Page 1 of 24
OG28.1 | Infertility Evaluation and Management — SDL Guide
Learning Objectives
- Define infertility and distinguish primary from secondary infertility using the standard 12-month criterion
- Enumerate the major causes of infertility and their approximate relative contributions
- Interpret semen analysis using WHO 2021 reference values and identify specific abnormalities
- Outline the stepwise investigation of the infertile couple including ovulatory assessment, tubal patency, and hormonal profile
- Describe cause-specific management principles including ovulation induction, surgical options, and assisted reproduction
INSTRUCTIONS
Infertility affects approximately one in six couples globally and is one of the most emotionally and medically complex presentations in gynaecological practice. For final-year students, this SDL equips you to take a systematic history from both partners, interpret key investigations including semen analysis and hormonal profiles, and counsel couples on cause-specific management pathways — skills directly tested in clinical assessments and the foundation for referral decisions in primary and secondary care.
References
- DC Dutta's Textbook of Gynaecology, 8th edition, Ch 18 (Infertility) (textbook)
- Shaw's Textbook of Gynaecology, 17th edition, Ch 23 (textbook)
- WHO Laboratory Manual for Human Semen Examination and Processing, 6th edition (WHO 2021) (guideline)
- NICE Fertility Guideline CG156, updated 2017 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Priya and Suresh, both in their early thirties, have been married for two years. They report regular, unprotected intercourse but Priya has not conceived. Her cycles are irregular — sometimes 45 days, sometimes 60 — and she has noticed increasing facial hair over the past year. Suresh works in a textile factory and has smoked since his teens. They have been told by friends to 'just relax', but have come to your OPD seeking answers. As the attending clinician, your first task is to conduct a structured evaluation of both partners simultaneously — because infertility is always a couple's diagnosis, not one partner's burden.
WHY THIS MATTERS
Infertility is defined as the failure to achieve a clinical pregnancy after 12 months of regular, unprotected sexual intercourse. It affects approximately 10–15% of couples of reproductive age worldwide and represents one of the leading causes of gynaecological consultation. In India, estimates suggest 10–15% of married couples are affected at some point, with significant psychological, social, and economic consequences. As a final-year student entering clinical practice, you will encounter infertile couples at every level of care — primary health centres, district hospitals, and tertiary referral units. The ability to take a systematic couples history, order the right first-line investigations, and initiate or appropriately refer cause-specific management is a core competency. Understanding the full landscape of causes — from a simple anovulatory cycle to male-factor azoospermia — is what enables you to approach every case without missing a treatable diagnosis.
RECALL
Before proceeding, recall from your Physiology studies: the hypothalamic-pituitary-gonadal (HPG) axis drives both ovulation and spermatogenesis. GnRH from the hypothalamus stimulates pituitary release of FSH and LH. In women, FSH drives follicular development and oestrogen secretion; the LH surge triggers ovulation; progesterone from the corpus luteum sustains the luteal phase. In men, FSH supports Sertoli cells and spermatogenesis; LH stimulates Leydig cells to produce testosterone. Any disruption at hypothalamic, pituitary, gonadal, or end-organ level can impair fertility in either sex. Also recall from Anatomy: the uterine tubes travel from the uterine cornua to the ovaries — tubal patency is essential for sperm–egg transport and fertilisation. The uterine cavity must be anatomically normal for implantation.
Clinical Presentation of the Infertile Couple
Infertility is the failure to achieve a clinical pregnancy after 12 months of regular, unprotected sexual intercourse. The 12-month threshold is shortened to 6 months in women aged over 35 years, because declining ovarian reserve and reduced conception rates with age justify earlier investigation and intervention. Primary infertility describes the situation where the couple has never achieved a clinical pregnancy, whereas secondary infertility refers to failure to conceive after a previous clinical pregnancy — regardless of whether that pregnancy resulted in a live birth, miscarriage, or ectopic pregnancy. This distinction is clinically important: secondary infertility implies prior fertility potential and often points to an acquired cause such as pelvic inflammatory disease, post-surgical adhesions, or a new-onset male factor.
The evaluation must always begin with a thorough history from both partners together, as approximately 40% of infertility is attributed to male factors, 40% to female factors, and 20% involves combined or unexplained causes. A single-partner focus misses a significant proportion of diagnoses from the outset.
Female history should cover menstrual pattern (cycle length, regularity, dysmenorrhoea, intermenstrual bleeding), contraceptive history, previous pregnancies and their outcomes, sexual history (frequency and timing of intercourse, dyspareunia), symptoms suggesting specific diagnoses (pelvic pain, deep dyspareunia in endometriosis; hirsutism, weight gain, irregular cycles in PCOS; hot flushes and night sweats in premature ovarian insufficiency), past pelvic infections, pelvic or abdominal surgeries, and systemic illnesses (thyroid disease, hyperprolactinaemia, diabetes).
Male history covers previous paternity (establishes prior fertility), past medical history (orchitis, undescended testes, scrotal or inguinal surgery, sexually transmitted infections), occupational exposures (heat, pesticides, radiation, solvents), lifestyle factors (cigarette smoking, alcohol, anabolic steroids, cannabis — all adversely affect spermatogenesis), and any symptoms of hypogonadism (reduced libido, erectile dysfunction).
Physical examination of the woman includes BMI (both underweight and obesity affect ovulation), signs of hyperandrogenism (acne, hirsutism, clitoromegaly), thyroid palpation, and bimanual pelvic examination for uterine size/mobility and adnexal pathology. Examination of the man includes scrotal examination for testicular volume (normal ≥15 mL by Prader orchidometer), consistency, varicocele (bag-of-worms feel on standing, more common on left), and epididymal tenderness.
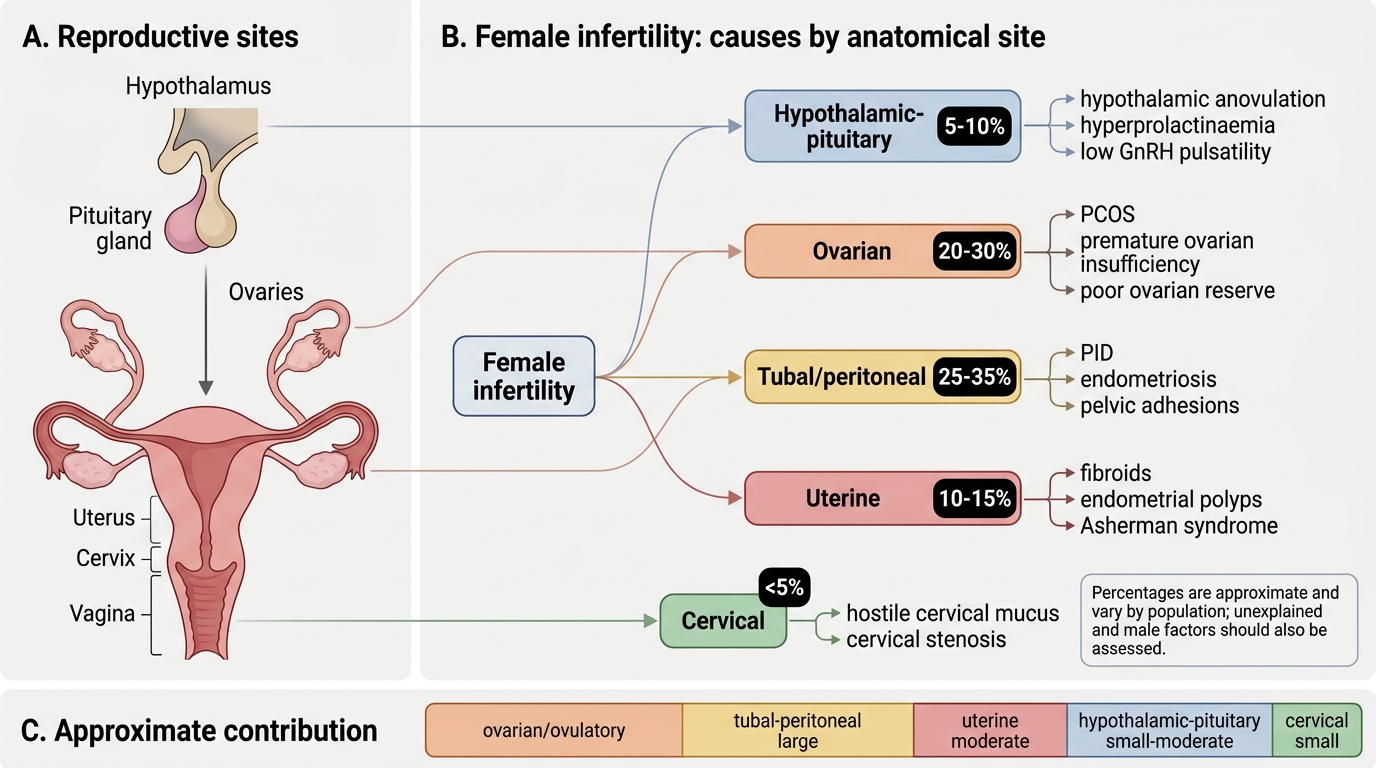
Causes of Female Infertility by Anatomical Site
Pathophysiology and Causes of Infertility
Infertility arises from disruption at any step of the reproductive cascade: folliculogenesis and ovulation, sperm production and transport, fertilisation in the fallopian tube, early embryo development, and implantation in a receptive endometrium. Understanding which step is disrupted guides investigation and treatment.
Female causes are conventionally categorised by anatomical site or physiological system.
Ovulatory dysfunction accounts for approximately 25–35% of female infertility. The most common cause is polycystic ovary syndrome (PCOS), characterised by chronic anovulation, hyperandrogenism, and polycystic ovarian morphology on ultrasound. Pathophysiology involves insulin resistance driving excess LH and androgen secretion, which arrests follicular development at the antral stage. Hypothalamic amenorrhoea (functional — due to excessive exercise, low BMI, or psychological stress) suppresses GnRH pulsatility, leading to low FSH, low LH, and anovulation. Hyperprolactinaemia (from prolactinoma or drugs such as metoclopramide, antipsychotics) suppresses GnRH via dopaminergic pathways. Premature ovarian insufficiency (POI) — hypergonadotrophic hypogonadism before age 40 — causes anovulation with elevated FSH (>25 IU/L on two occasions) and reduced AMH, due to follicular depletion (idiopathic, autoimmune, chromosomal, iatrogenic).
Tubal and peritoneal factors account for 25–35% of female infertility. Pelvic inflammatory disease (PID) caused by Chlamydia trachomatis and Neisseria gonorrhoeae is the leading cause of tubal damage: peritubal adhesions, hydrosalpinx, and intraluminal scarring block sperm or egg transport and impair ciliary function. Endometriosis causes peritubal and periovarian adhesions, alters the peritoneal fluid environment, impairs oocyte quality, and may affect implantation through immunological mechanisms. Previous pelvic or abdominal surgery (appendicectomy, ovarian cystectomy) can produce adhesions that distort tubal anatomy.
Uterine factors account for approximately 10–15% of cases. Submucous fibroids distort the endometrial cavity and impair implantation. Endometrial polyps may mechanically block the fallopian tube ostia or alter the implantation environment. Asherman syndrome (intrauterine adhesions) — typically following overzealous curettage — reduces endometrial receptivity and may cause secondary infertility and hypomenorrhoea.
Cervical factors are less common (<5%) and include hostile cervical mucus (inadequate in consistency or volume at mid-cycle due to prior surgery, infection, or antisperm antibodies) that impedes sperm penetration.
Male causes account for approximately 40% of all infertility:
| Category | Examples | Pathophysiology |
|---|---|---|
| Pre-testicular | Hypogonadotrophic hypogonadism (Kallmann, pituitary tumours), hyperprolactinaemia, anabolic steroids | Low FSH/LH → impaired spermatogenesis |
| Testicular | Varicocele (most common surgically correctable cause), orchitis (mumps), undescended testes, Klinefelter syndrome (47,XXY), idiopathic | Impaired spermatogenesis, raised scrotal temperature, genetic |
| Post-testicular | Obstructive azoospermia (CBAVD in CF, vasectomy, epididymal obstruction), retrograde ejaculation | Sperm produced but not delivered |
Unexplained infertility is diagnosed in approximately 15–30% of couples after full investigation reveals no identifiable cause. It likely represents subtle defects in sperm function, oocyte quality, fertilisation, or implantation not detectable with standard tests.
SELF-CHECK
A 28-year-old woman presents with infertility for 18 months. She has cycles every 45–60 days, hirsutism, and an elevated LH:FSH ratio. Her partner's semen analysis is normal. What is the most likely cause of her infertility?
A. Hypothalamic amenorrhoea due to low body weight
B. Polycystic ovary syndrome causing anovulation
C. Premature ovarian insufficiency
D. Tubal factor due to prior PID
Reveal Answer
Answer: B. Polycystic ovary syndrome causing anovulation
Irregular long cycles, hirsutism, and elevated LH:FSH ratio are classic features of PCOS, the most common cause of anovulatory infertility. Hypothalamic amenorrhoea would show low LH and FSH. POI would show elevated FSH with low AMH and estrogen. Tubal factor would not explain the hormonal and androgen abnormalities.
Systematic Investigation of the Infertile Couple
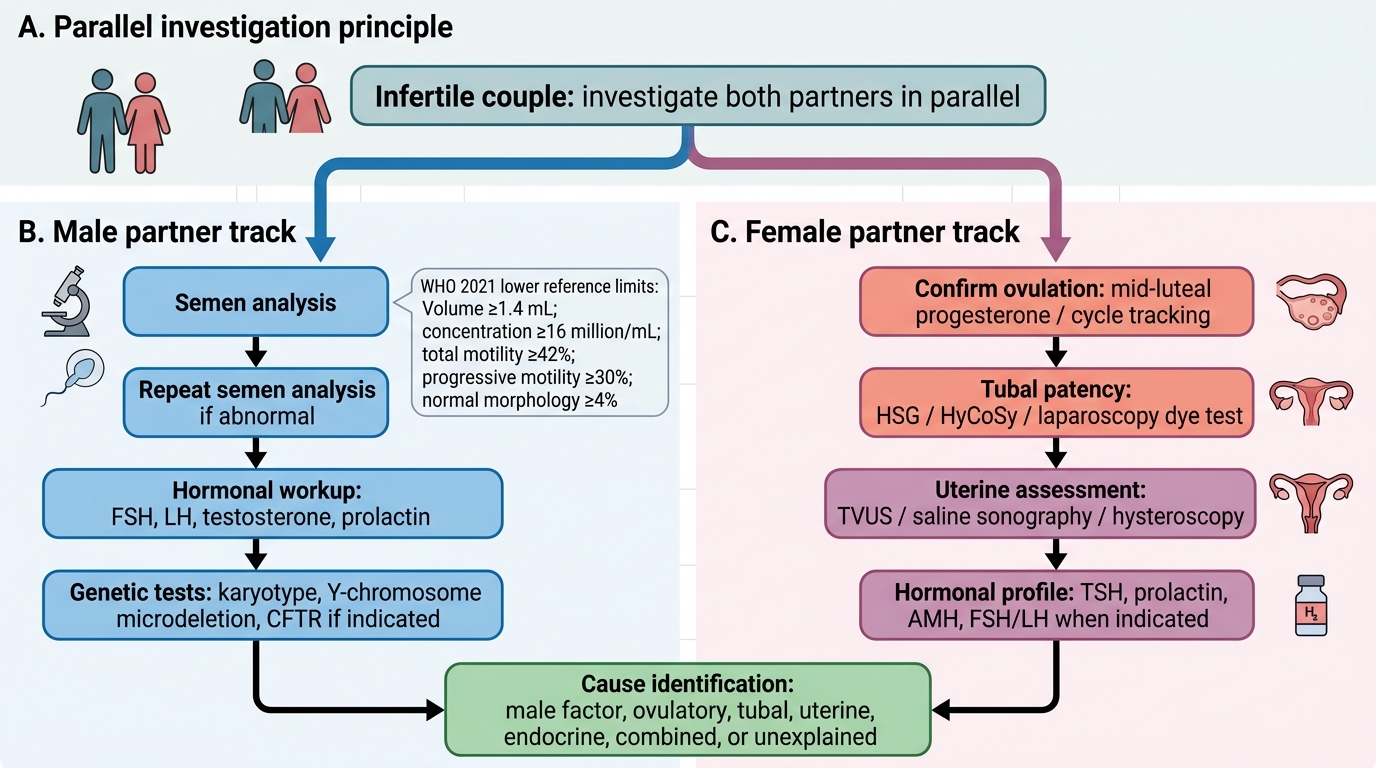
Investigation of infertility follows a structured, stepwise approach addressing each partner simultaneously. The goal is to identify all contributing causes before initiating treatment, because mixed-cause infertility (both partners contributing) is common and treatment targeting only one cause produces suboptimal outcomes.
Semen analysis is the first and most important male investigation. A single abnormal result is not sufficient — two samples collected 2–7 weeks apart after 2–7 days of abstinence are required to confirm any abnormality. The WHO 2021 Laboratory Manual (6th edition) defines the lower reference limits (5th centile of fertile men within 12 months of conception): volume ≥1.4 mL, total sperm number per ejaculate ≥39 million, sperm concentration ≥16 million/mL, total motility ≥42%, progressive motility ≥30%, and normal morphology ≥4% (Tygerberg strict criteria). Abnormalities are named systematically: oligospermia (low count), asthenospermia (poor motility), teratospermia (poor morphology), azoospermia (no sperm), and combined designations (oligo-astheno-teratospermia, OAT).

Provided image
Ovulation confirmation is assessed by:
- Mid-luteal serum progesterone on day 21–23 of a 28-day cycle (or 7 days before expected period in irregular cycles): >10 nmol/L (approximately >3.2 ng/mL) confirms ovulation. Values >30 nmol/L are considered a strong positive by some centres.
- Serial transvaginal ultrasound (follicle tracking): monitors dominant follicle growth (≥18 mm pre-ovulatory), collapse post-rupture, and corpus luteum formation — the most direct confirmation.
- LH urine kits detect the mid-cycle LH surge 24–36 hours before ovulation (useful for timing but does not confirm actual ovulation).
- Endometrial biopsy (secretory pattern on histology) is now rarely used for ovulation confirmation due to poor reproducibility.
Hormonal profile (day 2–3 of cycle): FSH and LH (detect hypergonadotrophic or hypogonadotrophic state; elevated FSH >10 IU/L suggests poor reserve), oestradiol, AMH (anti-Müllerian hormone) — cycle-independent marker of ovarian reserve; <1.0 ng/mL indicates diminished reserve. Antral follicle count (AFC) on USS: <7 total follicles suggests poor response. Thyroid function (TSH) and prolactin are checked in all women, as hypothyroidism and hyperprolactinaemia are easily treated causes of anovulation.
Tubal patency is assessed by hysterosalpingography (HSG), saline/contrast sonohysterography (SSG/HyCoSy), or diagnostic laparoscopy with dye (chromopertubation) — covered in detail in the Tubal Patency Assessment SDL.
Uterine cavity assessment: hysteroscopy (gold standard for intrauterine pathology), sonohysterography, or transvaginal ultrasound detect fibroids, polyps, and adhesions.
Post-coital test (PCT) — traditionally assessing sperm penetration into cervical mucus within 9 hours of intercourse — has fallen out of routine use due to poor reproducibility and limited predictive value; it is no longer recommended in standard algorithms.
Stepwise Investigation Algorithm for the Infertile Couple
SELF-CHECK
According to WHO 2021 reference values, which of the following correctly describes a normal semen analysis?
A. Volume ≥2.0 mL, concentration ≥20 million/mL, progressive motility ≥50%
B. Volume ≥1.4 mL, concentration ≥16 million/mL, total motility ≥42%, normal morphology ≥4%
C. Volume ≥1.5 mL, concentration ≥15 million/mL, normal morphology ≥14%
D. Volume ≥2.0 mL, concentration ≥20 million/mL, normal morphology ≥30%
Reveal Answer
Answer: B. Volume ≥1.4 mL, concentration ≥16 million/mL, total motility ≥42%, normal morphology ≥4%
The WHO 2021 (6th edition) lower reference limits (5th centile of fertile men) are: volume ≥1.4 mL, concentration ≥16 million/mL, total motility ≥42%, progressive motility ≥30%, and normal morphology ≥4% (Tygerberg strict criteria). Options A and D use older WHO 2010 values. Option C uses incorrect morphology threshold of 14% (the strict Tygerberg criterion is ≥4%).