Page 12 of 28
OG21.1 | Contraceptive Methods — SDL Guide (Part 2)
Temporary Methods: Barrier and Hormonal
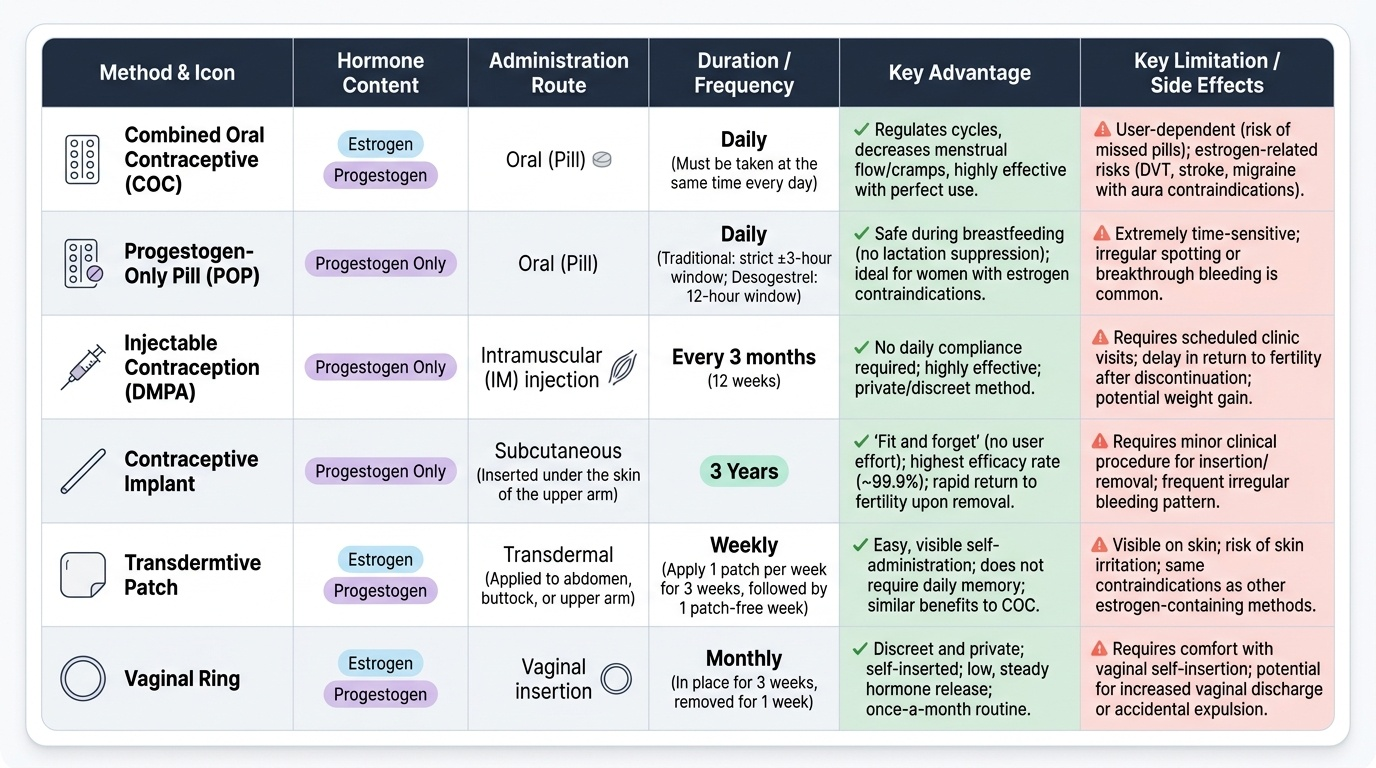
Temporary contraceptive methods are reversible — fertility returns after discontinuation. They range in efficacy from the highly effective (implant, IUCD) to the moderate (injectable, COC, POP) to the user-dependent (condom, diaphragm). Hormonal methods require ongoing adherence or a scheduled return visit, whereas long-acting methods (IUCD, implant) require no daily effort and have failure rates approaching those of surgical sterilisation.
Male condom: The only contraceptive that also provides protection against sexually transmitted infections (STIs) including HIV. Perfect use failure rate 2 per 100 wy; typical use 13–18 per 100 wy. Counselling points: correct application before any genital contact, storage away from heat, checking expiry date, use of water-based lubricant with latex condoms.
Combined Oral Contraceptive (COC): Contains a synthetic oestrogen (ethinylestradiol 20–35 mcg) and a progestogen. Mechanisms: anovulation (primary for ethinylestradiol), cervical mucus thickening, and endometrial atrophy. Typical use failure 7–9 per 100 wy; perfect use <1 per 100 wy. The gap indicates that missing pills is the main source of failure. Missed pill rule (current WHO guidance): For a 30–35 mcg EE pill — if one pill is missed (<24 h late), take it as soon as remembered and take the next at the usual time; additional contraception is not needed. If two or more pills are missed (>48 h late) — take the last missed pill immediately, discard the rest, use additional contraception for 7 days. Key side effects: nausea, breakthrough bleeding (early cycles), breast tenderness, headache, mood change. Rare serious risks: DVT, stroke, hepatic adenoma — risk substantially amplified by smoking, age ≥35, migraine with aura.
Progestogen-Only Pill (POP): Contains only a progestogen (norethisterone, desogestrel). Primary mechanism: cervical mucus thickening (all POPs) plus anovulation (desogestrel 75 mcg — consistent anovulation). Ideal for breastfeeding women (no oestrogen → no lactation suppression), women with oestrogen contraindications (migraine with aura, hypertension, thrombosis risk). The traditional POP requires a ±3-hour window for pill-taking; desogestrel POP (Cerazette) has a 12-hour window. Perfect use failure 0.3 per 100 wy.
Injectable contraception (DMPA): Depot medroxyprogesterone acetate 150 mg IM every 3 months (Depo-Provera). Highly effective (failure 0.2 per 100 wy perfect use). Mechanism: anovulation + cervical mucus thickening. Advantages: no daily pill, highly discreet, amenorrhoea in many women (useful for those with anaemia from heavy periods). Disadvantages: delayed return of fertility (12–18 months after last injection), no immediate reversibility if side effects occur, bone mineral density reduction with prolonged use (reversible), weight gain.
Subdermal implant (Implanon/Nexplanon): A single 4 cm rod containing etonogestrel, inserted subdermally in the upper arm under local anaesthesia. Effective for 3 years. Lowest failure rate of any reversible method (0.05 per 100 wy). Mechanism: anovulation + cervical mucus thickening. Side effects: irregular bleeding (the main reason for removal), no heavy periods. Advantages: long-acting, highly discreet, not coitus-dependent.
Provided image
SELF-CHECK
A 28-year-old woman delivered 5 weeks ago and is exclusively breastfeeding. She wants to start hormonal contraception. Which of the following is most appropriate?
A. Combined oral contraceptive (COC) — low-dose oestrogen will not affect milk
B. Desogestrel progestogen-only pill (POP) — safe in breastfeeding, no oestrogen
C. Wait 6 months before starting any hormonal method
D. DMPA injectable — but warn her that it suppresses lactation
Reveal Answer
Answer: B. Desogestrel progestogen-only pill (POP) — safe in breastfeeding, no oestrogen
At 5 weeks postpartum while breastfeeding, COC is WHO MEC 4 (contraindicated) — oestrogen inhibits prolactin-driven lactation and exposes the infant to oestrogen via breast milk. DMPA is WHO MEC 2 at 5 weeks postpartum and breastfeeding (generally useable from 6 weeks). The desogestrel POP is WHO MEC 2 from birth in a breastfeeding woman and is the most appropriate immediate option — progestogen-only, no effect on lactation, high efficacy, 12-hour pill window.
Intrauterine Devices, Emergency Contraception, and Male Contraception
Intrauterine devices and emergency contraception represent two of the most impactful modalities in modern contraceptive practice — IUCDs because they offer long-acting, highly effective reversible contraception that removes the human-error element entirely; emergency contraception because it provides a second-chance option after unprotected intercourse, contraceptive failure, or sexual assault.
Copper IUCD (CuT380A): A T-shaped polyethylene frame wound with copper wire. Effective for 10 years. Mechanism: copper-mediated spermicidal inflammation (foreign body reaction + copper ions). Failure rate 0.6–0.8 per 100 wy — among the most effective reversible methods. Advantages: highly effective, long-acting, non-hormonal (suitable for women who cannot use hormones), reversible (fertility returns promptly after removal), can be used as emergency contraception if inserted within 5 days of unprotected intercourse. Disadvantages: heavier and more painful menstruation (reduced after 3–6 cycles), insertion discomfort, risk of expulsion (3–5% in first year), increased risk of PID in women with multiple sexual partners (from insertion-related ascending infection, not inherent to the device).
LNG-IUS (Mirena 52 mg levonorgestrel): Effective for 5 years. Releases 20 mcg/day of levonorgestrel locally into the uterine cavity. Mechanism: extreme endometrial atrophy + profound cervical mucus thickening + partial anovulation in some cycles. Failure rate 0.2 per 100 wy. Advantages: amenorrhoea or very light periods in most women after 3–6 months (makes it therapeutic for heavy menstrual bleeding and dysmenorrhoea), very high efficacy, systemic progestogen absorption is minimal. Disadvantages: irregular spotting in first 3–6 months; contraindicated in current or recent breast cancer.
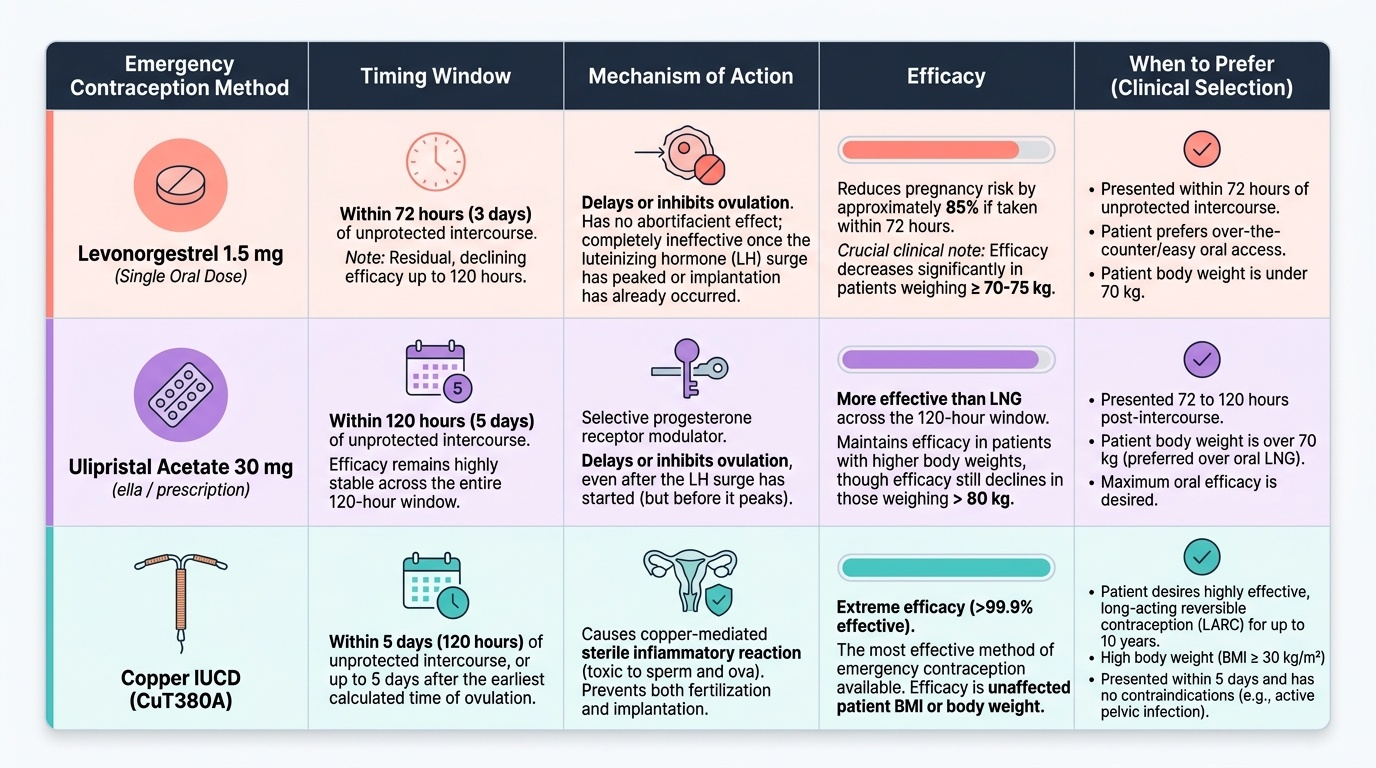
Emergency contraception (EC): EC is used within a defined time window after unprotected intercourse or contraceptive failure.
- Levonorgestrel 1.5 mg single oral dose: effective within 72 hours, with residual efficacy up to 120 hours. Reduces pregnancy risk by approximately 85% if taken within 72 h. Mechanism: delays or inhibits ovulation; no abortifacient effect once implantation has occurred. Available over-the-counter in India. Efficacy decreases significantly with body weight >70–75 kg.
- Ulipristal acetate (UPA) 30 mg (ella): effective within 120 hours; superior to levonorgestrel in the 72–120-hour window and in women with higher body weight. Selective progesterone receptor modulator — delays or inhibits ovulation.
- Copper IUCD inserted within 5 days of unprotected intercourse: the most effective EC method (>99% effective), and converts to ongoing contraception for 10 years.
Male contraception:
- Male condom: See above — also the primary STI-prevention method.
- Vasectomy: Permanent surgical sterilisation — the vas deferens is ligated, cut, or excised, preventing sperm from entering the ejaculate. The no-scalpel vasectomy (NSV) technique is standard in India's National Family Planning Programme — a small puncture rather than a scalpel incision, with lower complication rates. Failure rate: 0.1 per 100 wy. The ejaculate appears normal (sperm contribute <5% of volume); no effect on testosterone or sexual function. Semen analysis at 3 months post-procedure confirms azoospermia. Reversal (vasovasostomy) has a success rate of 40–90% depending on time since vasectomy — counsel this as effectively permanent.
- Experimental male hormonal methods: Testosterone-based injectable methods and combination regimens are under development but are not approved for clinical use in India.
Provided image
SELF-CHECK
A 30-year-old woman had unprotected intercourse 90 hours ago and requests emergency contraception. Which of the following is the best choice?
A. Levonorgestrel 1.5 mg — she is within the 72-hour window
B. Ulipristal acetate 30 mg — she is within the 120-hour window and LNG efficacy declines after 72 h
C. Wait — nothing is effective beyond 72 hours
D. Combined oral contraceptives in the Yuzpe regimen — safer than newer methods
Reveal Answer
Answer: B. Ulipristal acetate 30 mg — she is within the 120-hour window and LNG efficacy declines after 72 h
At 90 hours after intercourse, levonorgestrel has significantly reduced efficacy (it is most effective within 72 h and less so beyond). Ulipristal acetate (UPA) 30 mg is effective within 120 hours and is superior to LNG in the 72–120-hour window. The copper IUCD is the most effective option (>99%) and would also provide ongoing contraception. The Yuzpe regimen (high-dose COC) is no longer recommended as first-line EC due to higher side effects and lower efficacy compared with dedicated EC products.
Permanent Methods: Tubectomy and Vasectomy
Permanent contraception should be offered only after thorough counselling confirming that the couple has completed their family and understands that these methods are intended to be irreversible. Although surgical reversal is possible, its success rate decreases with time and cannot be guaranteed. Obtaining a truly informed and voluntary decision for sterilisation is therefore a critical counselling skill — and it must be a decision made free from the emotional pressure of an acute obstetric event. India has a well-documented history of coercive sterilisation programmes in the 20th century; the National Family Planning Programme guidelines explicitly prohibit incentives to healthcare providers for achieving sterilisation targets, and require that consent be obtained well before any delivery or surgical event where sterilisation might be offered. As a clinician, you must ensure that permanent sterilisation is chosen by the patient, not pressured by institutional incentives, family members, or provider assumptions about family size. This ethical obligation is as important as the technical surgical knowledge.
Female sterilisation (tubectomy): Tubal occlusion prevents the ovum from meeting sperm in the ampullary portion of the fallopian tube. Several techniques are used.
- Interval tubectomy (performed outside the puerperium or pregnancy): Laparoscopic approach — Filshie clips (titanium with silicone liner, standard modern technique) or fallope rings (bands) applied to the isthmic portion of the tube. Minilaparotomy (2–3 cm suprapubic incision) — Pomeroy technique (a loop of tube is ligated and excised; simple, widely taught, failure rate 0.4 per 100 wy) or Parkland technique (tubal segment resected between two ties).
- Postpartum tubectomy (PPTL): Performed within 48 hours of delivery or during caesarean section, when the fundus is high and the tube easily accessible. The modified Pomeroy technique or tubal ring is used. PPTL failure rate is slightly higher than interval tubectomy due to postpartum tubal congestion; the woman must have made the decision before delivery — post-delivery consent is not valid in the context of pain or anaesthetic influence.
- Failure rates and reversibility: Overall tubectomy failure 0.1–0.5 per 100 wy cumulative over 10 years (Filshie clips among the lowest; bilateral salpingectomy — removing the entire tube — is the most effective). Reversal (tubal reanastomosis) is possible but success drops with time: >80% within 1 year, <40% after 10 years.
Vasectomy (see also male contraception above): The no-scalpel technique is preferred in the national programme. Performed under local anaesthesia as an outpatient. Complications are uncommon: haematoma (most common), sperm granuloma, epididymo-orchitis. Failure rate 0.1 per 100 wy; not immediately effective — a post-vasectomy semen analysis at 3 months must confirm azoospermia before unprotected intercourse is safe. Vasectomy is simpler, safer, cheaper, and more effective per procedure than tubectomy — counselling should present vasectomy as an equally valid option when the man is willing, to avoid placing the burden of permanent contraception entirely on the woman.
SELF-CHECK
A couple request surgical sterilisation. The woman is 32 years old with three children; the husband is 35. Both are healthy. Which of the following is most accurate about vasectomy vs tubectomy in this case?
A. Tubectomy is always preferred because it eliminates the possibility of method failure through non-compliance
B. Vasectomy is simpler, equally effective, and carries lower surgical risk than tubectomy — it should be offered as a co-equal option
C. Vasectomy is unreliable until confirmed by semen analysis, so tubectomy is the safer option for immediate effect
D. Vasectomy is contraindicated in India under the National Family Planning Programme
Reveal Answer
Answer: B. Vasectomy is simpler, equally effective, and carries lower surgical risk than tubectomy — it should be offered as a co-equal option
Vasectomy is simpler (outpatient, local anaesthesia), as effective as tubectomy (failure rate 0.1 per 100 wy), and carries lower anaesthetic and surgical risk than tubectomy under general anaesthesia with laparoscopy or minilaparotomy. It is actively promoted in India's National Family Planning Programme via no-scalpel vasectomy. Counselling should present it as a co-equal option — gender equity in accepting the burden of surgical contraception. The requirement for 3-month semen analysis is a temporary limitation, not a contraindication.
CLINICAL PEARL
The three most commonly asked WHO MEC 4 conditions for COC in exams and OSCEs are: (1) migraine WITH aura — oestrogen triples ischaemic stroke risk in this group; (2) breastfeeding less than 6 weeks postpartum — oestrogen inhibits prolactin and exposes the neonate; (3) smokers aged 35 or more with heavy smoking — arterial thrombosis risk is multiplicative. In clinical practice, always ask about migraine aura (not just headache), breastfeeding status and duration, and smoking habit and quantity before prescribing COC. A woman who ticks any of these boxes must not receive combined oestrogen-progestogen contraception — offer a progestogen-only method or a copper IUCD instead.
Self-Assessment
You have covered the full scope of OG21.1 — classification, mechanisms, WHO MEC categories, failure rates, and clinical application of temporary and permanent contraceptive methods including male contraception and emergency contraception. The questions below test integration of these elements in clinical scenarios. Before answering each question, identify the key clinical constraint (WHO MEC condition, breastfeeding status, gestational timing, or patient preference) that drives the method selection. This structured approach reflects the way an experienced clinician approaches contraceptive counselling, and it is the reasoning process that earns marks in clinical viva examinations. Good contraceptive practice is not just knowing the options — it is matching the safest, most acceptable, and most effective option to the individual patient, documented with the reasoning. Each question is structured to test exactly this clinical reasoning, not the memorisation of facts in isolation.
- Classify contraceptive methods into barrier, hormonal, and intrauterine categories. For hormonal methods, give one example of each subtype (oral combined, oral progestogen-only, injectable, implant).
- A 32-year-old woman with a history of deep vein thrombosis requests contraception. She is not breastfeeding and delivered 3 months ago. What is the most appropriate method?
- Explain the difference in mechanism between the copper IUCD (CuT380A) and the LNG-IUS.
- A couple present for contraceptive counselling 2 years after the birth of their third child. They are certain they do not want more children. Describe the counselling you would provide for permanent sterilisation, including the key points about reversibility and vasectomy as an option.
- What are the three WHO MEC 4 contraindications to COC that every obstetrician must know?
Answers:
1. Barrier: male condom, female condom, diaphragm. Hormonal: COC (e.g., Mala-N — ethinylestradiol + norgestrel); POP (desogestrel 75 mcg — Cerazette); injectable (DMPA 150 mg IM every 3 months); implant (etonogestrel single rod, effective 3 years).
2. DVT history is WHO MEC 4 for COC (oestrogen dramatically amplifies VTE risk). The copper IUCD CuT380A is the safest and most effective option — non-hormonal, no VTE risk, long-acting, easily reversible. If she prefers hormonal, progestogen-only implant or POP is MEC 2 in past DVT (some risk but acceptable if no current anticoagulation).
3. Copper IUCD (CuT380A): non-hormonal; works by copper-mediated spermicidal inflammation (foreign body reaction + copper ions); does not suppress ovulation; effective 10 years. LNG-IUS: delivers levonorgestrel locally (20 mcg/day) causing extreme endometrial atrophy and thick cervical mucus; partial anovulation in some cycles; amenorrhoea in majority after 3–6 months; effective 5 years.
4. Counselling for permanent sterilisation: both options (tubectomy and vasectomy) are highly effective (failure rate 0.1–0.5 per 100 wy) and should be considered permanent. Reversal is possible but success rates decline with time and cannot be guaranteed — offer this option only to couples who are certain. Vasectomy is simpler, safer (outpatient under local anaesthesia), equally effective, and should be actively discussed as a valid option to avoid placing the full burden on the woman. A voluntary, informed consent process — separate from any acute obstetric or psychiatric event — must be documented.
5. Three WHO MEC 4 contraindications to COC: (1) Migraine with aura (at any age — stroke risk); (2) Breastfeeding less than 6 weeks postpartum (oestrogen suppresses lactation + infant exposure); (3) Smokers aged ≥35 years with heavy smoking (≥15 cigarettes/day — multiplicative arterial thrombosis risk with age and oestrogen).