Page 16 of 28
OG21.2 | IUCD Insertion and Removal — SDL Guide (Part 3)
Self-Assessment: IUCD Skills
The questions below are designed to consolidate your understanding across all six sections of this SDL and to prepare you for the simulation OSCE. They span eligibility decision-making, technique steps, and complication recognition — the three domains that are assessed in clinical practice and in written examinations. For each question, work out the answer independently, reason through the underlying anatomical or clinical principle, and only then check your notes. If you cannot answer a question, return to the relevant section before your simulation session rather than leaving a gap. Questions 3 and 4 are particularly important because they describe emergencies that must be recognised and acted on immediately; a learner who cannot recall the immediate action for suspected perforation or ectopic pregnancy in an IUCD user is not yet ready for supervised clinical exposure.
- You sound a uterus and the sound reaches 5.5 cm. What does this mean for IUCD insertion and what would you do?
- A woman has her CuT 380A inserted during an interval visit. Four months later she presents with heavy periods that are twice her usual flow. The device is in situ on ultrasound. What is your management?
- During IUCD insertion you feel a sudden loss of resistance and the inserter has passed to 11 cm. What has likely occurred and what is your immediate action?
- A woman with a copper IUCD of 3 years presents with 8 weeks of amenorrhoea. Her urine pregnancy test is positive. What is the most important immediate investigation and why?
- A breastfeeding woman 6 weeks postpartum requests contraception. She has a history of deep vein thrombosis. What is the role of copper IUCD and LNG-IUS in her management, and what are the relevant WHO MEC categories?
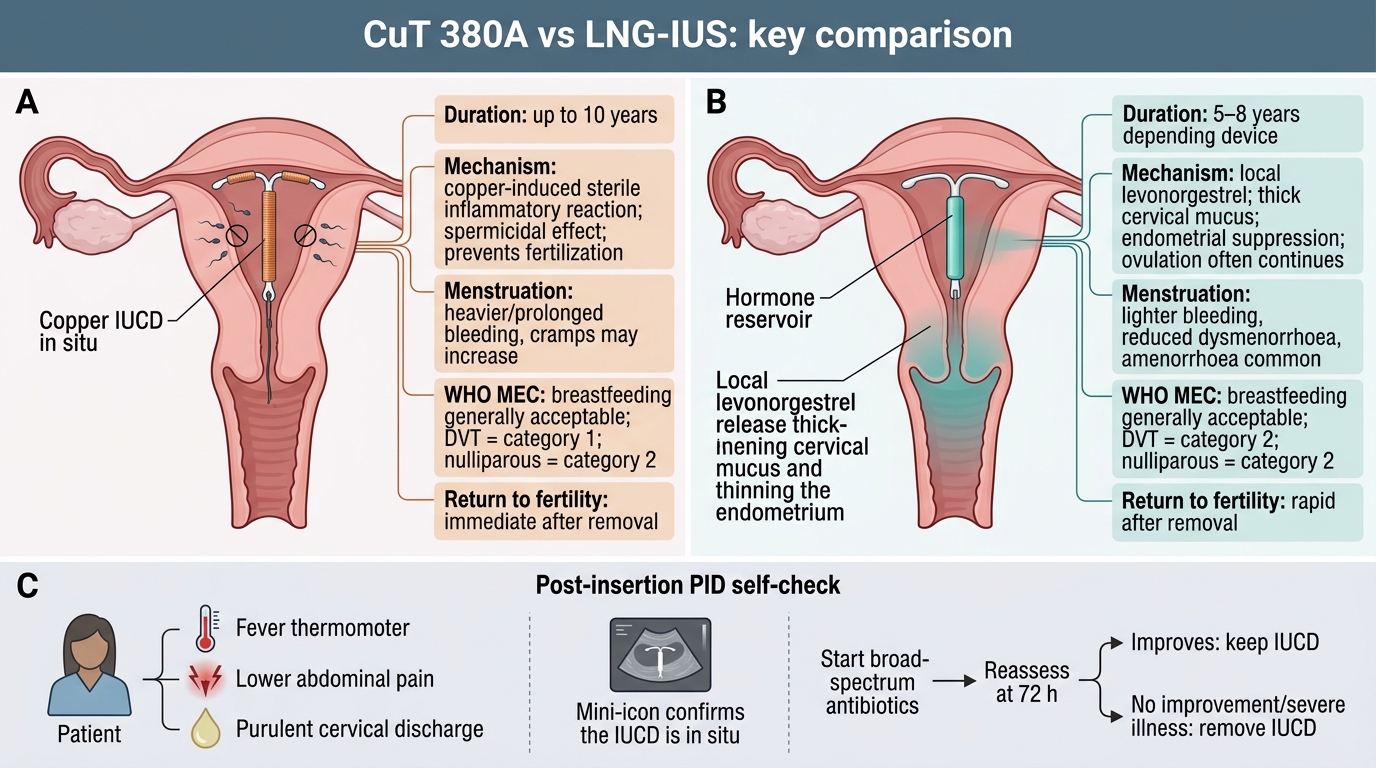
CuT 380A vs LNG-IUS: Summary Comparison
SELF-CHECK
A 25-year-old nulliparous woman had a CuT 380A inserted 3 days ago. She now presents with lower abdominal pain, fever of 38.8°C, and purulent cervical discharge. The device is confirmed in situ on ultrasound. What is the most appropriate management?
A. Immediate IUCD removal followed by antibiotics
B. Antibiotics alone; defer decision on device removal to 72 hours and assess response
C. IUCD removal only; antibiotics are not indicated as they will not penetrate the endometrium
D. Reassure and review in 1 week; early post-insertion discomfort is expected
Reveal Answer
Answer: B. Antibiotics alone; defer decision on device removal to 72 hours and assess response
Guidelines (RCOG, FSRH) recommend treating IUCD-associated PID with appropriate antibiotics and NOT routinely removing the device immediately, as removal does not improve outcomes and may deny the patient effective contraception. The device should be removed only if there is no clinical improvement within 72 hours or if the patient is severely ill. Immediate fever + discharge 3 days post-insertion strongly suggests ascending infection from the insertion procedure — initiate broad-spectrum antibiotics covering Chlamydia, gonorrhoea, and anaerobes (e.g., doxycycline + metronidazole ± ceftriaxone per local protocol), review at 72 h.
CLINICAL PEARL
The most common technique error leading to early expulsion is failure to place the device at the fundus. If the device sits in the lower segment or the cervical canal, it has no contraceptive effect and will almost certainly be expelled within days. The flange on the inserter is the sole objective marker that the device has reached the correct depth — set it to the sounding depth, advance until the flange touches the external os, and only then withdraw the tube. Do not release the arms before reaching fundal depth. In postpartum insertions, always confirm placement by ultrasound when feasible, as the large, soft postpartum uterus makes tactile feedback less reliable.