilations interleaved. The mnemonic is 'ONE-and-TWO-and-THREE-and-BREATHE' — compressing on 'ONE', 'TWO', 'THREE' and pausing for a ventilation on 'BREATHE.'
Provided image
After 45–60 seconds of coordinated CPR (3:1), check the heart rate again. If HR ≥60 bpm → stop compressions, continue PPV. If HR remains <60 bpm despite adequate CPR → consider:
• Epinephrine (adrenaline): 0.01–0.03 mg/kg IV (or IO) via umbilical venous catheter (UVC) is the preferred route; ETT route is less reliable. Concentration used = 1:10,000 (0.1 mg/mL).
• Volume expansion (if suspected blood loss/hypovolaemia): normal saline 10 mL/kg IV over 5–10 minutes.
• Consider whether ventilation is truly adequate — intubation may be needed.
Common errors in simulation drills: (1) starting compressions before confirming adequate ventilation, (2) using adult 30:2 ratio, (3) incorrect hand position (too high on sternum → ineffective; too low → liver injury), (4) incomplete chest recoil.
Meconium-Stained Amniotic Fluid: Special Pathway
Meconium-stained amniotic fluid (MSAF) occurs in approximately 10–15% of deliveries, more commonly in post-term pregnancies and in fetuses experiencing intrauterine stress (e.g., cord compression, placental insufficiency, maternal hypoxia). When a fetus passes meconium in utero and then gasps — whether before or after delivery — meconium can enter the lower airways, causing the dreaded meconium aspiration syndrome (MAS). MAS carries significant morbidity through three linked mechanisms: direct airway obstruction (ball-valve plugging of bronchioles), chemical pneumonitis (meconium constituents trigger a severe inflammatory response in the alveolar epithelium), and persistent pulmonary hypertension of the newborn (the inflammatory and hypoxic milieu raises PVR and reopens fetal shunts). Understanding these mechanisms explains both what you are trying to prevent and why the decision tree is based on the INFANT's condition rather than simply the colour of the liquor. The management approach has been substantially revised over the last decade based on robust multicentre evidence.
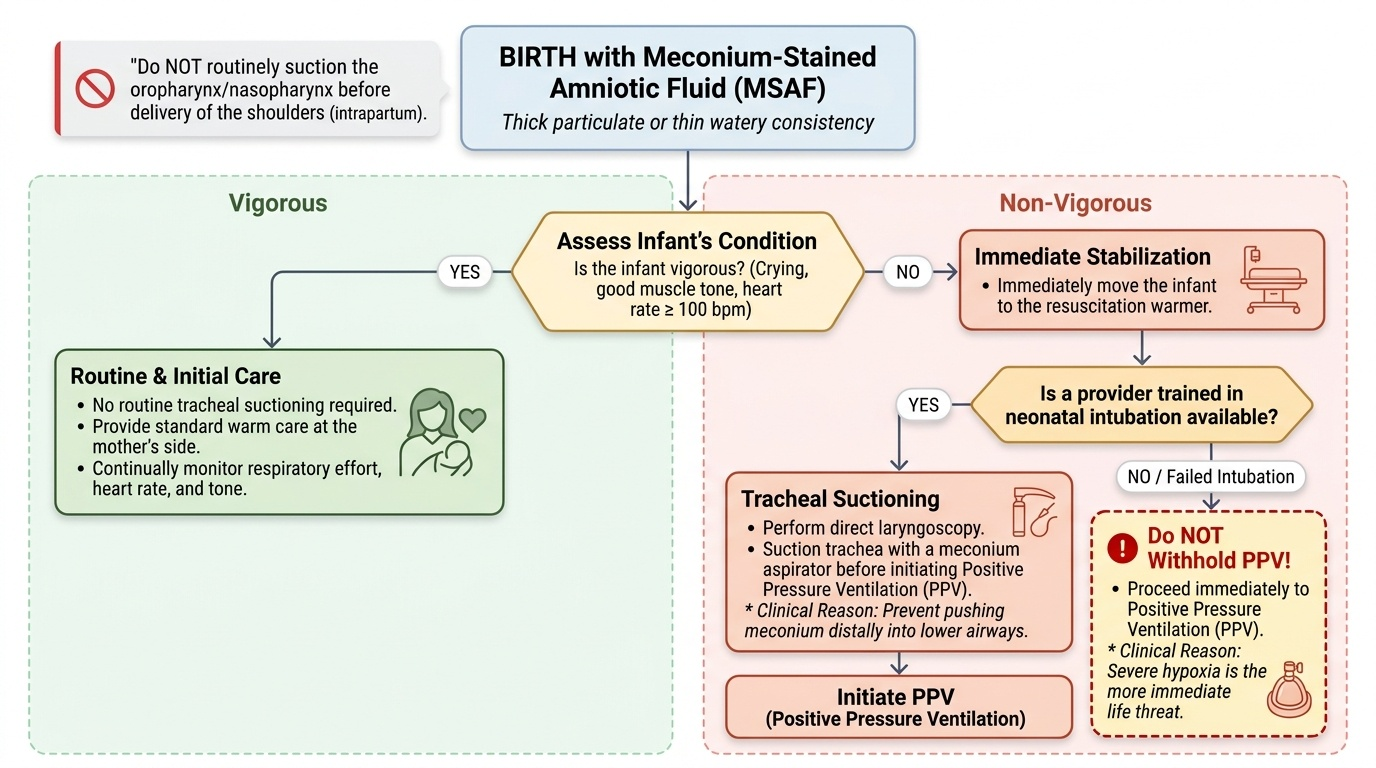
Current NRP guidance (7th/8th edition, endorsed by ILCOR): Do NOT routinely suction the oropharynx or nasopharynx of the baby before delivery of the shoulders (intrapartum suctioning was abandoned because a landmark multicentre RCT — the Carson et al. 1996 trial, with confirmatory ILCOR reviews — showed no benefit and possible harm from this practice). After birth:
• Vigorous baby (crying, good muscle tone, HR >100): no routine tracheal suctioning. Proceed with routine/initial care at mother's side.
• Non-vigorous baby (absent or poor respiratory effort, limp tone, HR <100): proceed to resuscitation warmer. If the care provider is trained in neonatal intubation, perform direct laryngoscopy and tracheal suctioning with a meconium aspirator before initiating PPV, because introducing PPV in the presence of meconium in the trachea can push it distally.
• If intubation skills are not available or if intubation fails, do NOT withhold PPV — hypoxia is the more immediate threat.
Thin watery MSAF vs thick particulate MSAF: Thick, pea-soup meconium is considered higher risk for MAS, but management decisions are based on the INFANT'S condition (vigorous vs non-vigorous), not solely on meconium consistency. This is an important nuance.
A word of caution: the Indian context includes many deliveries in secondary-care and first-referral units where laryngoscopy skill may be limited. The FOGSI/NNF guidelines align with NRP 7th edition: routine intrapartum suctioning is NOT recommended; post-delivery decisions are based on the infant's condition.
Provided image
SELF-CHECK
A post-term baby is born through thick meconium-stained amniotic fluid. The baby is limp, not breathing, and heart rate is 60 bpm. What is the MOST appropriate immediate action according to current NRP guidelines?
A. Suction the oropharynx before cutting the cord, then take to warmer
B. Start PPV immediately with bag-mask at the warmer
C. Take to the warmer, perform direct laryngoscopy and tracheal suctioning before initiating PPV if intubation skill is available
D. Administer surfactant via endotracheal tube
Reveal Answer
Answer: C. Take to the warmer, perform direct laryngoscopy and tracheal suctioning before initiating PPV if intubation skill is available
This is a non-vigorous baby (limp, apnoeic, HR 60). NRP: take to warmer first; if intubation skills are available, perform direct laryngoscopy and tracheal suction before PPV to prevent pushing meconium distally. If intubation is not available, start PPV — do not withhold. Intrapartum (before-shoulders) suctioning is NOT recommended. Surfactant is not the initial step.
Interpreting Response: Apgar Score and Ongoing Assessment
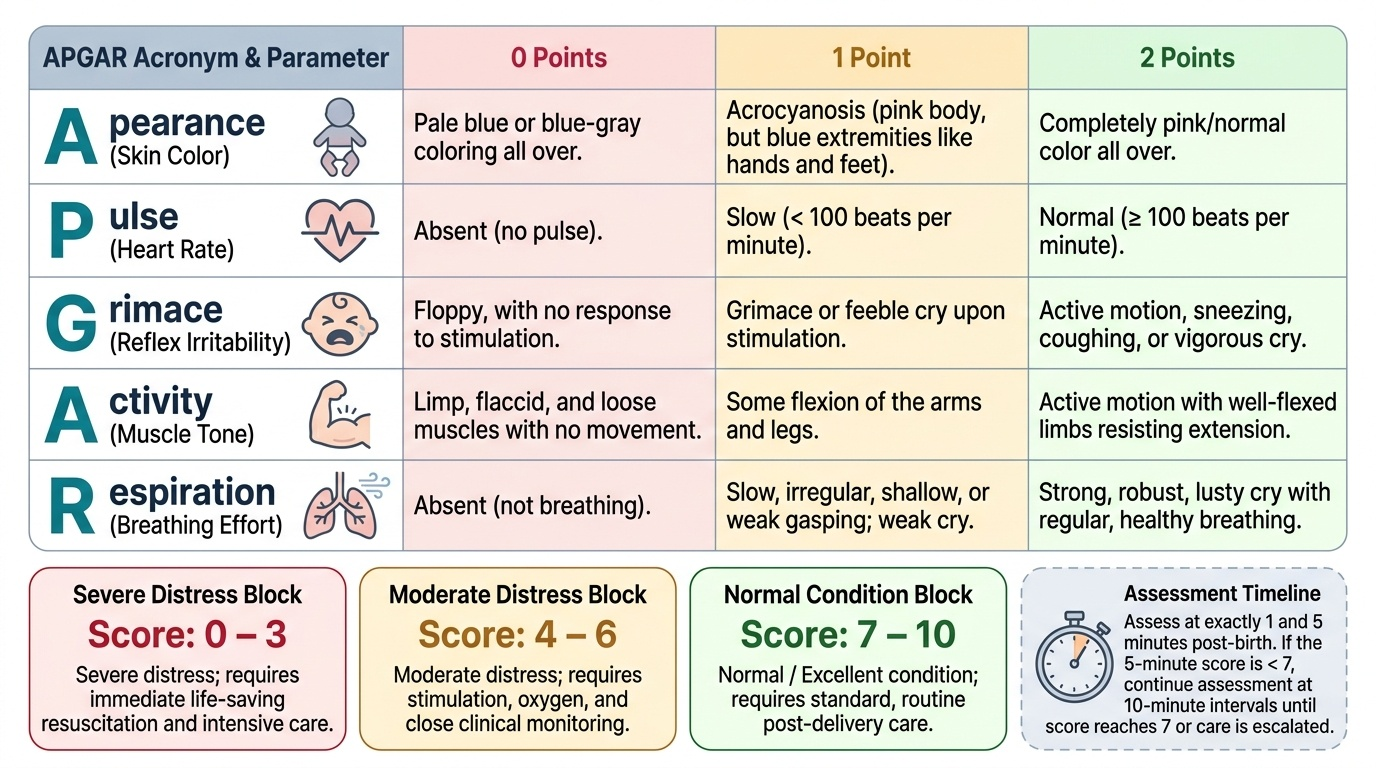
The Apgar score was introduced by Dr Virginia Apgar in 1952 as a rapid, standardised method to communicate the condition of the newborn at birth and to guide post-delivery care decisions. Before its introduction, there was no consistent way for birth attendants to document the infant's status or to communicate it meaningfully to the receiving paediatric team. The score uses five easily observable parameters, each reflecting a different physiological domain — cardiovascular status, respiratory effort, neurological tone, reflex integration, and peripheral perfusion — and assigns 0, 1, or 2 points to each, giving a maximum total of 10. It is recorded at exactly 1 minute (reflecting the condition at the time of birth) and 5 minutes (reflecting the response to resuscitative efforts); if the 5-minute score is below 7, the assessment continues at 10-minute intervals until it reaches 7 or the clinical team decides on escalation of care. The 1-minute score alone should never be used as the sole determinant of neonatal outcome, since many normal babies have a depressed 1-minute score that fully corrects. The parameters are remembered by the acronym APGAR itself:
| Parameter | 0 | 1 | 2 |
|---|---|---|---|
| Appearance (colour) | Blue/pale all over | Pink body, blue extremities | Pink all over |
| Pulse (heart rate) | Absent | <100 bpm | ≥100 bpm |
| Grimace (reflex irritability) | No response | Grimace/feeble cry | Cry, cough, sneeze |
| Activity (muscle tone) | Limp | Some flexion | Active motion |
| Respiration | Absent | Weak/irregular | Strong cry |
Interpretation bands: Score 7–10 = normal; 4–6 = moderately depressed (may need stimulation, supplemental O₂, brief PPV); 0–3 = severely depressed (requires immediate resuscitation).
Provided image
Two important caveats about the Apgar score:
1. The Apgar score is a RETROSPECTIVE assessment tool, not a resuscitation decision-making tool. Resuscitation decisions are made in real time based on breathing and heart rate — you do not wait 60 seconds to calculate an Apgar before starting PPV.
2. Normal Apgar does NOT equal normal outcome — a baby who scores 3 at 1 minute but 7 at 5 minutes after resuscitation may still have experienced significant hypoxic-ischaemic injury requiring neonatal unit monitoring. Conversely, a low Apgar at 1 minute in a premature baby may reflect immaturity rather than asphyxia.
Ongoing post-resuscitation monitoring focuses on: SpO₂ (pre-ductal probe on right hand), HR, capillary refill time, blood glucose (hypoglycaemia is a common post-resuscitation complication — target ≥2.6 mmol/L), temperature, and neurological status. Any baby who required chest compressions or epinephrine should be transferred to a neonatal unit for observation and monitoring for HIE.