Page 2 of 32
OG17.1 | Physiology of Lactation and BFHI — SDL Guide (Part 2)
Milk Ejection: The Oxytocin Reflex and Galactopoiesis
Milk synthesis by the alveolar cells fills the alveolar lumen and the small ductules, but milk does not reach the nipple by gravity alone — it must be actively expelled. This is the function of the milk-ejection reflex (also called the let-down reflex), mediated by oxytocin released from the posterior pituitary.
The reflex arc operates as follows: mechanical stimulation of the nipple-areola by the infant's suckling activates sensory afferent fibres, which send impulses via the spinal cord to the hypothalamus. In response, magnocellular neurons in the paraventricular (PVN) and supraoptic nuclei (SON) of the hypothalamus release oxytocin into the systemic circulation from axon terminals in the posterior pituitary. Oxytocin binds to receptors on the myoepithelial cells surrounding the alveoli, causing them to contract. This contraction squeezes milk from the alveolar lumen into the larger lactiferous sinuses and towards the nipple, where the infant can extract it.
Critically, the reflex can be conditioned: many women experience let-down in response to the baby's cry, the sight of their baby, or even thinking about feeding, because higher cortical pathways can activate hypothalamic oxytocin release. Conversely, the reflex is powerfully inhibited by psychological stress, pain, embarrassment, and anxiety — all of which activate the sympathetic system and release adrenaline, which causes vasoconstriction and directly inhibits myoepithelial cell contraction. This explains why privacy, a calm environment, and skin-to-skin contact facilitate successful feeding, and why BFHI Step 7 (rooming-in) and Step 10 (community support) are physiologically rational.
Beyond milk ejection, oxytocin released during suckling has a second important postpartum function: it stimulates uterine contraction, accelerating involution and reducing the risk of postpartum haemorrhage. The uterine cramps (afterpains) some women feel during feeding in the first few postpartum days are a direct manifestation of this oxytocin effect.
IMARK: Galactopoiesis depends on BOTH hormones together — prolactin for synthesis and oxytocin for ejection. A mother may have adequate prolactin (and therefore adequate milk production) but poor feeding outcome if the let-down reflex is impaired by stress.
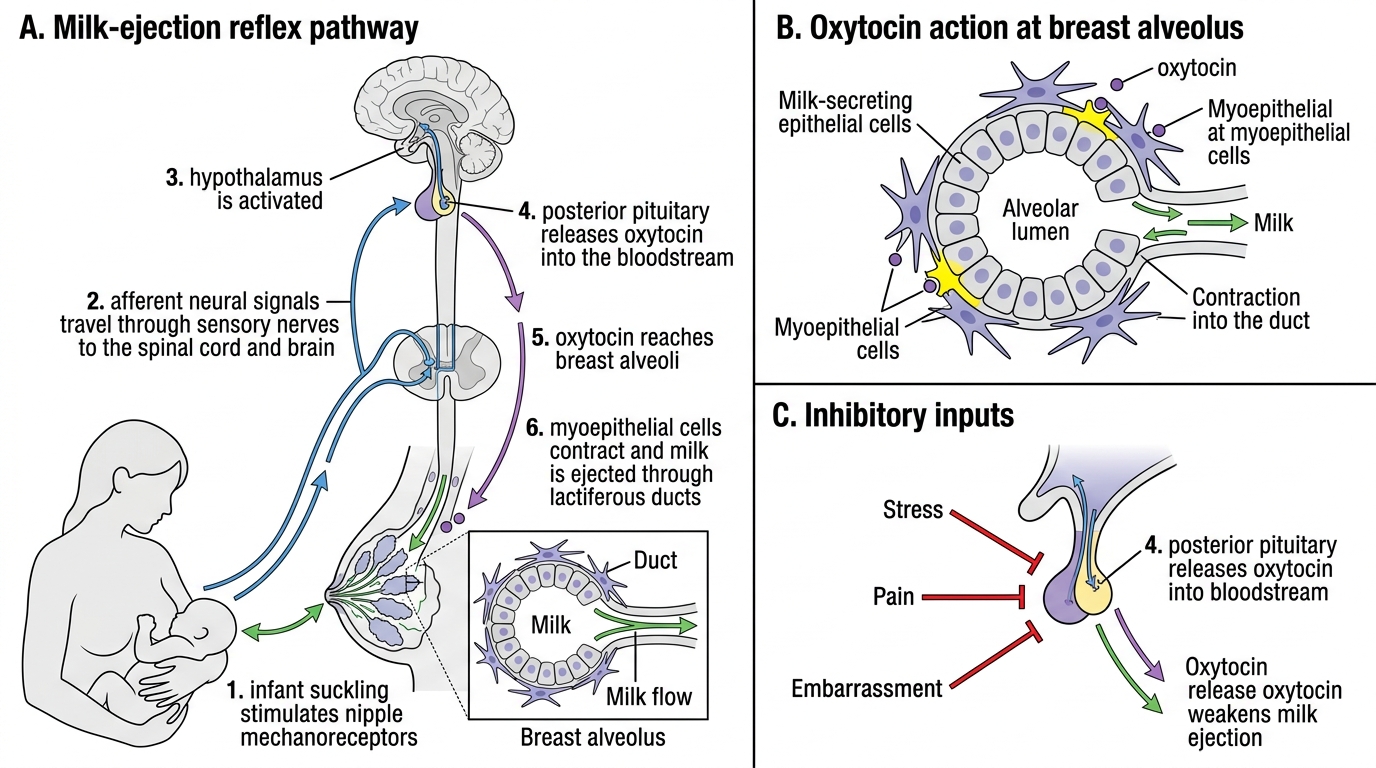
Milk-Ejection Reflex and Its Inhibition
Composition and Immunological Properties of Human Milk
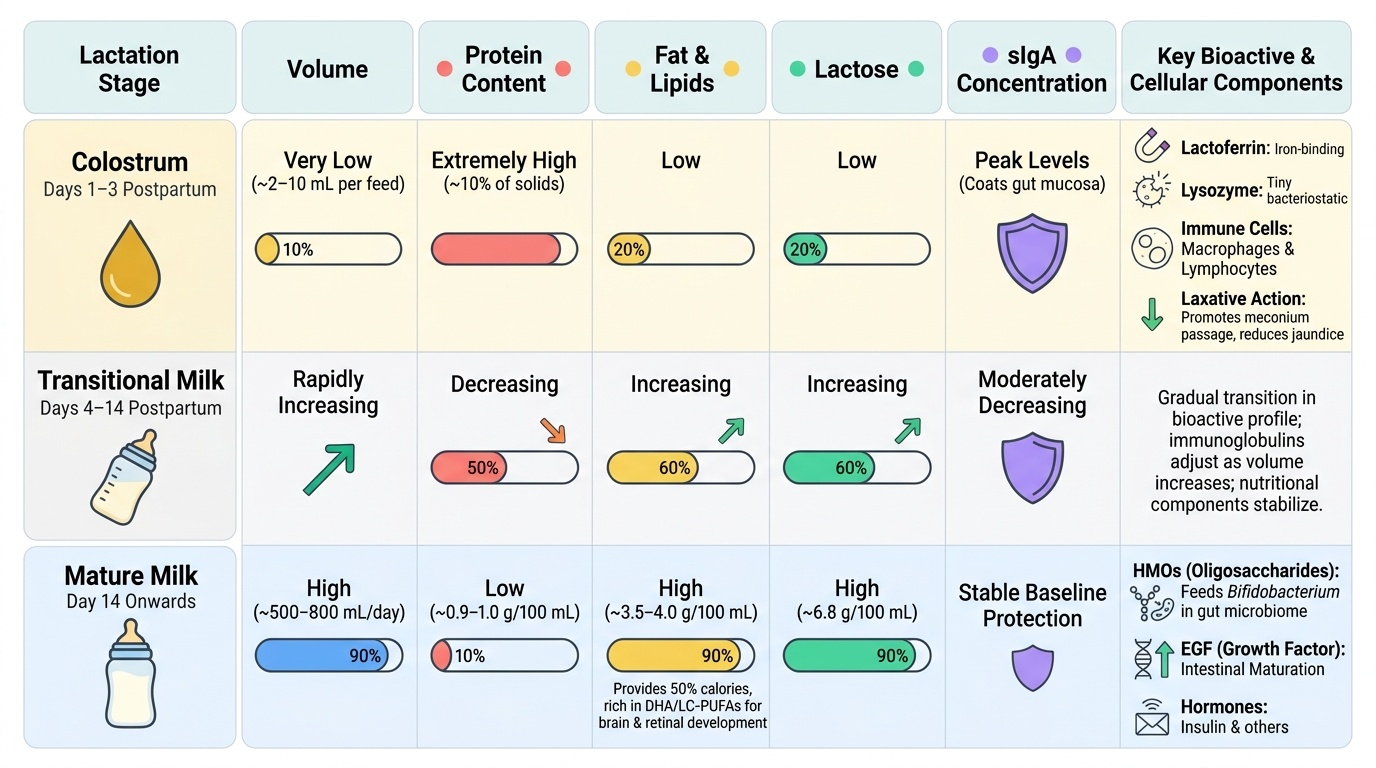
Human milk is not a static fluid — its composition changes dynamically over the first weeks of lactation and in response to the gestational age and needs of the infant. Three stages are conventionally described: colostrum, transitional milk, and mature milk.
Colostrum is the yellowish, thick fluid secreted in the first 2–3 days postpartum in small volumes (approximately 2–10 mL per feed initially). Its distinctive yellow colour reflects high concentrations of beta-carotene (a vitamin A precursor). Colostrum is protein-rich and relatively low in fat and lactose compared to mature milk. Its most important property is its extraordinarily high content of secretory IgA (sIgA), which coats the neonatal gastrointestinal mucosa and provides passive immune protection against enteric pathogens in the first days before the neonate's own immune system is functional. Colostrum also contains high concentrations of lactoferrin (iron-binding protein with bacteriostatic and antifungal effects), lysozyme (lytic against Gram-positive bacteria), macrophages, and lymphocytes. Colostrum is also mildly laxative, promoting the passage of meconium and reducing the enterohepatic circulation of bilirubin (thereby reducing neonatal jaundice). Mothers who are concerned about the small volume of colostrum should be reassured that it is ideally matched to neonatal gastric capacity in the first days.
Transitional milk replaces colostrum between approximately days 4 and 14. Volume increases substantially, immunoglobulin concentration falls toward mature levels, and fat and lactose content rise.
Mature milk (from about day 14 onwards) comprises approximately 88% water, with the remainder being carbohydrate (principally lactose, 6.8 g/100 mL), fat (3.5–4 g/100 mL), and protein (0.9–1 g/100 mL). Human milk fat is particularly important because it provides approximately 50% of the infant's caloric intake and contains long-chain polyunsaturated fatty acids (LC-PUFAs such as docosahexaenoic acid, DHA) that are critical for brain and retinal development. Mature milk also contains a rich array of bioactive factors: oligosaccharides (human milk oligosaccharides, HMOs) that selectively feed Bifidobacterium species in the infant gut microbiome; epidermal growth factor (EGF) promoting intestinal maturation; and hormones including insulin, IGF-1, and leptin.
Within a single feed, foremilk (produced at the start) is more watery and quenches thirst; hindmilk (produced as the alveolus empties) is fat-rich and provides caloric density. Effective attachment and complete drainage of the breast are essential for the infant to receive both components.
Provided image
SELF-CHECK
A new mother at 36 hours postpartum is worried her baby is not getting enough milk because her breasts do not feel 'full'. Which of the following best explains the physiology of her current stage of lactation?
A. Prolactin levels have fallen to pre-pregnancy levels, halting milk synthesis
B. Copious milk production (lactogenesis II) typically begins 30–72 hours postpartum after placental progesterone withdrawal
C. Oxytocin deficiency is preventing milk ejection from the alveoli
D. Colostrum production requires oestrogen replacement to initiate
Reveal Answer
Answer: B. Copious milk production (lactogenesis II) typically begins 30–72 hours postpartum after placental progesterone withdrawal
Lactogenesis II (onset of copious milk production) is triggered by the abrupt fall in progesterone following placental delivery, allowing prolactin to act unopposed on alveolar receptors. This transition typically occurs 30–72 hours postpartum. In the first 24–36 hours, small volumes of colostrum are normal and appropriate; reassuring the mother and encouraging frequent, effective suckling is the correct clinical response.
Baby-Friendly Hospital Initiative: The WHO/UNICEF 10 Steps
The Baby-Friendly Hospital Initiative (BFHI), launched jointly by WHO and UNICEF in 1991 and substantively revised in 2018, is the global framework for transforming hospital and clinic practices to support breastfeeding. Hospitals that implement all 10 Steps and are independently assessed may receive the Baby-Friendly designation. The initiative has been associated with significantly higher rates of breastfeeding initiation, exclusivity, and duration in multiple low-, middle-, and high-income country contexts. Understanding the rationale behind each step — grounded in the lactation physiology covered in this module — is what distinguishes a clinician who can advocate effectively for breastfeeding from one who merely recites guidelines.
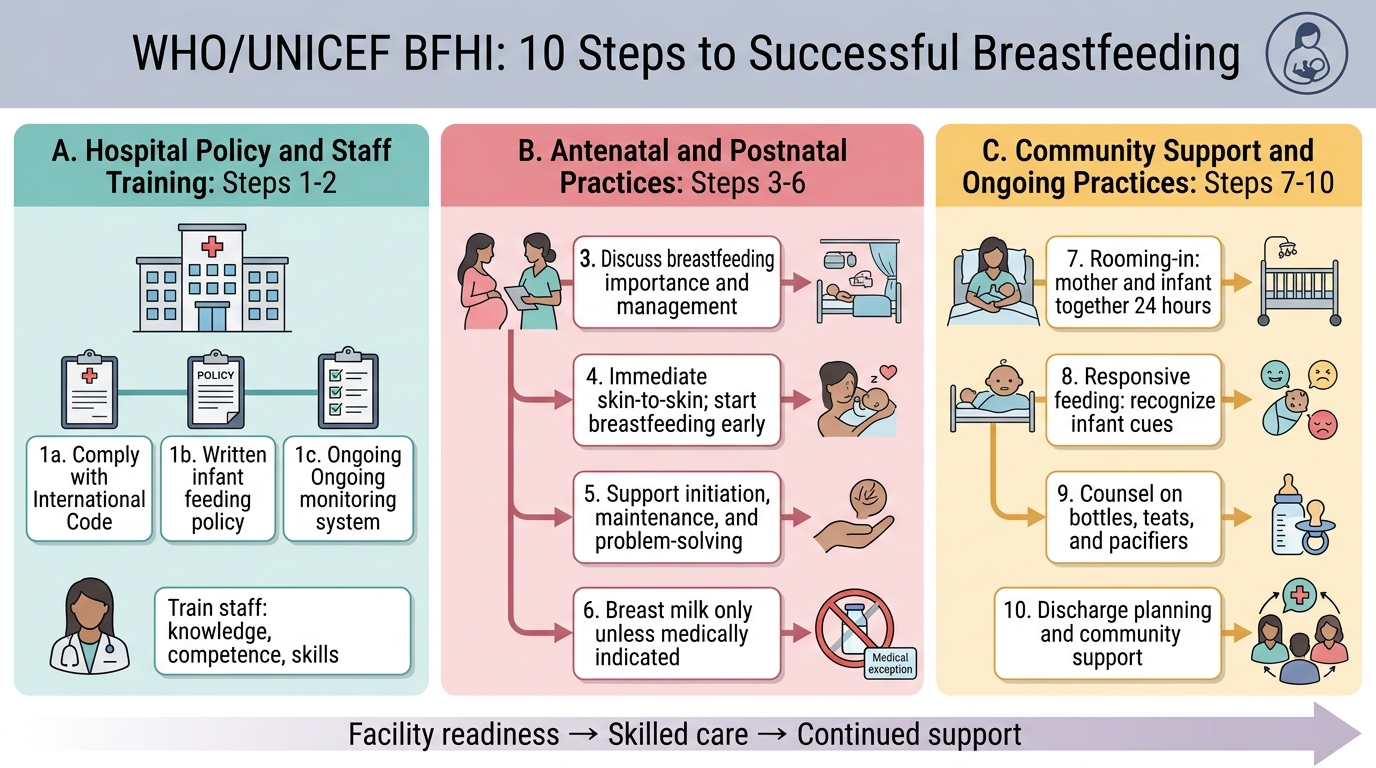
The 2018 revised BFHI framework organises the 10 Steps into two broad domains: (a) critical management procedures (institutional policy, staff competency, antenatal education) and (b) key clinical practices (skin-to-skin, rooming-in, responsive feeding, avoiding supplementation, pacifiers, and community referral).
The 10 Steps to Successful Breastfeeding (WHO/UNICEF, revised 2018) are:
- Comply with the International Code of Marketing of Breast-milk Substitutes — refuse free/low-cost formula, feeding bottles, and teats from manufacturers.
- Have a written infant feeding policy communicated routinely to staff and parents.
- Establish ongoing monitoring and data management systems to track compliance.
- Ensure staff have sufficient knowledge, competence, and skills to support breastfeeding (through training).
- Discuss the importance and management of breastfeeding with pregnant women and their families (antenatal education).
- Facilitate immediate and uninterrupted skin-to-skin contact and support mothers to initiate breastfeeding as soon as possible after birth — ideally within the first hour.
- Support mothers to initiate and maintain breastfeeding and manage common difficulties (positioning, attachment, nipple soreness, engorgement).
- Do not provide breastfed newborns any food or fluids other than breast milk, unless medically indicated.
- Enable mothers and their infants to remain together (rooming-in) and practise responsive feeding 24 hours a day.
- Provide discharge planning including referral to community support (breastfeeding support groups, lactation consultants).
Each step has a direct physiological correlate: Step 6 (early skin-to-skin) maximises neonatal colonisation and oxytocin release in both mother and infant; Step 8 (no supplementation) prevents the 'nipple-confusion' that reduces suckling effectiveness and thereby drops prolactin; Step 9 (rooming-in) ensures on-demand feeding with frequent prolactin surges to establish galactopoiesis.
IMARK: The previous BFHI (1991) had a different numbering/grouping for some steps. The 2018 revision is the current standard. In examinations, knowing the physiological rationale for each step is more valuable than rote numbering alone.
WHO/UNICEF BFHI 10 Steps to Successful Breastfeeding