Page 9 of 28
OG20.3 | PC and PNDT Act — SDL Guide (Part 2)
Offences, Penalties, and the Appropriate Authority
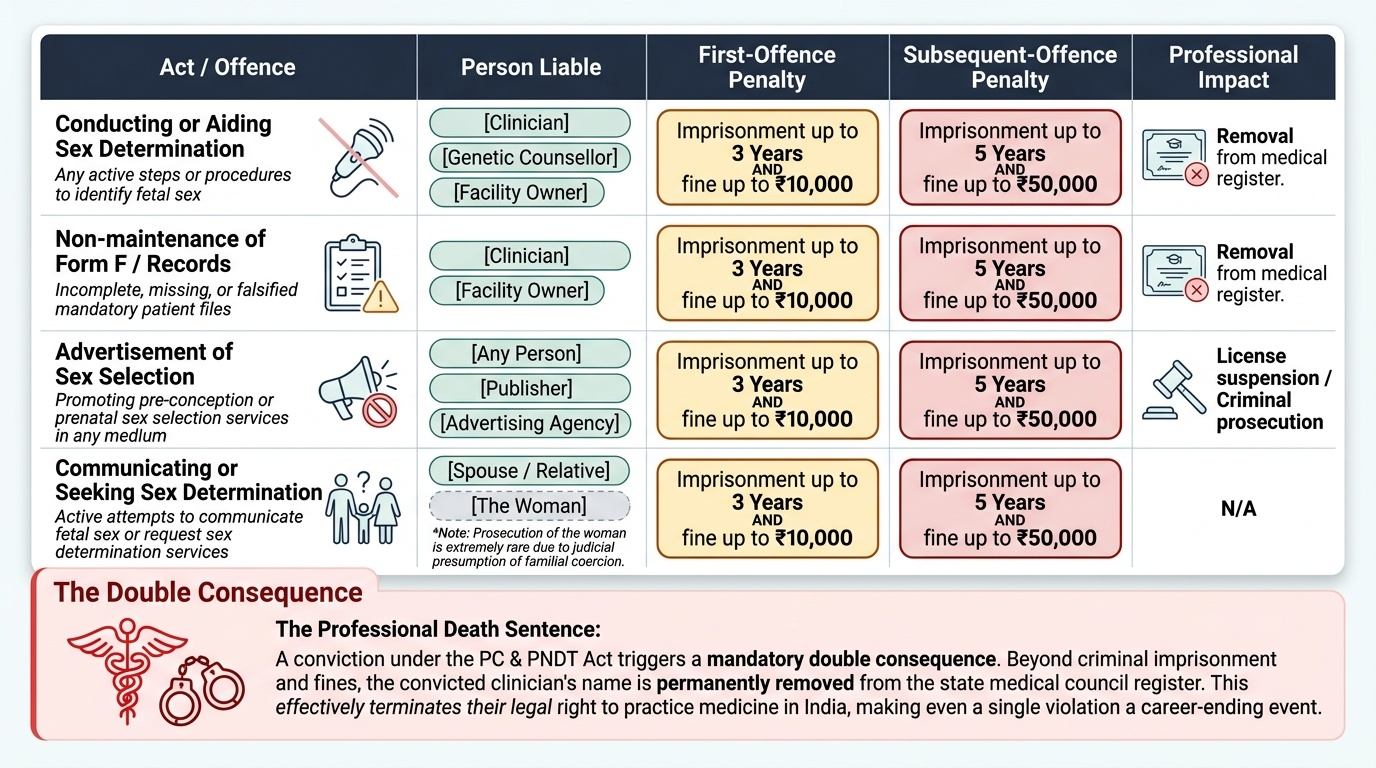
The PCPNDT Act creates a system of offences applicable to individuals and institutions, and it places enforcement responsibility with Appropriate Authorities at different levels. Understanding the offence categories and their penalties is not merely an examination requirement — it is a professional necessity, because the consequences of a PCPNDT conviction are career-ending: in addition to imprisonment and a fine, the convicted person's name is removed from the register maintained under any law in force, effectively ending their legal right to practise medicine. The Act deliberately designed this double consequence (criminal penalty plus professional deregistration) to make violation a serious risk for any clinician who might otherwise rationalise a single act of sex-disclosure as harmless. The penalties were also made proportionate: a first offence carries a lighter sentence to allow for the possibility of negligence or inadvertence, while repeat offenders face significantly heavier punishment.
The Act identifies the following as offences for which the registered person (clinician, genetic counsellor, or owner of the facility) is liable.
Principal offences and their penalties under the Act (as amended 2003):
- Conducting or aiding sex determination: First offence — imprisonment up to 3 years AND fine up to Rs. 10,000. Subsequent offence — imprisonment up to 5 years AND fine up to Rs. 50,000. The name of the convicted person is removed from the register maintained under any law for the time being in force.
- Failure to maintain Form F / records: Offence under the Act; same penalty structure.
- Advertisement of sex-selection services: Offence attracting imprisonment and fine.
- Running an unregistered facility: Offence under the Act.
- Seeking sex determination (by the woman or her relative): The Act was amended to make the woman seeking the information liable, but in practice prosecution of women is rare because the Supreme Court and various High Courts have emphasised that women are often coerced by family members.
The Appropriate Authority at the State level (typically the District Medical Officer in many states) has wide powers: inspecting facilities, seizing records, suspending or cancelling registration, filing complaints, and initiating prosecution. The Central Supervisory Board monitors policy and implementation. The State Supervisory Board oversees the State Appropriate Authority.
The Suo motu complaint provision is important: any person, including a woman's relative who has been pressured to reveal foetal sex, can bring a complaint before the Appropriate Authority. The authority is also empowered to act on its own information without waiting for a formal complaint.
Provided image
SELF-CHECK
A radiologist is prosecuted under the PCPNDT Act for failing to maintain Form F for 15 patients over 3 months. This constitutes which type of offence?
A. Not an offence — Form F is only required when sex determination is performed
B. An offence under the Act attracting up to 3 years imprisonment and fine of Rs. 10,000 for the first offence
C. A civil violation only, not a criminal offence
D. Only the owner of the facility is liable, not the radiologist personally
Reveal Answer
Answer: B. An offence under the Act attracting up to 3 years imprisonment and fine of Rs. 10,000 for the first offence
Failure to maintain Form F is an independent offence under the PCPNDT Act, not contingent on sex determination having occurred. The radiologist is personally liable (not just the institution's owner) if they conducted the procedure without Form F. The penalty for first offence is imprisonment up to 3 years AND fine up to Rs. 10,000.
Applying the Act in Clinical Practice: Scenarios
The PCPNDT Act is applied every time a covered prenatal technique is performed on a pregnant woman. The following scenarios represent the range of situations encountered in clinical practice. In each case, identify whether the proposed action is legal, what obligations apply, and how you should respond if asked to disclose foetal sex.
Scenario 1 — Routine anomaly scan:
A 25-year-old primigravida at 19 weeks attends for her Level II anomaly scan. No indication other than routine anatomy assessment. Is this scan covered by the Act? Yes — all ultrasonography on a pregnant woman is covered. Before beginning: (a) confirm registration of the facility; (b) fill Form F with the woman's details; (c) proceed with the scan; (d) document findings of anatomy, amniotic fluid, placenta in the report; (e) do not record the sex of the foetus anywhere in the report; (f) if the sex is visible, do not comment on it. If the woman asks 'What is it?', the correct response is: 'I am required by law not to disclose the sex of the baby. The scan is for checking that the baby's anatomy is healthy.'
Scenario 2 — CVS for chromosomal analysis:
A 38-year-old woman at 12 weeks undergoes CVS for chromosomal analysis (indication: advanced maternal age). The karyotype report will include the sex chromosomes. The sex is therefore known at the chromosomal level. Under the Act, the laboratory must not communicate the sex chromosome result in a way that reveals foetal sex — only the chromosomal diagnosis (e.g., 'Karyotype 46,XX — no numerical or structural anomaly detected') may be reported. The genetic counsellor must not say 'The baby is a girl and is chromosomally normal.'
Scenario 3 — Couple insists on knowing the sex:
As in the opening hook: a couple at 20 weeks asks the ultrasonologist to tell them the sex. The correct response is firm, non-apologetic, and non-confrontational: 'I understand your curiosity, and I know this is an exciting time. However, I am legally prohibited from disclosing the sex of the baby — this is required by the PCPNDT Act, and there are no exceptions. The purpose of this scan is to check that your baby is healthy, and I am happy to tell you everything I find about the baby's health.' If the couple persists or becomes aggressive, document the interaction and consider informing the Appropriate Authority if you suspect a complaint may follow.
SELF-CHECK
A genetic laboratory reports a CVS karyotype as '46,XX — no chromosomal abnormality detected' on the report it gives to the referring obstetrician. Under the PCPNDT Act, which of the following is correct?
A. This is an offence — sex chromosomes must not be reported in any form
B. This is acceptable — the chromosomal diagnosis is communicated but the report should not explicitly state 'female' or 'girl'
C. This is an offence only if the couple requested the sex determination
D. The laboratory is not subject to the PCPNDT Act — only ultrasonography clinics are
Reveal Answer
Answer: B. This is acceptable — the chromosomal diagnosis is communicated but the report should not explicitly state 'female' or 'girl'
Genetic laboratories conducting CVS/amniocentesis are covered by the Act. Reporting the karyotype (e.g., 46,XX) as part of a legitimate chromosomal analysis is acceptable, but the report must not translate this into explicit sex disclosure (e.g., 'female' or 'your baby is a girl'). The karyotype itself is part of the diagnostic result — its suppression would compromise the clinical purpose of the analysis. The critical rule is that the information must not be used for sex selection.
CLINICAL PEARL
The most common PCPNDT prosecution scenario is not a deliberate sex-determination service — it is an ultrasonologist who makes an offhand comment during a routine scan ('Everything looks fine — I can see it is a little boy'). This is a violation of the Act regardless of intent. The rule is absolute: no comment about foetal sex, however casual, in any form, to any person. Train yourself to respond to sex-related questions with the same short, consistent script: 'I cannot tell you the sex of the baby by law.' Practise this until it is automatic — it protects you, the institution, and ultimately the girls who might not be born otherwise.
Self-Assessment
You have now covered the entire scope of competency OG20.3 — the historical context, the Act's structure and key provisions (including the 2003 amendment), clinician obligations (registration, Form F, records, communication restrictions), offences and penalties, and applied clinical scenarios. These questions are pitched at the level expected in written exams and viva voce for final-year MBBS. Work through each one independently before checking the answer. The questions on specific penalty figures, Form F requirements, and the boundary between lawful prenatal diagnosis and prohibited sex determination are the most frequently tested — pay close attention to them. Examiners consistently reward candidates who can articulate not just the rule but the reason: the Act's absolute prohibition on communicating foetal sex exists because any exception creates a loophole that defeats the entire purpose of the legislation. Internalise that rationale and the specific provisions will follow logically.
- What is the full formal name of the PCPNDT Act and what year was it enacted? What was the major change introduced by the 2003 amendment?
- Enumerate any four valid indications for prenatal diagnosis under the PCPNDT Act.
- A pregnant woman undergoes amniocentesis for Down syndrome risk assessment. The laboratory finds a 46,XX karyotype. What should the laboratory report state, and what must it NOT state?
- What is Form F? Who fills it, when must it be filled, and for how long must it be retained?
- An obstetrician at a private hospital inadvertently tells a couple that 'the scan shows a healthy baby girl.' What offence has been committed? What is the penalty for a first offence?
Answers:
1. Pre-conception and Pre-natal Diagnostic Techniques (Prohibition of Sex Selection) Act, 1994. The 2003 amendment extended the Act's scope to cover pre-conception sex selection techniques (sperm sorting, embryo selection by sex), renamed it from the PNDT Act to the PC & PNDT Act, and strengthened enforcement mechanisms.
2. Any four from: maternal age >35 years; 2+ previous spontaneous abortions or foetal loss; previous child with chromosomal/metabolic/neural-tube defect; family history of mental retardation; abnormal maternal serum markers; exposure to teratogenic drugs, radiation, infection, or chemicals during pregnancy.
3. The report should state the karyotype finding and diagnostic conclusion (e.g., '46,XX — no numerical or structural chromosomal anomaly detected'). The report must NOT explicitly state 'The baby is a girl' or 'female foetus' in a way that serves sex-disclosure beyond the chromosomal diagnosis. The purpose of amniocentesis was chromosomal analysis, not sex determination.
4. Form F is the compulsory declaration/consent form required under the PCPNDT Act before any prenatal diagnostic procedure. It is filled by the clinician/facility and signed by the pregnant woman. It must be filled before every covered procedure — not once per pregnancy. It must be retained for 2 years and made available to the Appropriate Authority on demand.
5. The offence is communicating the sex of the foetus to the woman or her relatives — a violation of Section 5 of the Act. First offence penalty: imprisonment up to 3 years AND fine up to Rs. 10,000; the obstetrician's name is removed from the medical register.