Page 11 of 28
OG21.1 | Contraceptive Methods — SDL Guide
Learning Objectives
- Classify temporary and permanent contraceptive methods by mechanism of action
- Describe indications, technique, side effects, and failure rates for COC, POP, injectable, IUCD (CuT380A and LNG-IUS), implant, and barrier methods
- Apply WHO Medical Eligibility Criteria categories to select an appropriate contraceptive for a given patient scenario
- Describe emergency contraception options including levonorgestrel, ulipristal acetate, and copper IUCD
- Describe male contraception and permanent sterilisation methods for men and women
INSTRUCTIONS
Contraception is one of the most frequently requested obstetric and gynaecological services, and one of the most clinically complex — because every patient's eligibility for a given method depends on her medical history, age, parity, breastfeeding status, and personal preference. This module equips you with the classification, mechanisms, failure rates, eligibility criteria (WHO MEC), and practical details of the full range of contraceptive methods covered by competency OG21.1.
References
- DC Dutta's Textbook of Gynaecology, 7th ed., Chap 28 (Contraception) (textbook)
- Jeffcoate's Principles of Gynaecology, 8th ed., Chap 9 (Contraception) (textbook)
- WHO Medical Eligibility Criteria for Contraceptive Use, 5th ed., 2015 (updated 2017) (guideline)
- Family Planning: A Global Handbook for Providers, WHO/CDC, 3rd ed., 2018 (guideline)
- Ministry of Health and Family Welfare — National Family Planning Programme Technical Guidelines (2019 update) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Four women attend your OPD on the same morning with contraceptive requests: (1) a 32-year-old with a history of migraine with aura who has been using COC for two years; (2) a 24-year-old who delivered 4 weeks ago and is exclusively breastfeeding; (3) a 38-year-old smoker who wants to 'switch to the pill'; (4) a 22-year-old who had unprotected intercourse 60 hours ago. All four have legitimate contraceptive needs, but none of the four can safely use a combined oral contraceptive. Can you explain why — and what to offer each instead?
WHY THIS MATTERS
India is the world's most populous country, and unintended pregnancy remains a leading driver of maternal morbidity, unsafe abortion, and child poverty. Approximately 48% of pregnancies in India are unintended. Family planning is a national priority and a core primary-health-care competency. As a graduating doctor, you will counsel patients on contraception in every clinical setting — obstetric wards, gynaecology OPD, primary health centres, and community outreach. You must know not just which methods exist, but which methods are safe for which patients, what the failure rates are, and how to counsel about side effects and the permanence of surgical methods.
RECALL
Recall from your Pharmacology and Physiology modules: the hypothalamic-pituitary-ovarian (HPO) axis drives the menstrual cycle. Gonadotrophin-releasing hormone (GnRH) from the hypothalamus stimulates LH and FSH from the pituitary; LH surge triggers ovulation. Oestrogen promotes endometrial proliferation; progesterone after ovulation causes secretory transformation and cervical mucus thickening. Spermatozoa survive in the female genital tract for up to 5 days; the ovum is viable for 12–24 hours after ovulation. These physiological facts underpin every contraceptive mechanism you will study.
The Need for Contraception: Clinical Contexts
The clinical need for contraception arises across several distinct life-phase contexts, and matching the method to the context is as important as knowing the methods themselves. A woman's age, parity, breastfeeding status, medical comorbidities, partner involvement, and contraceptive history all determine which options are appropriate for her.
Postpartum contraception is one of the highest-stakes contexts. The risk of conception returns as early as 21 days after delivery in non-breastfeeding women; in breastfeeding women, ovulation may be suppressed for months (the lactational amenorrhoea method, LAM), but this suppression is unreliable once breastfeeding is not exclusive. The postpartum IUCD (PPIUCD) — a copper IUCD inserted within 48 hours of delivery or during caesarean section — is a highly effective option. Progesterone-only methods (POP, DMPA injectable, implant) are preferred if hormonal contraception is needed postpartum in a breastfeeding woman, because they do not suppress lactation. Combined oral contraceptives are contraindicated before 6 weeks postpartum in breastfeeding women (WHO MEC 4) due to oestrogen's suppressive effect on lactation and infant exposure through breast milk.
Spacing vs limiting: A couple who want to space births by 2–3 years and then have more children need a reversible, highly effective method — typically a long-acting reversible contraceptive (LARC) such as an IUCD or implant. A couple who have completed their family need either a permanent method (tubectomy, vasectomy) or a very reliable reversible method used consistently. Counselling must distinguish between spacing and limiting goals and ensure that permanent methods are chosen only with full understanding of their irreversibility.
Contraception with medical comorbidities: Conditions such as hypertension, diabetes, migraine with aura, thromboembolic risk, and liver disease significantly restrict contraceptive options. The WHO Medical Eligibility Criteria (WHO MEC) codify these restrictions into a four-category framework. Knowing the key MEC 3 and 4 conditions for the most commonly used methods is a core clinical skill.
Mechanisms of Action Across Contraceptive Methods
Understanding contraceptive mechanisms is the conceptual foundation for selecting and counselling about contraception. Most modern methods work through more than one biological pathway simultaneously, which is why their efficacy when used correctly exceeds what any single mechanism could achieve.
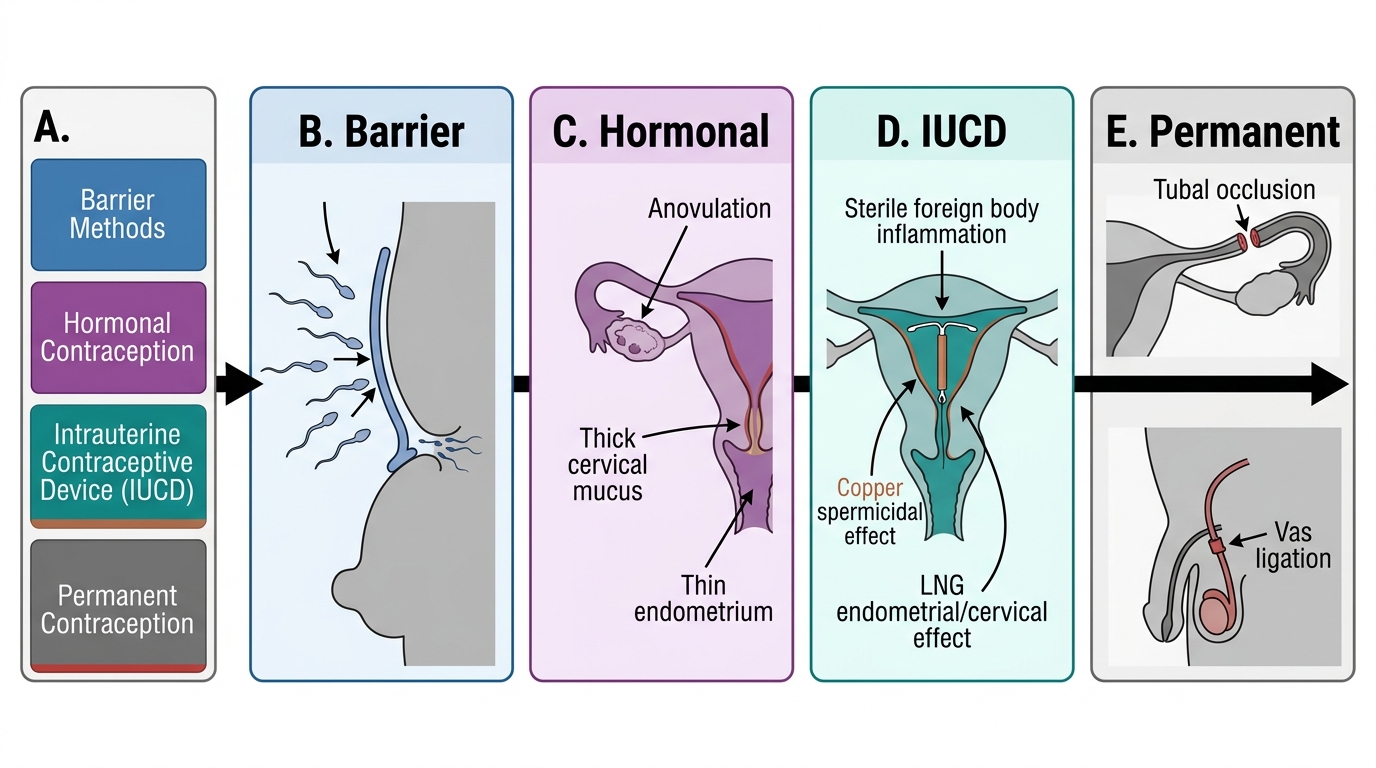
Barrier methods (male condom, female condom, diaphragm, cervical cap) act purely mechanically: they prevent sperm from entering the female genital tract or reaching the ovum. No hormone is involved; there is no effect on ovulation, endometrium, or cervical mucus. Spermicides (nonoxynol-9) kill or immobilise sperm by disrupting the sperm cell membrane; they are used as adjuncts to barrier methods, not as stand-alone contraceptives, due to a failure rate of approximately 18–28 per 100 woman-years with typical use.
Hormonal methods work through one or more of three pathways: (a) Anovulation — oestrogen in combined pills suppresses the LH surge, preventing ovulation; progestogens in high enough doses (DMPA, implant, combined pills) also suppress ovulation. (b) Cervical mucus thickening — progestogens convert cervical mucus from the thin, stretchable (spinnbarkeit) mid-cycle type to the thick, impenetrable post-ovulatory type, blocking sperm penetration. (c) Endometrial thinning — progestogens suppress endometrial proliferation, producing an atrophic endometrium that cannot support implantation.
Copper IUCDs (CuT380A) work primarily through a foreign-body reaction — the copper and the plastic frame trigger an intense local inflammatory response in the uterine cavity, producing a spermicidal, leukocytic environment that prevents fertilisation. Copper ions are also directly spermicidal — they impair sperm motility and viability. There is no anovulatory effect; ovulation is normal. The LNG-IUS (levonorgestrel intrauterine system) combines the foreign-body effect with potent local progestogenic effects: extreme endometrial atrophy, profound cervical mucus thickening, and partial (not complete) ovulation suppression in some cycles.
Permanent methods — tubectomy and vasectomy — work by physically blocking the transport of gametes: tubal occlusion prevents the ovum from reaching the sperm in the ampullary region of the tube; vas deferens occlusion prevents sperm from reaching the ejaculate.
Classification of Contraceptive Mechanisms
Patient Selection: WHO MEC Categories and Failure Rates
The WHO Medical Eligibility Criteria for Contraceptive Use (WHO MEC, 5th edition 2015) is the international standard framework for assessing whether a contraceptive method is safe for a woman with a given medical condition or characteristic. Every practitioner advising on contraception must know this framework, because it represents a systematically reviewed, evidence-based synthesis that resolves the clinical dilemma at the heart of contraceptive prescribing: when a woman with a medical condition wants contraception, how do you weigh the risk of the method against the risk of an unintended pregnancy? The MEC's four-tier scale was specifically designed to express this balance, making it more nuanced than a simple 'safe or not safe' binary. The framework is updated periodically as new evidence emerges, and the 2015/2017 version is the standard currently used in India's National Family Planning Programme guidance. Understanding the MEC categories for the most commonly prescribed methods — particularly COC, POP, DMPA, and IUCDs — is a core clinical competency for all postgraduate and final-year trainees.
WHO MEC categories:
- Category 1: No restriction — the method can be used without reservation.
- Category 2: Advantages generally outweigh risks — the method can generally be used, with close follow-up.
- Category 3: Risks generally outweigh advantages — the method is usually not recommended unless other more suitable methods are unavailable or unacceptable.
- Category 4: Unacceptable health risk — the method is contraindicated.
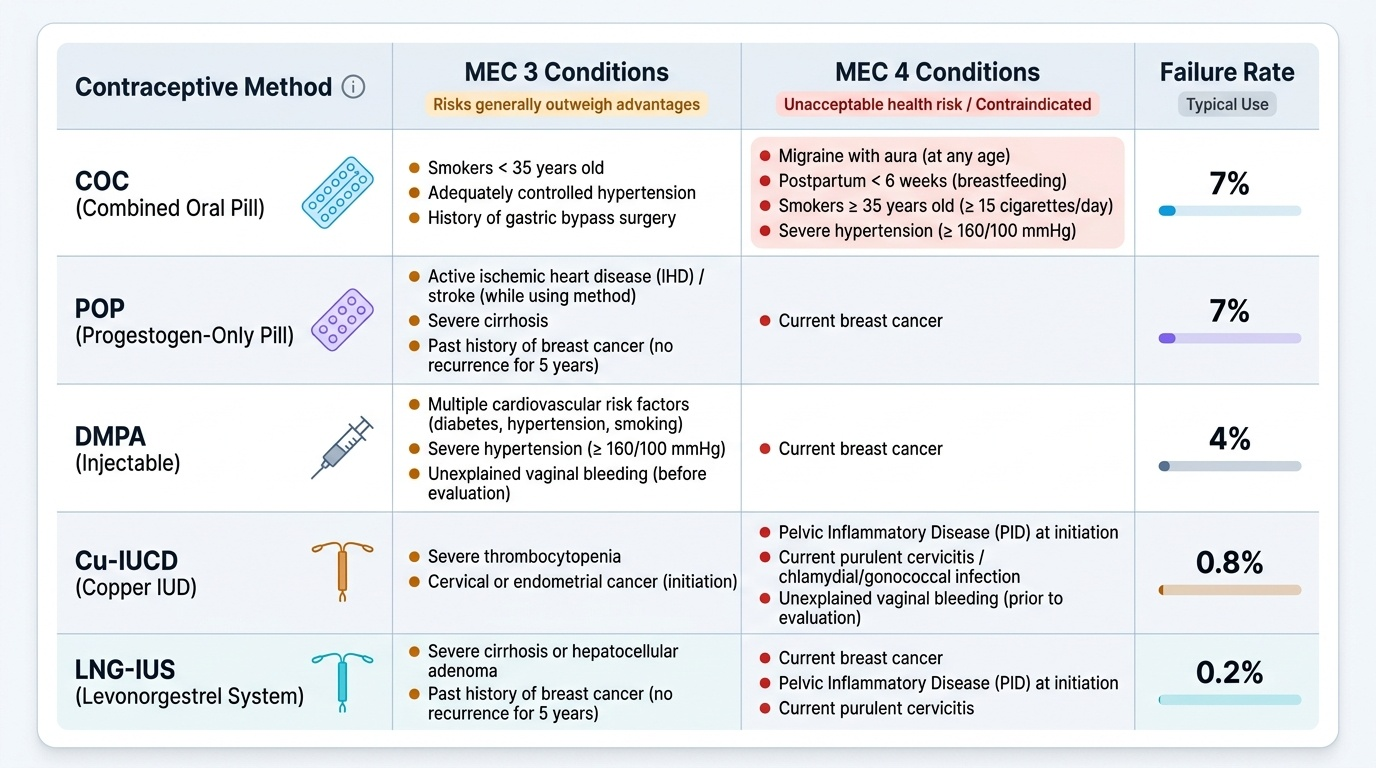
Key MEC 3/4 conditions for Combined Oral Contraceptives (COC):
- MEC 4 (contraindicated): Migraine with aura at any age (stroke risk — oestrogen increases coagulability); breastfeeding <6 weeks postpartum (suppresses lactation, oestrogen exposure to infant); smokers ≥35 years with ≥15 cigarettes/day; history of thromboembolic disease; current ischaemic heart disease; multiple cardiovascular risk factors; liver disease with impaired function.
- MEC 3 (usually not recommended): Breastfeeding 6 weeks–6 months postpartum; migraine without aura (past or current); smokers ≥35 years <15 cigarettes/day; adequately controlled hypertension; history of gestational hypertension.
Key conditions for IUCD:
- Copper IUCD MEC 4: Unexplained uterine bleeding; current cervical or endometrial cancer; distorted uterine cavity; Wilson's disease (copper IUCD); current pelvic inflammatory disease (PID) or puerperal sepsis.
- LNG-IUS MEC 4: Same structural/cancer conditions; also past breast cancer (current or within 5 years — progestogenic effect).
Failure rates represent the probability of pregnancy during the first year of use. Two measures are standard: perfect use (the theoretical method failure rate) and typical use (the population-average rate accounting for human error). The gap between perfect and typical use is the measure of how much technique matters.
| Method | Perfect use (per 100 wy) | Typical use (per 100 wy) |
|---|---|---|
| Male condom | 2 | 13–18 |
| COC | <1 | 7–9 |
| POP | 0.3 | 8 |
| DMPA injectable | 0.2 | 4–6 |
| Implant | 0.05 | 0.05 |
| CuT380A IUCD | 0.6–0.8 | 0.6–0.8 |
| LNG-IUS | 0.2 | 0.2 |
| Tubectomy | 0.1–0.5 | 0.1–0.5 |
| Vasectomy | 0.1 | 0.15 |
Provided image
SELF-CHECK
A 36-year-old woman who smokes 20 cigarettes per day requests COC. Her blood pressure is 130/85 mmHg. Under WHO MEC, which category applies to COC in this case?
A. WHO MEC 1 — no restriction, she can use COC freely
B. WHO MEC 2 — advantages outweigh risks, use with monitoring
C. WHO MEC 3 — risks usually outweigh advantages, usually not recommended
D. WHO MEC 4 — unacceptable health risk, contraindicated
Reveal Answer
Answer: D. WHO MEC 4 — unacceptable health risk, contraindicated
A woman ≥35 years who smokes ≥15 cigarettes per day is WHO MEC 4 for COC — the oestrogen component dramatically increases arterial and venous thrombotic risk in the context of age, smoking, and mild hypertension. This is an absolute contraindication. She should be offered a progestogen-only method (POP, implant, DMPA) or an IUCD, none of which carry the same thromboembolic risk from oestrogen.