Page 1 of 32
OG17.1 | Physiology of Lactation and BFHI — SDL Guide
Learning Objectives
- Describe the stages of mammary gland development (mammogenesis) during pregnancy and lactation
- Explain the hormonal regulation of milk synthesis including the roles of prolactin, progesterone, oestrogen, and human placental lactogen
- Describe the neuroendocrine pathway of the milk-ejection reflex mediated by oxytocin
- Distinguish colostrum, transitional milk, and mature milk by composition and immunological properties
- Enumerate the WHO/UNICEF Baby-Friendly Hospital Initiative (BFHI) 10 Steps to Successful Breastfeeding and justify each step with physiological evidence
- Identify clinical situations that require modification or cessation of breastfeeding
INSTRUCTIONS
Lactation is a defining event in postpartum care. A sound understanding of the hormonal machinery driving milk production and the evidence-based practices enshrined in the BFHI equips you to support mothers effectively, troubleshoot feeding problems at the bedside, and counsel about the benefits and limits of breastfeeding. This module covers both the biology and the hospital-level policy that translates that biology into practice.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch. 17 — Lactation (textbook)
- Williams Obstetrics, 25th ed., Ch. 36 — The Puerperium (textbook)
- WHO/UNICEF, Baby-Friendly Hospital Initiative: Revised, Updated and Expanded for Integrated Care, 2009 (revised 2018) (guideline)
- Ganong's Review of Medical Physiology, 26th ed. — Pituitary Hormones and Lactation (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 26-year-old primipara delivered a healthy male neonate 18 hours ago via normal vaginal delivery. The baby has been crying persistently and the mother is anxious that her breasts are 'empty'. The neonatology nurse mentions that the mother has not yet attempted skin-to-skin contact. You are the junior resident on the postnatal ward — what do you tell her? Understanding why milk has not yet appeared in abundance, what colostrum does for the newborn in these critical early hours, and how to initiate a positive breastfeeding experience is the foundation of postnatal care.
WHY THIS MATTERS
Breastfeeding rates in India remain below global targets, and a significant proportion of women who intend to breastfeed stop within the first month, often because of problems that are preventable with timely, evidence-based support. As an obstetrician, you will counsel women about breastfeeding initiation during antenatal visits, manage early postnatal challenges on the ward, and certify institutions under the BFHI. The physiology you learn here underpins every clinical decision: why early suckling matters, why stress inhibits milk let-down, why exclusive breastfeeding for 6 months is physiologically achievable, and why certain maternal medications or infections require breastfeeding to be modified or stopped. These are not isolated facts — they form a coherent neuroendocrine narrative that guides practical care.
RECALL
Before proceeding, activate prior knowledge:
- Hypothalamo-pituitary axis: Recall that the anterior pituitary secretes prolactin from lactotroph cells, regulated by dopamine (inhibitory, from the hypothalamus) and thyrotropin-releasing hormone (stimulatory). The posterior pituitary releases oxytocin synthesised in the paraventricular and supraoptic nuclei.
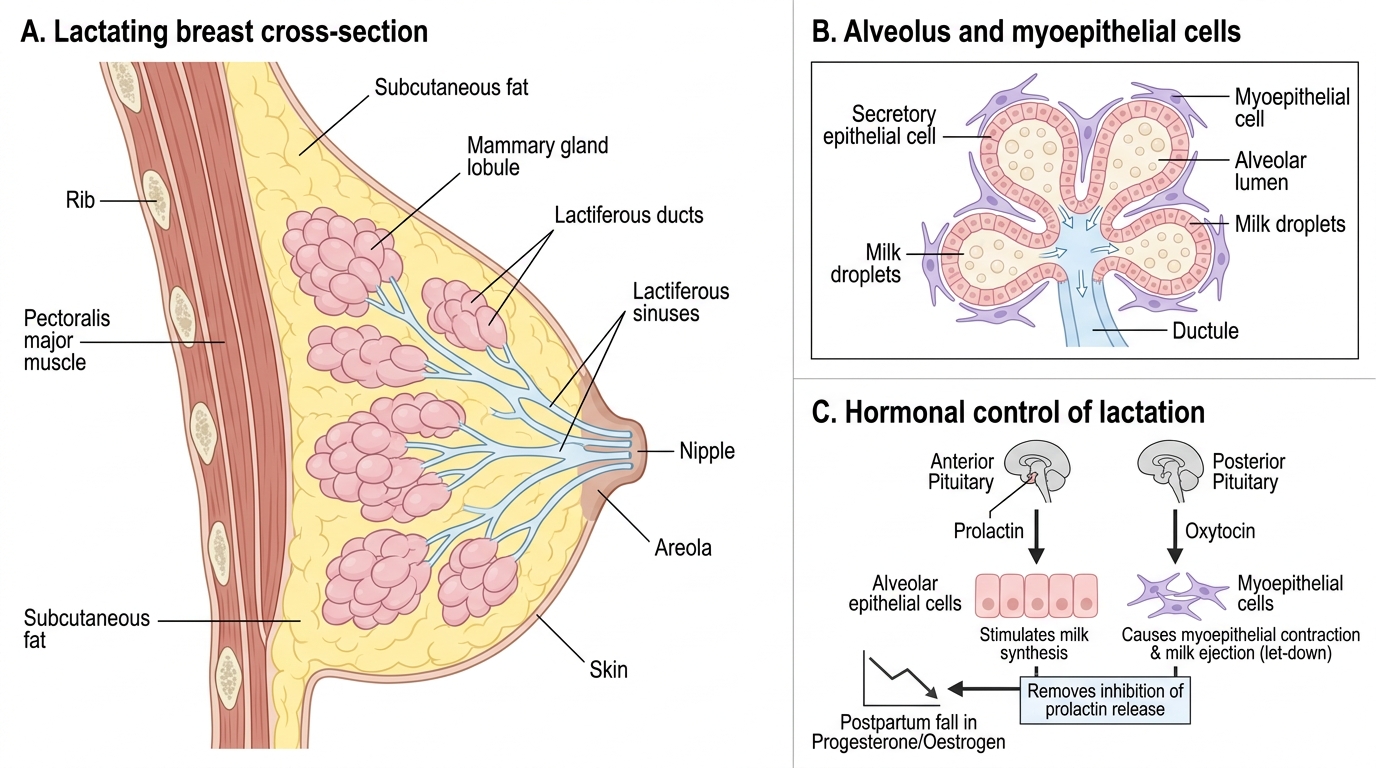
- Mammary gland anatomy: The gland is composed of 15–20 lobes, each divided into lobules containing secretory alveoli lined by secretory epithelial cells surrounded by myoepithelial cells. Lactiferous ducts converge at the nipple-areola complex.
- Hormones of pregnancy: Oestrogen, progesterone, and human placental lactogen (HPL) rise progressively. Oestrogen drives ductal proliferation; progesterone and HPL drive alveolar development.
- Immune immunoglobulins: Recall IgA (secretory form = sIgA) as the primary mucosal immunoglobulin; it is the dominant antibody in breast milk.
Why Lactation Physiology Matters for the Obstetrician
Lactation is not a passive phenomenon that occurs automatically after delivery — it is an active, hormonally orchestrated process that requires specific environmental conditions (particularly early, frequent suckling and skin-to-skin contact) to establish and maintain. The World Health Organization recommends exclusive breastfeeding for the first six months of life, followed by continued breastfeeding alongside complementary foods until two years of age or beyond. The epidemiological evidence for this recommendation is compelling: exclusively breastfed infants have significantly lower rates of diarrhoeal disease, pneumonia, otitis media, and neonatal sepsis compared with formula-fed infants. For the mother, breastfeeding reduces the risk of postpartum haemorrhage (through oxytocin-mediated uterine involution), suppresses ovulation (lactational amenorrhoea as a natural contraceptive method), and reduces long-term risks of breast and ovarian cancer.
Despite these benefits, global breastfeeding initiation and exclusive breastfeeding rates fall well short of WHO targets. India's National Family Health Survey (NFHS-5, 2019–21) recorded early initiation of breastfeeding (within one hour of birth) at approximately 41.8% nationally — a figure that highlights the gap between evidence and practice. The Baby-Friendly Hospital Initiative (BFHI), launched by WHO and UNICEF in 1991, was designed precisely to bridge this gap by embedding breastfeeding-supportive practices into hospital policy and routine care. As a clinician, knowing the physiology is inseparable from knowing how to apply it — every BFHI step has a physiological justification you will learn in this module.
Structure of the Lactating Breast: Mammogenesis and Anatomy
Mammogenesis refers to the process by which the mammary gland develops to its full secretory capacity. This occurs in stages that span puberty, the luteal phase of each menstrual cycle, and pregnancy. Understanding these stages clarifies why certain hormonal events — particularly progesterone withdrawal after delivery — are pivotal triggers for milk production.
At puberty, rising oestrogen stimulates ductal elongation and branching. Progesterone, present during the luteal phase, drives limited alveolar budding. During pregnancy, a more profound structural transformation occurs: oestrogen (from the placenta and corpus luteum) causes marked ductal proliferation, while progesterone and HPL (human placental lactogen, also called human chorionic somatomammotropin) together stimulate extensive alveolar development. The alveoli — the milk-secreting units — are lined by two cell types: the inner secretory epithelial cells (lactocytes) that synthesise and secrete milk into the alveolar lumen, and the outer myoepithelial cells that contract under oxytocin stimulation to propel milk into the ducts. By the third trimester, the gland has undergone complete lobuloalveolar development and is structurally ready to produce milk.
The nipple-areola complex is richly innervated with sensory afferent fibres, particularly around the nipple base and areola. This innervation is the afferent limb of the milk-ejection reflex — mechanical stimulation by the infant's gums and tongue initiates afferent nerve impulses that travel to the hypothalamus. The areola also contains Montgomery's glands (sebaceous glands of modified structure) that secrete lubricating substances and odorants that may guide the neonate to the nipple.
IMARK: The size of the breast does not determine milk-producing capacity — capacity depends on the number and functional state of alveoli, not on adipose tissue volume.
Lactating Breast: Structure and Hormonal Control
Hormonal Control of Milk Synthesis: Prolactin, Progesterone, and Lactogenesis
Milk synthesis is regulated by a sequence of hormonal events divided into two stages of lactogenesis — a term coined to distinguish the initiation phases from the maintenance phase (galactopoiesis).
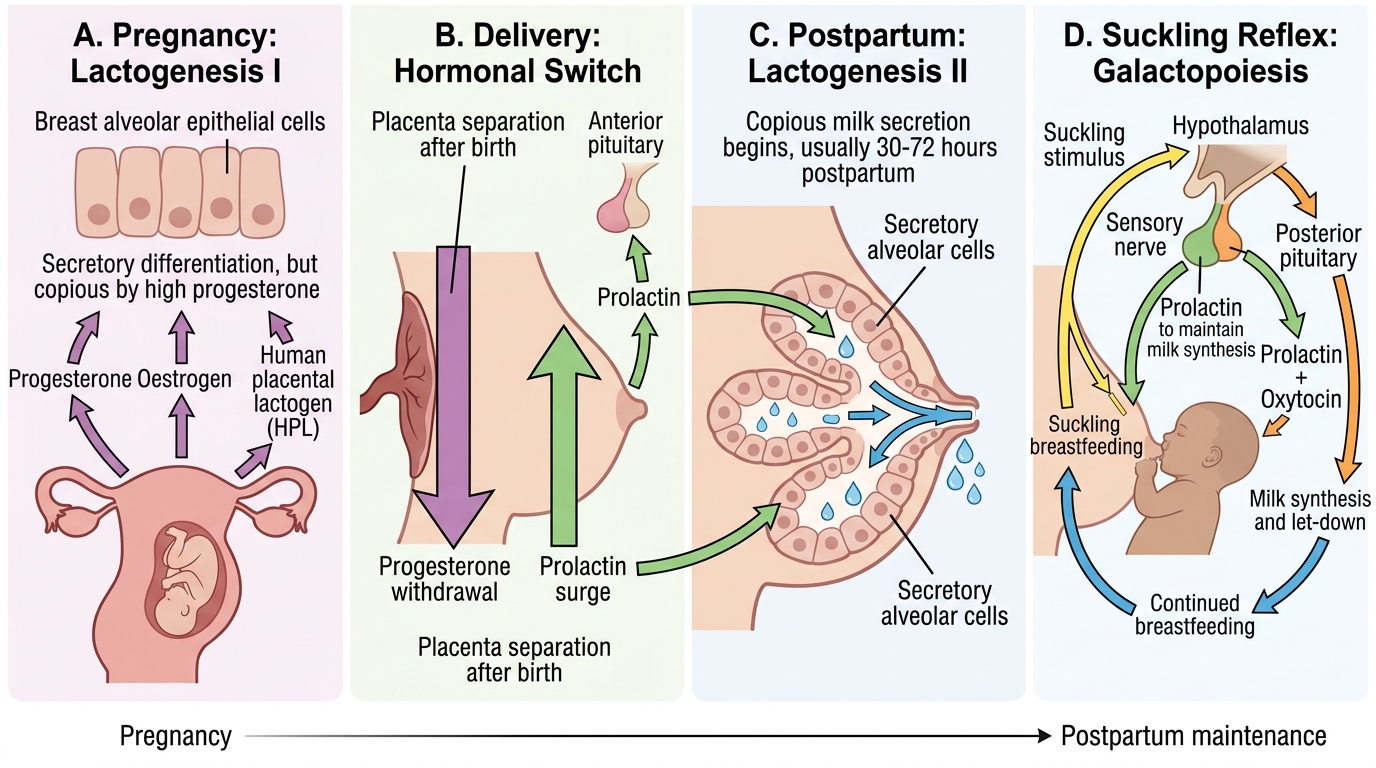
Lactogenesis Stage I (mid-pregnancy, approximately 16–22 weeks onwards) refers to the onset of secretory differentiation, during which the alveolar cells acquire the biosynthetic machinery to produce milk components — caseins, lactose, and fat. During this stage, small volumes of colostrum can be expressed from the breast. Importantly, lactogenesis I is driven by prolactin (secreted by lactotrophs of the anterior pituitary under stimulation from TRH and inhibited by dopamine from the hypothalamus) and HPL. However, full, copious milk secretion does not occur because progesterone — at high circulating levels throughout pregnancy — competitively inhibits prolactin at the alveolar cell receptor. Oestrogen paradoxically suppresses prolactin receptor signalling as well.
Lactogenesis Stage II is defined as the transition to copious, secretory milk production. This occurs 30–72 hours postpartum and is triggered primarily by the abrupt fall in progesterone (and oestrogen) that follows delivery of the placenta. With the progesterone block removed, prolactin — whose levels are still markedly elevated postpartum — can now act unopposed at alveolar cell receptors, driving full-scale milk synthesis. This is why delayed placental delivery or a retained placental fragment can delay or inhibit milk coming in: circulating progesterone remains elevated, blocking the prolactin effect. Clinically, mothers should be reassured that this delay is normal in the first 24 hours and that early, frequent suckling accelerates the transition.
Galactopoiesis (maintenance of established lactation) depends on the continued release of prolactin in response to infant suckling. Each feed stimulates a spike in prolactin, which is essential for producing milk for the NEXT feed. This supply-demand relationship is the physiological basis for the clinical advice to feed 'on demand' — the more frequently and effectively the infant suckles, the higher the cumulative prolactin exposure and the greater the milk yield. Conversely, abrupt cessation of suckling leads to falling prolactin levels, alveolar involution, and cessation of lactation within days to weeks.
IMARK: Prolactin also suppresses GnRH pulsatility at the hypothalamus, leading to anovulation and lactational amenorrhoea. This effect is most reliable when breastfeeding is frequent, exclusive, and around the clock — the basis of the Lactational Amenorrhoea Method (LAM) of contraception.
Hormonal Control of Lactation