Page 8 of 28
OG20.3 | PC and PNDT Act — SDL Guide
Learning Objectives
- Discuss the historical and demographic context that led to the enactment of the PCPNDT Act 1994
- Describe the structure, scope, prohibited acts, and key provisions of the PC and PNDT Act 1994 and its 2003 amendment
- Enumerate the obligations of a clinician conducting prenatal diagnostic techniques under the Act, including Form F and record-keeping
- Identify offences under the Act and the applicable penalties
INSTRUCTIONS
India enacted the Pre-conception and Pre-natal Diagnostic Techniques (Prohibition of Sex Selection) Act in 1994 in direct response to evidence that prenatal diagnostic techniques were being misused to determine fetal sex and selectively terminate female pregnancies. Every doctor who performs ultrasonography, amniocentesis, or any other listed technique on a pregnant woman — in any setting — has legal obligations under this Act. This module walks you through those obligations, the structure of the Act, and how to apply it in clinical practice without inadvertently violating it.
References
- Pre-conception and Pre-natal Diagnostic Techniques (Prohibition of Sex Selection) Act 1994 and PCPNDT Rules 1996 (amended 2003 and subsequently) (guideline)
- DC Dutta's Textbook of Obstetrics, 9th ed., Appendix (PCPNDT Act) (textbook)
- Agarwal's Medicolegal Issues in Obstetrics and Gynaecology (textbook)
- Ministry of Health and Family Welfare, India — PCPNDT Implementation Guidelines (guideline)
- Reddy's The Essentials of Forensic Medicine and Toxicology, 35th ed. — Chapter on Medical Legislation (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
An ultrasonologist at a private clinic in a district with a low sex ratio is asked by a couple during their 20-week anomaly scan: 'Doctor, please tell us if it is a boy or a girl — we just want to be prepared.' The couple seem harmless. No FIR will be filed. No one is watching. What is the legal status of this request? What are the consequences if you comply? And what precisely is the correct response — and how do you frame it? This scenario is not hypothetical; it is the most common PCPNDT violation encountered in practice.
WHY THIS MATTERS
Every doctor who uses ultrasonography, performs amniocentesis, or conducts any of the listed prenatal diagnostic techniques on a pregnant woman is subject to the PCPNDT Act — regardless of whether the technique is being used for sex determination. The Act requires registration of the facility, completion of Form F before each procedure, maintenance of records, and absolute prohibition on communicating foetal sex. Violation makes the clinician criminally liable. For the final-year MBBS student, this Act appears in viva voce, written papers, and clinical assessments — and in professional life, ignorance of it is not a defence.
RECALL
Recall from your Community Medicine and Forensic Medicine modules: India's sex ratio at birth (SRB) is the number of female births per 1,000 male births. A biologically normal SRB is approximately 950–985. Many Indian states showed SRBs well below 900 in the 1990s-2000s, particularly in Punjab, Haryana, and parts of Rajasthan — a pattern consistent with systematic female-selective abortion. The Missing Women concept, introduced by Nobel Laureate Amartya Sen in 1990, estimated that 100 million women were 'missing' from South Asia due to sex-selective practices. Ultrasonography became widely affordable in India in the late 1980s, coinciding with the acceleration of SRB distortion.
The Problem: Sex Selection and Its Consequences
Sex selection refers to practices intended to increase or decrease the probability of conceiving or continuing a pregnancy of a particular sex. In the Indian context, the operative concern is daughter aversion driven by social, economic, and cultural factors including the practice of dowry, son preference for agricultural labour and family lineage, and the perceived economic burden of raising daughters in communities without strong inheritance rights for women. The result has been systematic elimination of female foetuses, a practice that accelerated dramatically with the spread of affordable diagnostic ultrasonography in the 1980s.
The demographic consequences are profound. India's 2011 Census recorded a child sex ratio (0–6 years) of 914 girls per 1,000 boys — the lowest since independence. Districts in Haryana, Punjab, Rajasthan, and parts of Gujarat recorded CSRs below 880 — indicating the disappearance of thousands of female births per year in each district. The consequences extend beyond the immediate tragedy of female-selective abortion: skewed sex ratios correlate with increased trafficking of women across state lines, increased rates of marriage by abduction, and social instability in regions where marriageable women are scarce.
For the clinician, the relevance is direct: the stethoscope, the ultrasound probe, and the amniocentesis needle can become instruments of sex selection if the practitioner does not understand and comply with the law. The PC and PNDT Act 1994 is India's legislative response, and it places specific obligations on every facility and clinician performing prenatal diagnosis — not only on those who actually communicate foetal sex, but also on those who fail to register, maintain records, or fill Form F correctly.
PC and PNDT Act: Structure and Key Provisions
The PC and PNDT Act 1994: Structure and Key Provisions
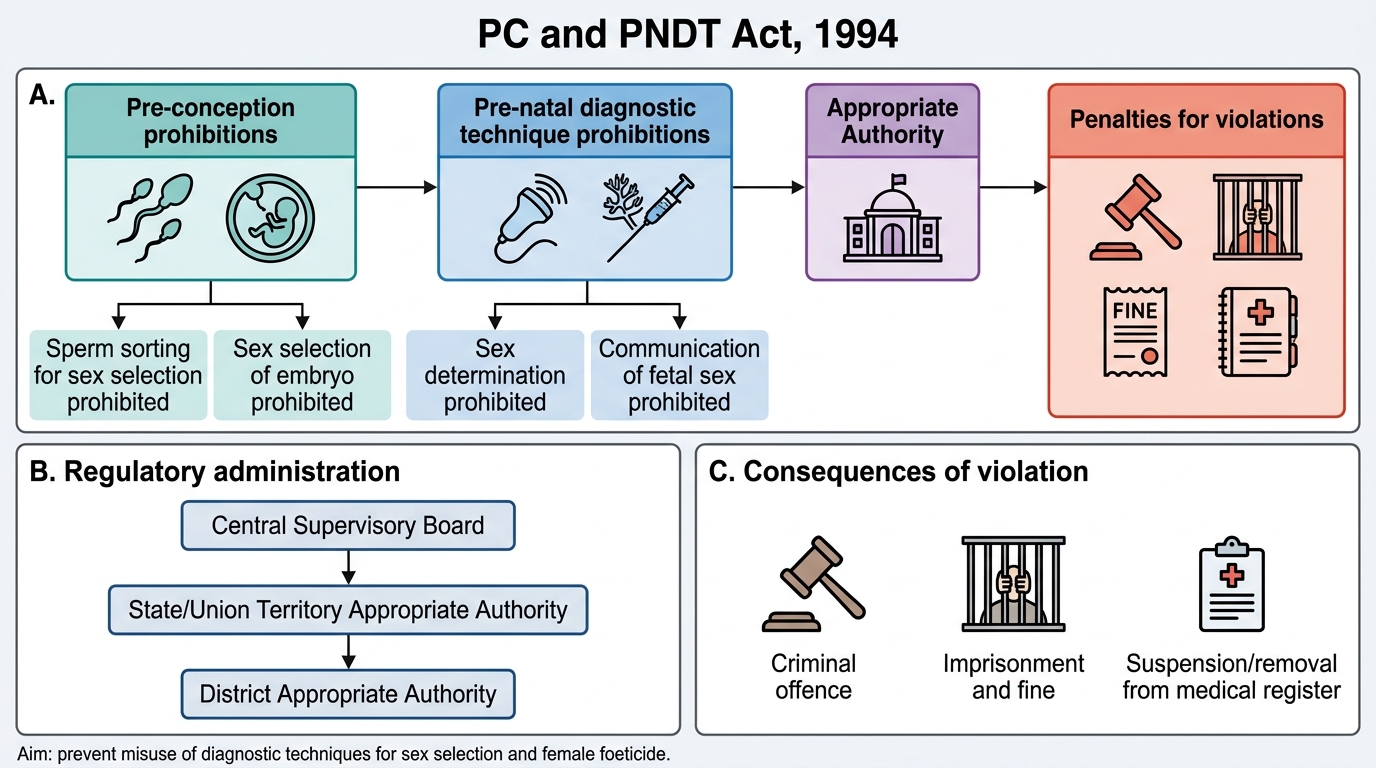
The Pre-conception and Pre-natal Diagnostic Techniques (Prohibition of Sex Selection) Act, 1994 (commonly abbreviated PCPNDT Act) was enacted to regulate pre-natal diagnostic techniques with a view to prevent their misuse for the purpose of pre-natal sex determination, and ultimately to prevent female foeticide. It was substantially amended in 2003 — the most consequential revision — which expanded the Act's scope from post-conception techniques only to include pre-conception sex selection as well, reflecting the policy-maker's recognition that selective sperm sorting and embryo selection were emerging as new frontiers for sex bias. This amendment also renamed the statute from the original PNDT Act (1994) to the current PC & PNDT Act (Pre-conception and Pre-natal Diagnostic Techniques). The Act is administered through a hierarchy of Appropriate Authorities — Central, State, and District — and violation of its provisions is a criminal offence carrying imprisonment and mandatory removal from the medical register. Every clinician who touches a pregnant woman with an ultrasound probe or a biopsy needle is within the Act's jurisdiction.
The Act covers two broad categories of regulated activity and their associated prohibitions.
Pre-conception techniques (added by 2003 amendment):
- Prohibited acts: Conducting pre-conception sex selection by any method including separation of X- or Y-bearing spermatozoa; use of preimplantation genetic diagnosis (PGD) for sex selection (unless for sex-linked disease).
- A genetic counselling centre, genetic laboratory, or genetic clinic offering these techniques must be registered.
Pre-natal diagnostic techniques:
- Defined as: ultrasonography (including transvaginal), amniocentesis, chorionic villus sampling (CVS), foetoscopy, maternal serum markers, and analysis of any blood or products of conception.
- Lawful indication for prenatal diagnosis: (a) maternal age above 35; (b) two or more previous spontaneous abortions or foetal loss; (c) previous child with chromosomal or metabolic abnormality; (d) family history of mental retardation; (e) abnormal maternal serum markers; (f) exposure to drugs, radiation, infection, chemicals; and others specified.
- Key point: The technique itself is lawful for these indications. What is prohibited is using the result — or the technique — to determine the sex of the foetus for sex-selection purposes.
What is prohibited under the Act:
1. Sex determination — conducting any pre-natal diagnostic technique to determine the sex of the foetus.
2. Communication of sex — communicating the sex of the foetus in any form (verbal, written, sign language, model, diagram) to the pregnant woman, her relatives, or any other person.
3. Advertisement — advertising, in any form, any sex-determination services.
4. Sex selection pre-conception — using any pre-conception technique to select the sex of the embryo or gamete.
Critically, the prohibition on communicating foetal sex applies even when the determination was made incidentally during a lawful anomaly scan. The doctor who notices the sex during a 20-week anomaly scan must actively withhold that information — it must not be volunteered, and must be refused if asked.
SELF-CHECK
A pregnant woman at 18 weeks requests an anomaly scan. The indication is a previous child with trisomy 21. During the scan, the sex of the foetus is incidentally observed. Which of the following is correct under the PCPNDT Act?
A. The scan is illegal because the woman did not have a valid indication
B. The scan is legal but the sex must not be communicated to the woman or anyone else
C. The sex may be disclosed only to the woman and not to her family
D. The sex may be communicated if the woman asks for it in writing
Reveal Answer
Answer: B. The scan is legal but the sex must not be communicated to the woman or anyone else
A previous child with chromosomal abnormality (trisomy 21) is a valid indication for prenatal diagnosis under the Act. The scan itself is legal. However, once foetal sex is observed (even incidentally), it must not be communicated — to anyone, in any form. The prohibition is absolute regardless of whether the woman requests the information or makes the request in writing. Only PGD for sex-linked disease (not sex selection) is an exception.
Clinician Obligations Under the Act
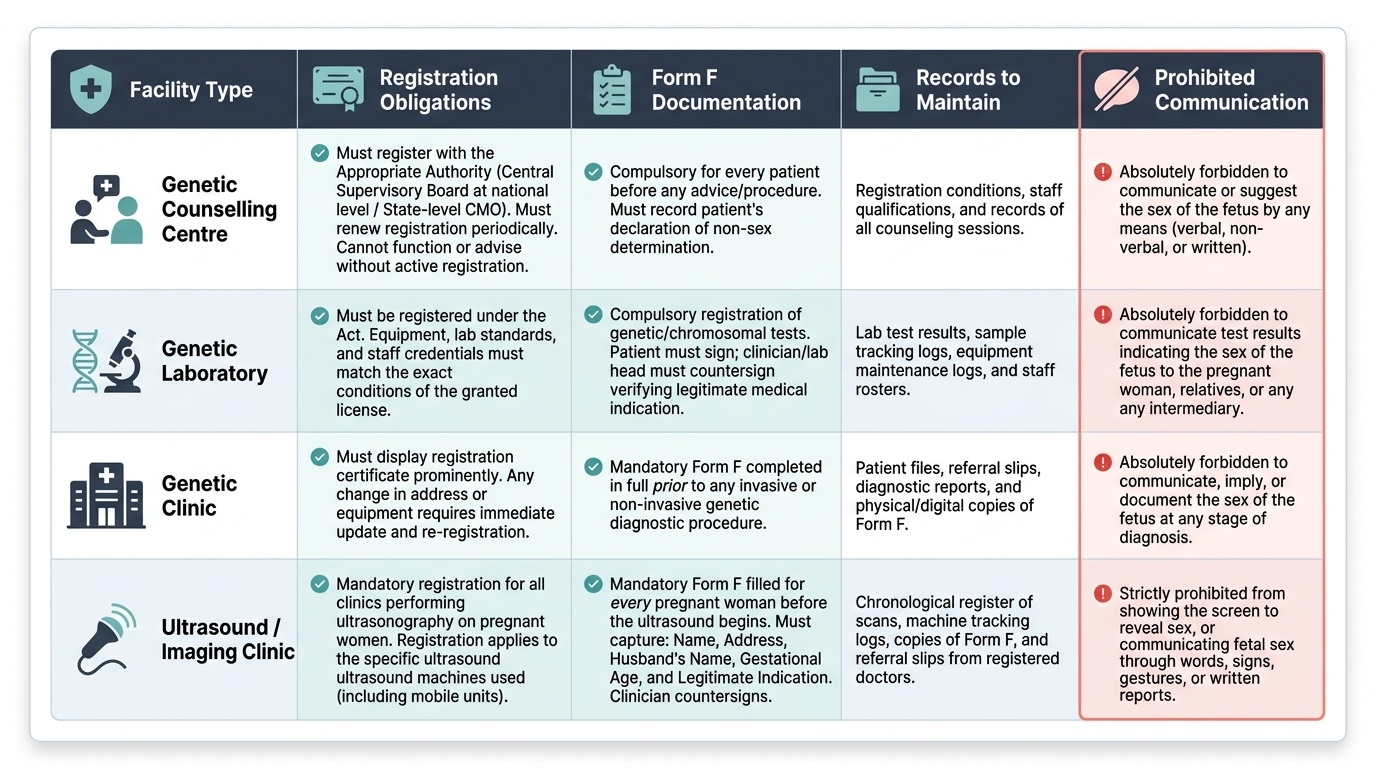
Every practitioner who performs a prenatal diagnostic technique covered by the Act — whether in a government hospital, a private clinic, or a mobile unit — is subject to specific legal obligations that are not optional and not delegable to a secretary or office manager. Failure to comply with any of these obligations is itself an offence under the Act, separate from and in addition to the prohibition on sex determination. The regulatory framework organises these obligations into three tiers: registration, documentation, and communication restrictions.
1. Registration:
No genetic counselling centre, genetic laboratory, genetic clinic, or imaging centre performing ultrasonography on pregnant women may function without registration under the Act. Registration is granted by the Appropriate Authority — the Central Supervisory Board at the national level; State-level Appropriate Authorities (usually the Chief Medical Officer) at the state level. Registration must be renewed, and the facility must maintain the conditions under which registration was granted (staffing, equipment, record systems). An unregistered facility operating any covered technique is committing an offence regardless of whether any sex determination is performed.
2. Form F (the compulsory consent/declaration form):
Form F is the single most important documentation requirement under the Act. It must be filled out for every pregnant woman before she undergoes any prenatal diagnostic procedure. Form F captures: the woman's name, address, husband's name, gestational age, indication for the procedure, and — crucially — the woman's declaration that she is not seeking the sex of the foetus. The clinician countersigns, attesting that the procedure is being performed for a legitimate indication and that the sex of the foetus has not been and will not be disclosed. Form F must be retained for a period of 2 years and must be made available to the Appropriate Authority on demand.
A practitioner who fails to maintain Form F, fills it incorrectly, or does not obtain it is guilty of a recordkeeping offence under the Act.
3. Communication restrictions:
No person conducting a prenatal diagnostic technique may communicate or cause to be communicated the sex of the foetus to the pregnant woman or her relatives or any other person in any manner whatsoever — whether verbally, in writing, by sign, gesture, or display of ultrasound images. This includes 3D/4D ultrasound images that clearly depict genitalia. Many practitioners have been prosecuted not for direct sex determination but for showing a clear image of the foetal genitalia on the screen and noting 'you can see everything is normal there.'
Provided image